0829
Improved Quantitative Diffusion in Fetal Lungs with Multiecho EPI Distortion and Motion Correction1Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 2Maternal Fetal Care Center, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
Keywords: Fetal, Fetus, fetal lung, diffusion, distortion correction
Motivation: Accurately assessing fetal lung maturity and development with quantitative diffusion parameters could guide critical care for at-risk fetuses, but has been severely limited by artifacts.
Goal(s): Develop an MRI technique to enable reliable diffusion imaging of fetal lungs.
Approach: Investigated a multi-echo spin echo sequence to provide motion/distortion correction.
Results: The technique improved lung analysis, in particular, resulting in more consistent ADC fitting. The method also increased the geometric fidelity of the diffusion image with structural images.
Impact: This work demonstrates a novel MRI technique to enable reliable diffusion imaging of fetal lungs, overcoming current barriers of motion and artifacts. Improving lung maturity assessment during pregnancy has the potential to transform care for at-risk fetuses through earlier interventions.
Introduction
Diffusion-weighted magnetic resonance imaging (DW-MRI) has shown promise in evaluating fetal lung maturation. Studies have demonstrated that apparent diffusion coefficients (ADC) from DW-MRI can provide a non-invasive biomarker for pulmonary structural maturation with a strong correlation to histological markers during tissue development.1 The ADC values of fetal lungs have been found to show a strong association with gestational age, increasing dramatically between 16 and 27 weeks and then achieving a plateau around 27 weeks.2 However, fetal and maternal motion, along with secondary effects such as susceptibility artifacts, limit the success rate of DWI