0818
T2* relaxometry of Fetal Brain Tissues using Low Field MRI1Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Department of Women and Children’s Health, St Thomas’ Hospital, King's College London, London, United Kingdom, 4Smart Imaging Lab, Radiological Institute, University Hospital Erlangen, Erlangen, Germany
Synopsis
Keywords: Fetal, Fetus
Motivation: The complex and rapid changes during human brain development call for a matched analysis of both structure and function. T2* relaxometry delivers non-invasive insights and pairs well with low field MRI. However, regional assessment is currently lacking.
Goal(s): Investigate the ability of low field MRI to quantify regional fetal brain T2*.
Approach: We acquired dynamic multi-echo gradient-echo sequences at 0.55T and developed automatic high-resolution reconstruction and segmentation to obtain the mean T2* values of 7 individual brain tissues.
Results: Fetal brain tissues vary both in absolute T2* value and in progression have differing T2* values and growth curves throughout gestation.
Impact: Regional fetal brain T2* values, obtained with an automatic pipeline, match the complexity, speed of change and growth during early human brain development and thus carry the potential to play a significant role in future research studies and clinical monitoring.
Introduction
Fetal MRI provides fascinating insights into early human development and particularly the dramatic changes in growth and complexity in the human brain. It plays an important complementary role in antenatal diagnosis and monitoring. In addition to anatomical, T2-weighted imaging, functional contrasts such as T2* relaxometry allow to study tissue properties in-vivo, with for example reduced mean whole brain T2* shown in cases with placental insufficiency1,2. However, this mean assessment does not match the complexity, speed of changes and requirement to assess small structures such as the subplate during fetal brain development.Recent improvements in post-processing tools such as slice-to-volume reconstructions have enabled the analysis of finer and finer structures in anatomical MRI. They exploit redundancies in multiple, individually motion-corrupted volumes3,4 to obtain high quality static 3D reconstructions. Furthermore, re-emerging low field fetal MRI5–7 on clinical 0.55T scanners pairs well with fetal T2* relaxometry: The longer intrinsic T2* at low field increases the dynamic range and allows to study even structures with low T2* such as deep grey matter in the brain.
This work combines both recent advances and shows T2* assessment of 7 brain regions in low field fetal MRI, presenting normal curves, thus paving the way for future application in research studies and for clinical assessment.
Methods
Fetal MRI was acquired as part of an ethically approved study (REC 19/LO/0852) between May 2022 and Oct 2023 at St Thomas’ Hospital, in London, UK on a clinical 0.55T scanner (MAGNETOM Free.Max, Siemens Healthcare) using a 6-element blanket coil and a 9-element spine coil built into the table scanner.The protocol included, among other sequences, both anatomical HASTE imaging and T2* relaxometry: 2D Half-Fourier Acquisition Single-shot Turbo spin Echo Imaging (HASTE) images were acquired in six whole uterus and three fetal brain stacks (FOV=450x450, resolution=1.5x1.5x4.5mm, TR=2500ms, TE=106ms). Dynamic multi-echo gradient-echo echo planar imaging (MEGE-EPI) sequences were acquired for T2* mapping with a resolution of 3mm isotropic, FOV=400x400mm2, GRAPPA=2, TE=[42, 107, 172]ms; TR=10,420ms, number of dynamics=20.
Structural fetal brain reconstructions were obtained from the HASTE stacks using in-house fully automated rigid slice-to-volume reconstructions in SVRTK8,9 after retraining on low field data. Multi-channel fetal brain rigid reconstructions3,10 were created for each echo in the MEGE-EPI image using all the dynamics without motion artefacts and T2* maps were calculated using an in-house python tool10. The MEGE-EPI reconstructions were registered to the corresponding structural brain reconstruction to bring the MEGE-EPI reconstructions and T2* maps into the standard imaging planes3. The third echo reconstruction was then segmented using BOUNTI11 into 19 different labels, which were combined into the following 7 categories: external cerebrospinal fluid (eCSF), grey matter (GM), white matter (WM), deep GM, ventricles, cerebellum and vermis, and brainstem. Brain tissue specific T2* mean values were calculated and changes across gestational age were explored in healthy subjects above 23 gestational weeks.