acquisition and reduce the robustness of quantitative markers such as ADC in fetal lungs. For instance, in the study by Afacan et al., it was reported that nearly 40% (26 out of 65 cases) had severe motion artifacts, preventing the assessment of lung maturity with DWI in those fetuses.This major drawback effectively limits clinical translation of quantitative DWI biomarkers for the fetal lungs, such as in congenital diaphragmatic hernia (CDH) assessment. In the context of imaging uncooperative children and fetuses, dual-echo spin-echo diffusion MRI sequence has been shown to improve the success rate of brain diffusion scans as it provides rapid distortion information for each slice.3-5 Here, we investigated the efficacy of an extended multi-echo spin echo EPI sequence improving on the dual-echo approach and enabling diffusion-weighted MRI analysis in the fetal lungs.
Methods
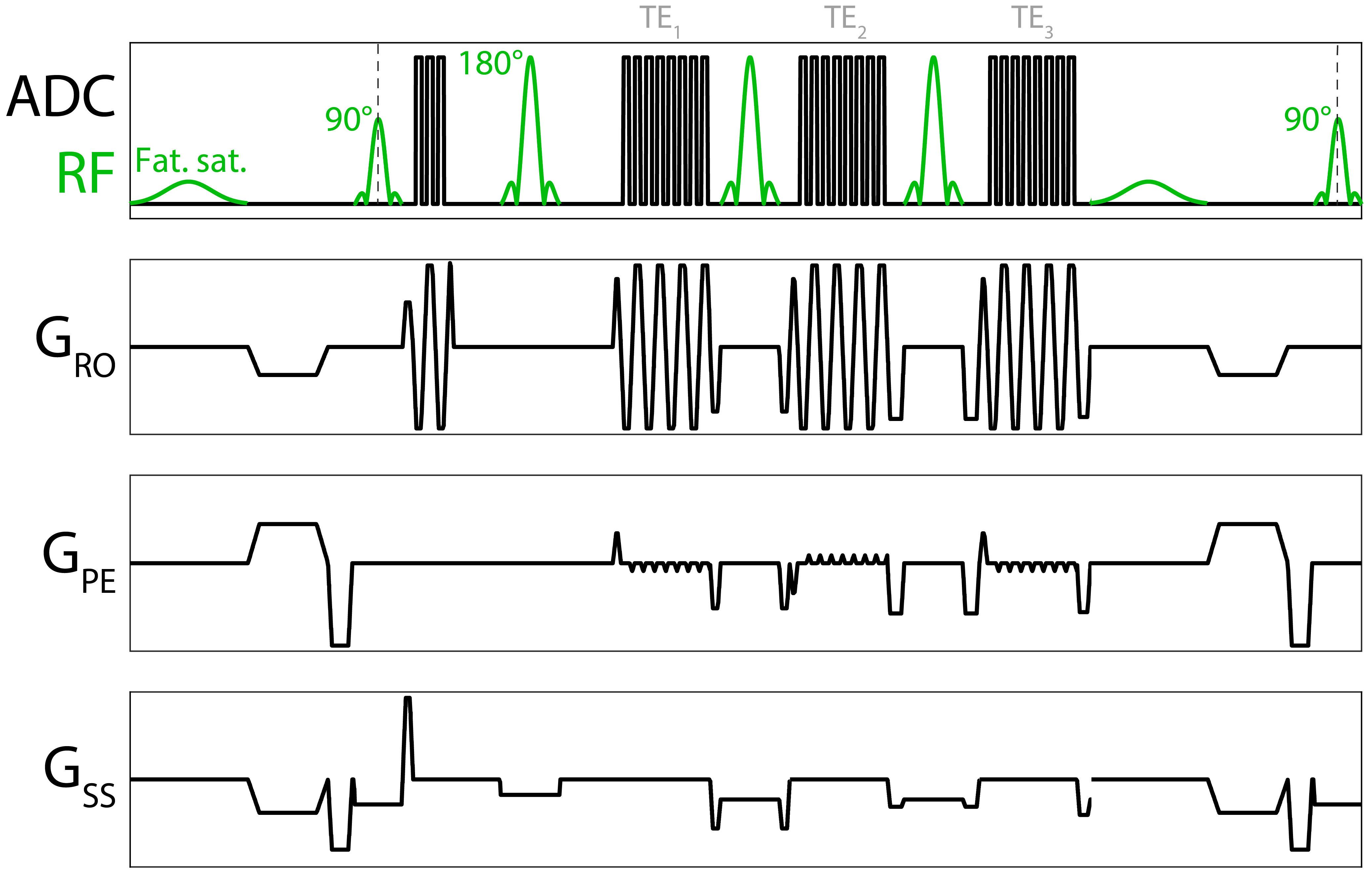
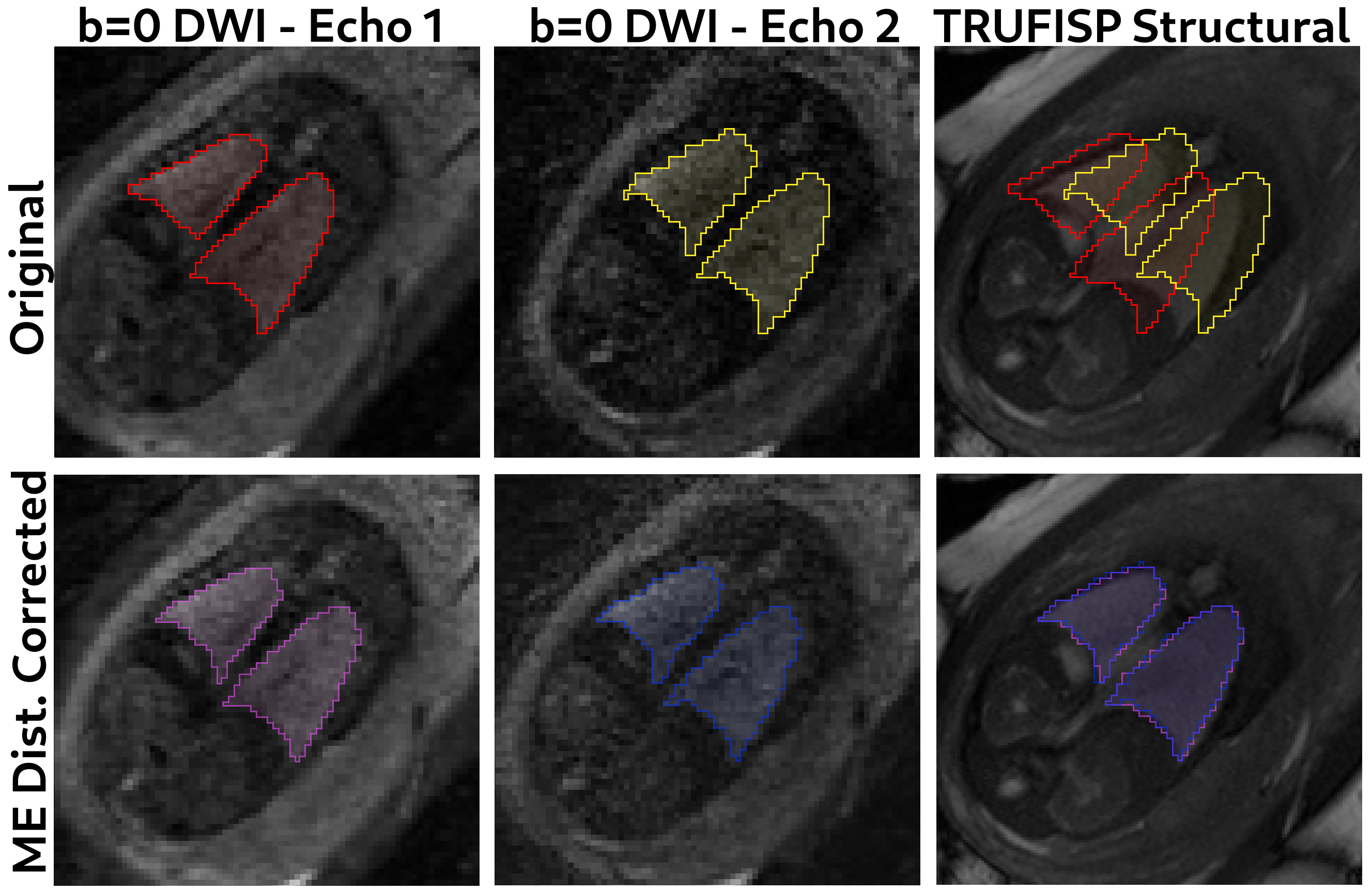
We have modified a standard spin-echo EPI sequence with additional readouts matching the first readout in resolution, field-of-view and bandwidth but with alternating k-space traversal. A 180-degree refocusing pulse and spoiler gradients generated the second and third echoes. Figure 1 shows the pulse sequence diagram for the sequence. The images were distortion-corrected using FSL’s TOPUP algorithm6 implementation on the basis of individual slices. To avoid artifacts due to signal decay across echoes, the first and third echoes were averaged to create an image that matches the contrast of the second echo but with opposing polarity. Using these, a field map was generated for each slice, which was then applied back to each individual echo.These geometrically corrected slices at each b-value were then fed into a slice-to-volume reconstruction algorithm implemented in SVRtk.7 When reconstructing the volume for each echo, the other echoes were used as multichannel inputs to improve the guidance of each slice to the full volume space. Finally, ADC and predicted signals at each b-value were calculated using a singular-value-decomposition-based algorithm via custom code implemented with the pytorch python library.
MRI acquisition: Multi-echo, spin-echo sequence with 2x2x4mm, TE of 52ms, 97ms and 120ms, IPAT of 2, coronally. 9 b-values; [0 10 30 50 100 200 400 600 800]. We acquired data from 6 pregnant healthy volunteers with IRB consent. Gestational ages for the fetuses were 32.8+-2.8 weeks.
Results
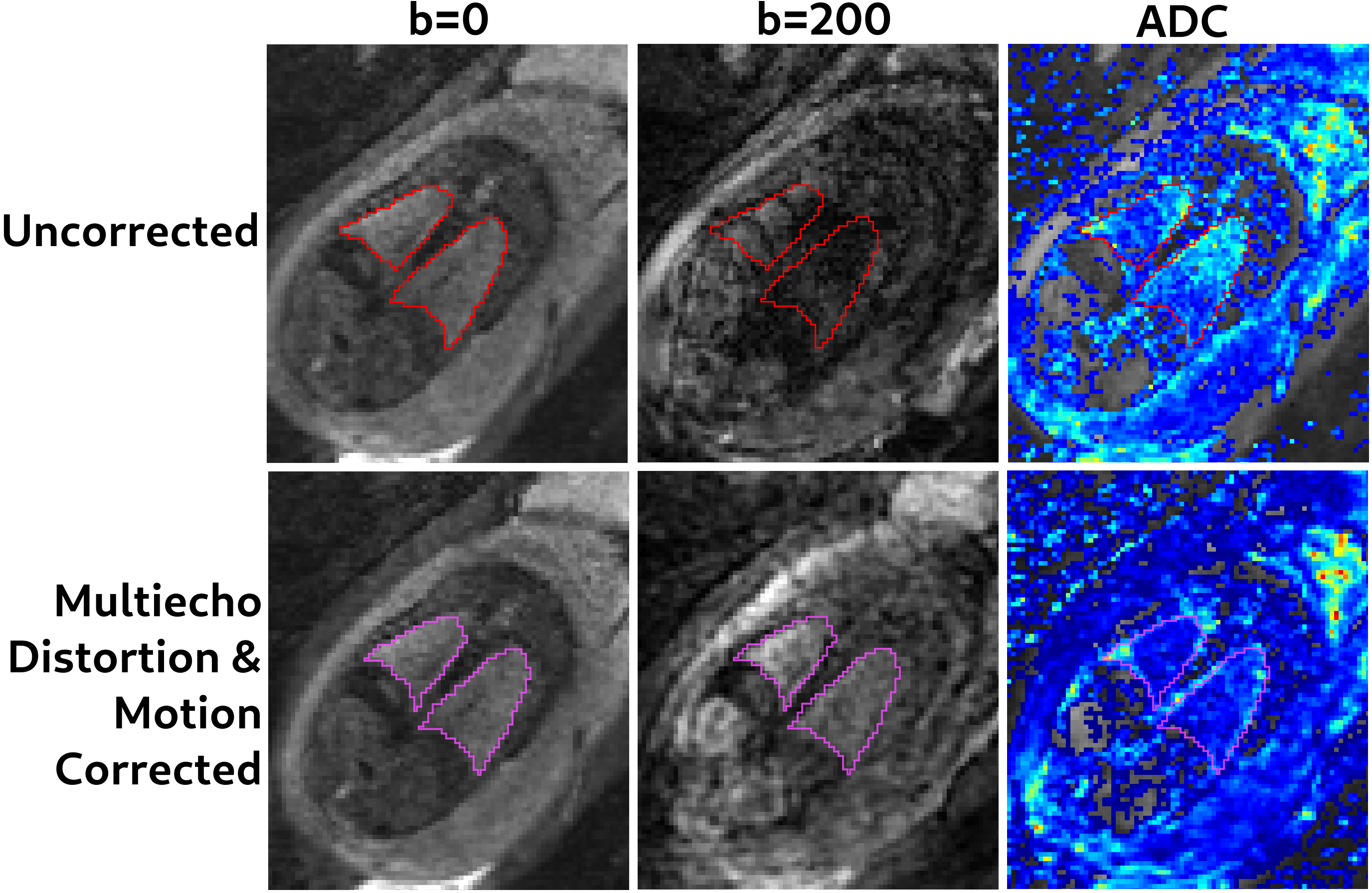
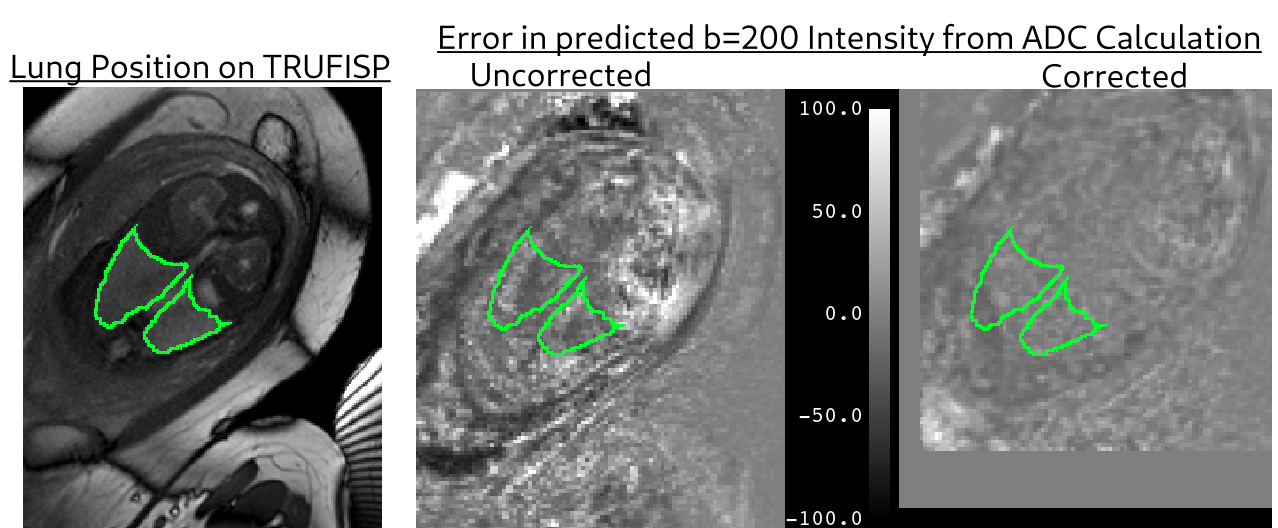
Using the contrast-matching approach with the alternating phase encoding multi-sequence allowed both distortion correction and motion correction of individual slices, even in the presence of fetal motion as outlined in Figure 1. Figure 2 demonstrates the effectiveness of our multi-echo diffusion sequence in rectifying distortions and enhancing the geometric accuracy of the diffusion-weighted images. The right panel illustrates the improved match with structural images between images acquired and corrected using our technique compared to single echo images. Figure 3 showcases the application of a slice-to-volume registration algorithm using SVRTK, enabling motion correction on a slice-by-slice basis across different b values. Specifically, the image of a slice at b=200 initially misaligned in the original image, is successfully registered to the b=0 image. This correction is achieved by leveraging multiple echoes during the distortion correction process. Figure 4 displays sample ADC maps and the corresponding fit errors from the ADC fits. Notably, the error figure demonstrates a reduction in fit errors when our motion and distortion correction sequence was applied, indicating the efficacy of the correction method in improving the accuracy of the fits.Discussion