Results
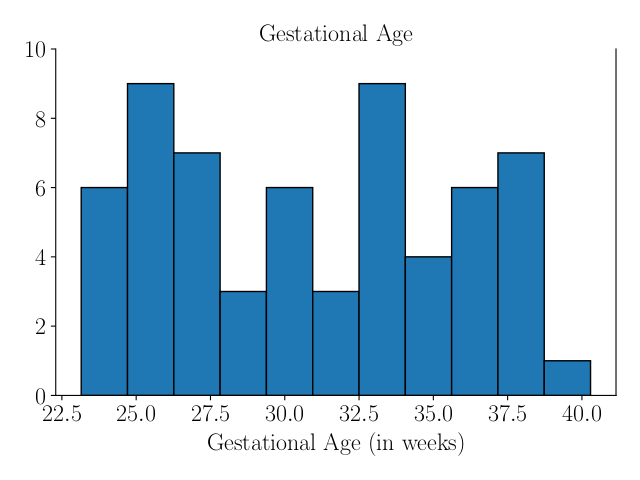
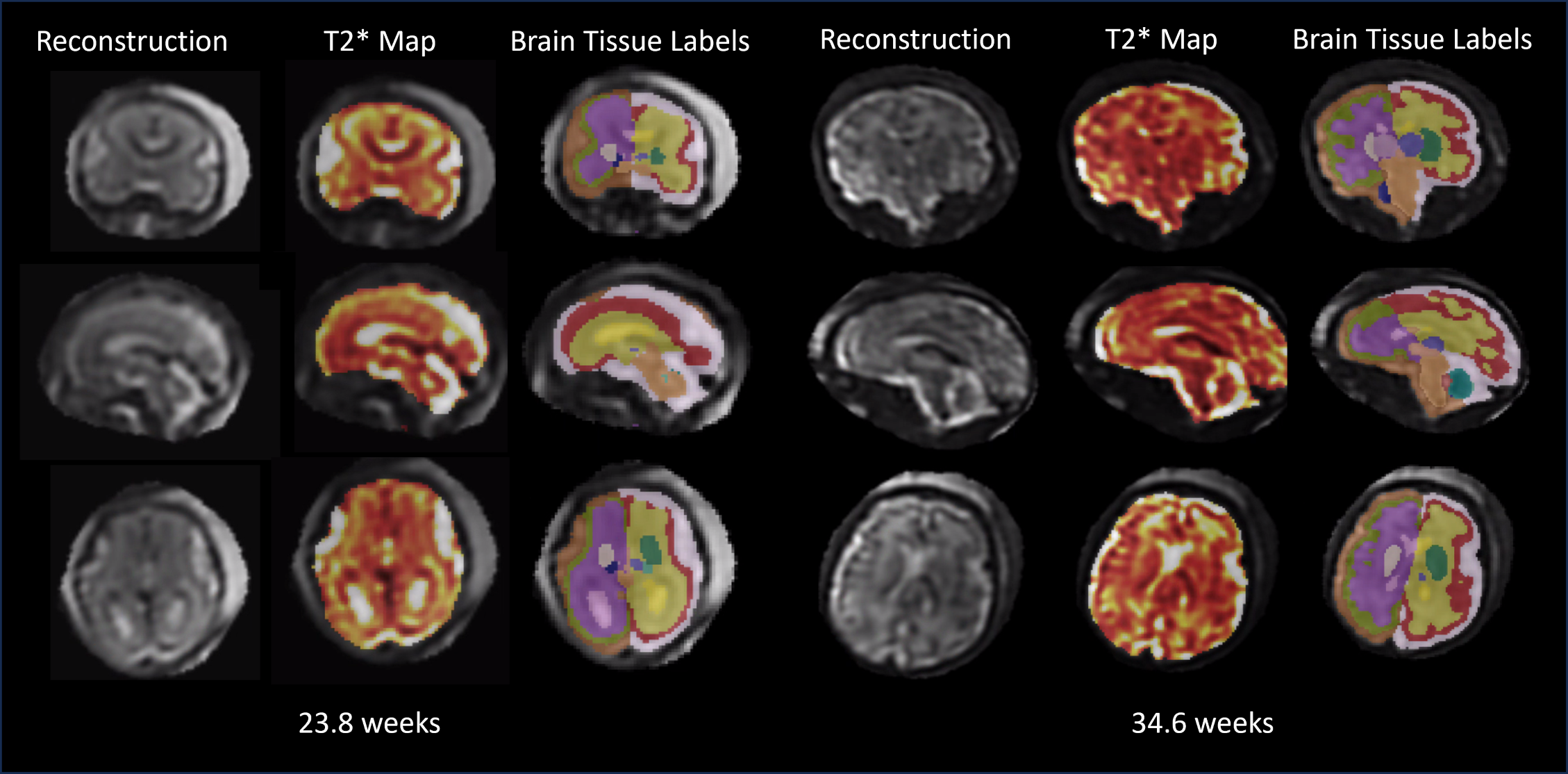
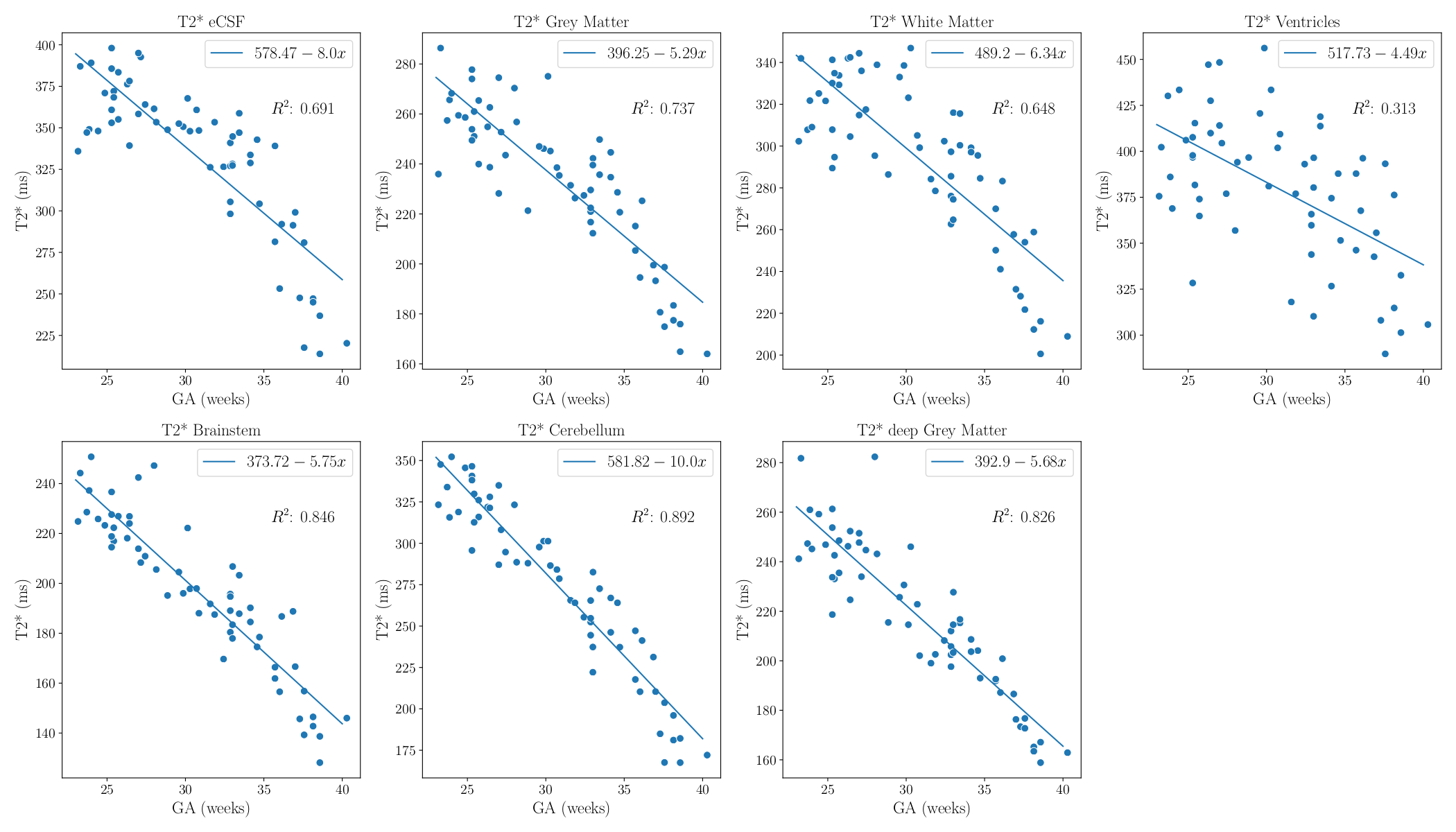
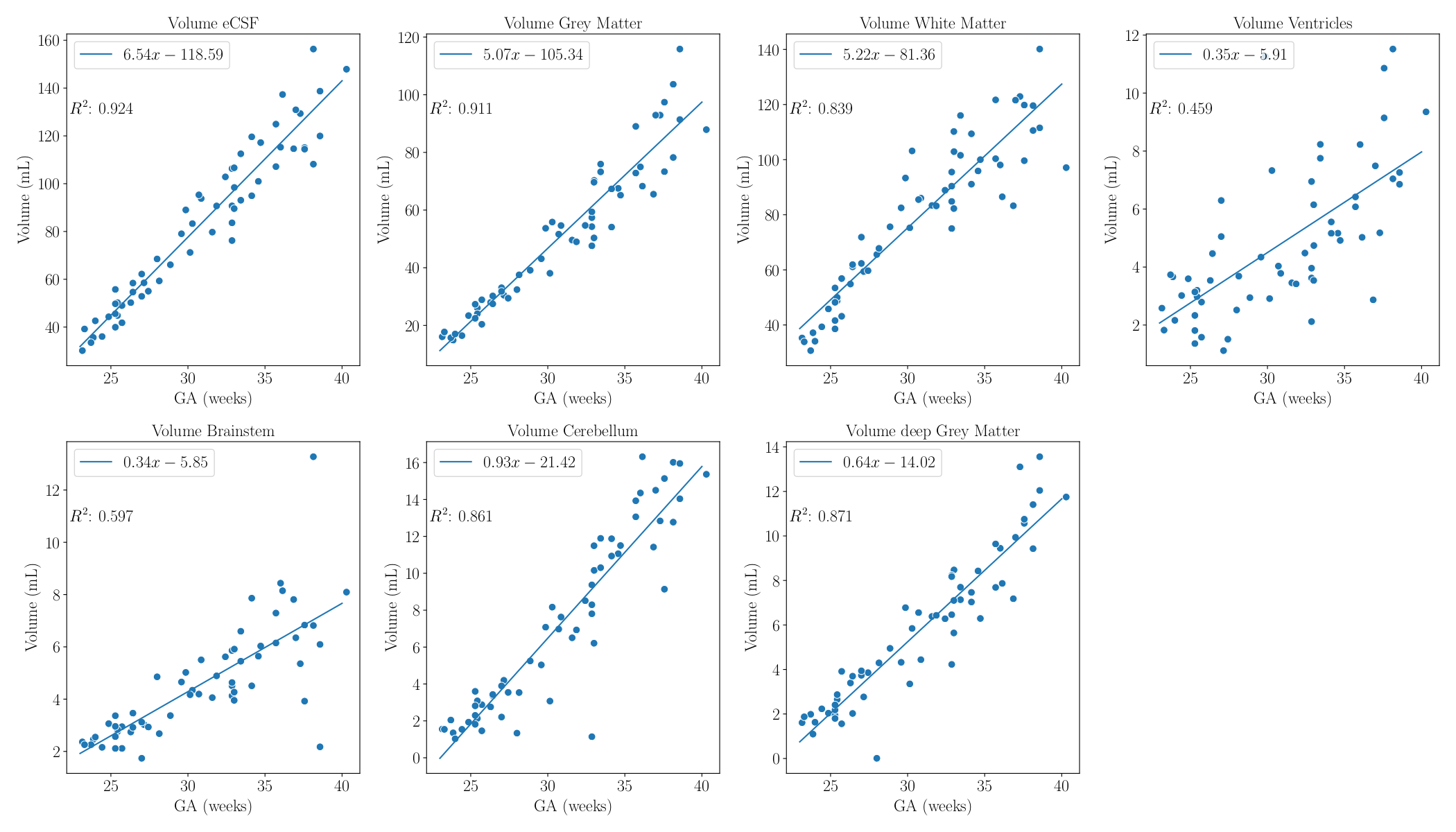
82 healthy fetuses (23-40 gestational weeks, see Figure 1) had both structural brain scans and dynamic MEGE-EPI scans, 61 of which had a good quality reconstruction and automatic segmentation, based on a visual assessment. Examples of included reconstructions, T2* maps and automatic segmentations can be found in Figure 2. The contrast between the white matter and cortical grey matter is very clear in both the third echo, and in the T2* maps, allowing for an accurate segmentation. However, the borders of the ventricles are not as clearly as they are in structural reconstructions, and therefore are more challenging to segment accurately.T2* values across gestation for each of the 7 brain tissues can be seen in Figure 3, and decline with gestational age. As expected, all brain tissue volumes increase throughout gestation (Figure 4). The absolute T2* values vary between tissue types with the cerebellum and white matter displaying the highest (non-fluid) values. All are significantly correlated with gestational age with the cerebellum and brainstem most clearly gestational age-related.