Overall, our study demonstrates a promising approach to overcome the challenges associated with fetal lung DW-MRI. By employing a multi-echo sequence and advanced post-processing techniques, we have significantly improved the quality and accuracy of diffusion-weighted images, making them more suitable for assessing fetal lung development. These advancements hold significant potential, particularly in the context of conditions like CDH, where accurate evaluation of lung maturity is critical for guiding clinical interventions and improving outcomes. Further research and validation in larger cohorts will be essential to establish the clinical utility and broader applicability of our proposed methods, as well as extend this analysis to cover the intravoxel incoherent motion imaging model.8Acknowledgements
This work was supported partially by the NIDDK, NIBIB, NINDS and NLM of the National Institutes of Health under award numbers R01DK125561, R21DK123569, R21EB029627, R01NS121657, R01LM013608, R01EB032366-02, 5R01HD109395-02 and by the grant number 2019056 from the United States-Israel Binational Science Foundation (BSF).References
1. Higano NS, Cao X, Guo J, Wang X, Kroenke CD,
Filuta AL, Bridges JP, Woods JC. Fetal lung development via quantitative
biomarkers from diffusion MRI and histological validation in rhesus
macaques. J Perinatol. 2022 Jul;42(7):866-872. doi:
10.1038/s41372-021-01236-x. Epub 2021 Oct 22. PMID: 34686834; PMCID:
PMC9023595.
2. Afacan, Onur, Ali Gholipour, Robert V. Mulkern, Carol E. Barnewolt, Judy A. Estroff, Susan A. Connolly, Richard B. Parad, Sigrid Bairdain, and Simon K. Warfield. “Fetal Lung Apparent Diffusion Coefficient Measurement Using Diffusion-Weighted MRI at 3 Tesla: Correlation with Gestational Age: Fetal Lung Diffusion MRI.” Journal of Magnetic Resonance Imaging 44, no. 6 (December 2016): 1650–55. https://doi.org/10.1002/jmri.25294.
3. Afacan, Onur, W. Scott Hoge, Tess E. Wallace, Ali Gholipour, Sila Kurugol, and Simon K. Warfield. “Simultaneous Motion and Distortion Correction Using Dual‐Echo Diffusion‐Weighted MRI.” Journal of Neuroimaging 30, no. 3 (May 2020): 276–85. https://doi.org/10.1111/jon.12708.
4. Gallichan, D., Andersson, J.L., Jenkinson, M., Robson, M.D. and Miller, K.L., 2010. Reducing distortions in diffusion‐weighted echo planar imaging with a dual‐echo blip‐reversed sequence. Magnetic resonance in medicine, 64(2), pp.382-390
5. Hutter, J., Christiaens, D.J., Schneider, T., Cordero-Grande, L., Slator, P.J., Deprez, M., Price, A.N., Tournier, J.D., Rutherford, M. and Hajnal, J.V., 2018. Slice-level diffusion encoding for motion and distortion correction. Medical image analysis, 48, pp.214-229
6. Andersson, Jesper L.R., Stefan Skare, and John Ashburner. “How to Correct Susceptibility Distortions in Spin-Echo Echo-Planar Images: Application to Diffusion Tensor Imaging.” NeuroImage 20, no. 2 (October 2003): 870–88. https://doi.org/10.1016/S1053-8119(03)00336-7.
7. Uus, Alena, Tong Zhang, Laurence H. Jackson, Thomas A. Roberts, Mary A. Rutherford, Joseph V. Hajnal, and Maria Deprez. “Deformable Slice-to-Volume Registration for Motion Correction of Fetal Body and Placenta MRI.” IEEE Transactions on Medical Imaging 39, no. 9 (September 2020): 2750–59. https://doi.org/10.1109/TMI.2020.2974844.
8. Jakab,
A., Tuura, R.L., Kottke, R., Ochsenbein‐Kölble, N., Natalucci, G.,
Nguyen, T.D., Kellenberger, C. and Scheer, I., 2018. Microvascular
perfusion of the placenta, developing fetal liver, and lungs assessed
with intravoxel incoherent motion imaging. Journal of Magnetic Resonance Imaging, 48(1), pp.214-225
Figures