Discussion & Conclusion
Fetal brain T2* values decline with gestational age, varying based on brain tissue type. Most studies to date have primarily measured whole brain T2* values, and these results suggest that a more in-depth analysis could elucidate further insights into prenatal brain development. It is possible to create normative curves based on regional brain T2* values and could potentially be a biomarker. Next steps involve the creation of such norms by including more cases and comparing pathological regional fetal brain T2* values to such norms. The increased dynamic T2* range at low field strength allows for an in-depth analysis of regional fetal brain T2* values.Acknowledgements
The authors thank all the participating families as well as the midwives and radiographers involved in this study. This work was supported by the NIH (Human Placenta Project—grant 1U01HD087202‐01), Wellcome Trust Sir Henry Wellcome Fellowship (201374/Z/16/Z and /B), UKRI FLF (MR/T018119/1), DFG Heisenberg funding [502024488], EPSRC (EP/V034537/1), the NIHR Clinical Research Facility (CRF) at Guy's and St Thomas' and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Clinical Research Facility based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS or the NIHR or the Department of Health and Social Care.References
1. Hutter, J. et al. Exploring the role of a time-efficient MRI assessment of the placenta and fetal brain in uncomplicated pregnancies and these complicated by placental insufficiency. Placenta 139, 25–33 (2023).
2. Blazejewska, A. I. et al. 3D in utero quantification of T2* relaxation times in human fetal brain tissues for age optimized structural and functional MRI. Magn. Reson. Med. 78, 909–916 (2017).
3. Uus, A. U. et al. Combined Quantitative T2* Map and Structural T2-Weighted Tissue-Specific Analysis for Fetal Brain MRI: Pilot Automated Pipeline. in Perinatal, Preterm and Paediatric Image Analysis (eds. Link-Sourani, D. et al.) 28–38 (Springer Nature Switzerland, 2023). doi:10.1007/978-3-031-45544-5_3.
4. Pier, D. B. et al. 3D Super-Resolution Motion-Corrected MRI: Validation of Fetal Posterior Fossa Measurements. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 26, 539–544 (2016).
5. Aviles Verdera, J. et al. Reliability and Feasibility of Low-Field-Strength Fetal MRI at 0.55 T during Pregnancy. Radiology 309, e223050 (2023).
6. Ponrartana, S. et al. Low-field 0.55 T MRI evaluation of the fetus. Pediatr. Radiol. (2023) doi:10.1007/s00247-023-05604-x.
7. Fulford, J. & Gowland, P. A. The emerging role of functional MRI for evaluating fetal brain activity. Semin. Perinatol. 33, 281–288 (2009).
8. Kuklisova-Murgasova, M., Quaghebeur, G., Rutherford, M. A., Hajnal, J. V. & Schnabel, J. A. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Med. Image Anal. 16, 1550–1564 (2012).
9. Scripts for automated SVRTK reconstruction dockers. (2023).
10. Payette, K. et al. An Automated Pipeline for Quantitative T2* Fetal Body MRI and Segmentation at Low Field. in Medical Image Computing and Computer Assisted Intervention – MICCAI 2023 (eds. Greenspan, H. et al.) 358–367 (Springer Nature Switzerland, 2023). doi:10.1007/978-3-031-43990-2_34.
11. Uus, A. U. et al. BOUNTI: Brain vOlumetry and aUtomated parcellatioN for 3D feTal MRI. eLife 12, (2023).
Figures