0816
Development of a cross-modality tissue-mimicking and anatomic mimicking Fetal Phantom to improve image based fetus assessment1INSERM U1254, IADI, University of Lorraine, Vandoeuvre les Nancy, France, 2CIC-IT 1433, CHRU Nancy, Vandoeuvre les Nancy, France, 3CIC-P 1433, CHRU Nancy, Vandoeuvre les Nancy, France, 4Maternité Régionale de Nancy, Vandoeuvre les Nancy, France
Synopsis
Keywords: Fetal, Phantoms, Fetus, Biometrics, Tissue mimicking, Cross-modality imaging
Motivation: Fetal MRI necessitates extra care due to inherent safety concerns, complicating the optimization of MRI protocols and calibration with ultrasound assessments.
Goal(s): To mitigate the aforementioned safety problems, we aim to create a cross-modality, tissue-mimicking, anatomically correct fetal phantom.
Approach: We designed a fetus phantom encapsulated within a natural rubber balloon filled with mimicking amniotic fluid, creating an amniotic sac analogue. This design utilized varying compositions of agarose, gadolinium, and gelatin to replicate different fetal organs with distinct T1 and T2 values.
Results: The developed phantom comprises various fetal organs and relaxation times, enabling precise fetal biometric comparisons between MRI and ultrasound modalities.
Impact: With the help of the developped cross-modality, tissue-mimicking and anatomical mimicking fetus phantom, the aforementioned constraints on fetal MR protocol optimization and calibration between different MR and ultrasound should be relaxed.
Introduction
Complementary to ultrasound, fetal MR is established as a reliable modality for evaluating anomalies not fully assessed by ultrasound1,2. However, fetal MRI is hampered by long acquisition time and fetal/maternal motion, necessitating new techniques and optimization of current exams. Safety concerns prevent testing new MR sequences and devices on pregnant patients, unlike on healthy volunteers3. Hence, a tissue-mimicking and anatomically accurate fetus phantom is essential to alleviate these constraints and provide a reference for ultrasound, the first-line imaging modality for fetal assessment. The objective of this work is to develop a cross-modality tissue-mimicking and anatomically accurate fetus phantom to optimize fetal assessment in MRI and ultrasound, focusing on fetal biometric measurements to demonstrate the potential of this construction methodology.Methods
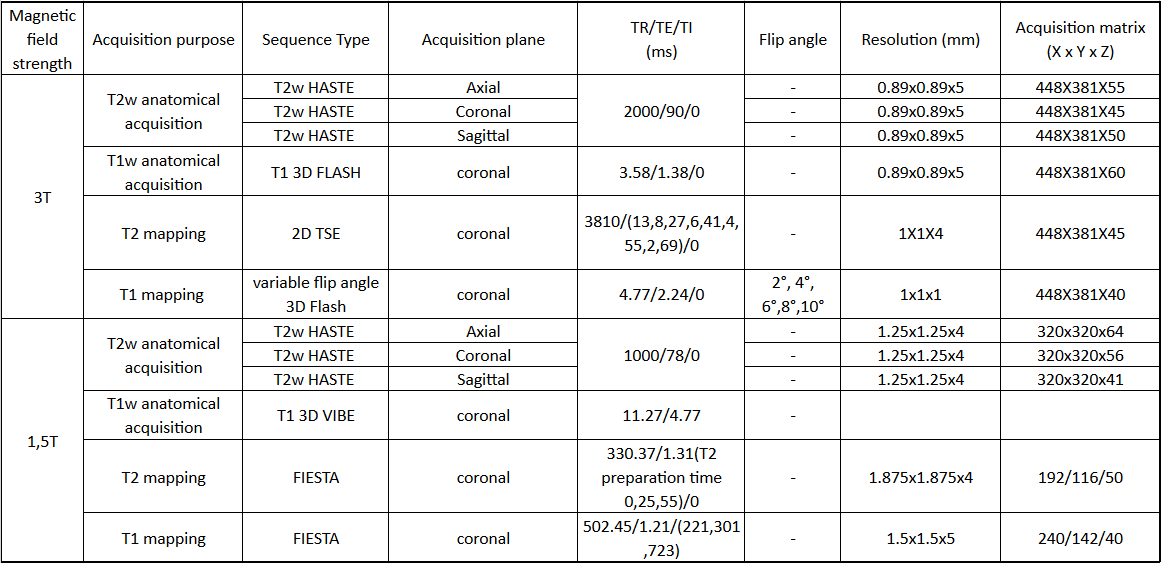
Phantom Design and Construction: We acquired a 26 cm doll empty inside to replicate a second-trimester fetus at approximately 24 weeks gestational age (GA) and its natural posture within the uterus (Figure 1). 0.5-1.5cm ultrasound windows were created in the head, torso, and limbs depending on the size of the particular part, enabling injection. These organ phantoms, made from agarose and gadolinium mixtures with varying percentages, emulate the T2/T1 properties of fetal brain, heart, lungs, stomach, kidneys, and colon. A 3D-printed ABS femur mimics fetal bone geometry for bony tissue simulation4. These components were embedded within a 5% gelatin matrix, reflecting anatomical spacing, and placed inside the doll. We added 0.1% preservative during gel preparation to extend the phantom's usable time. The fetus was encased in a rubber balloon filled with a solution containing 0.2% gadolinium and 0.7% NaCl to simulate amniotic fluid and the amniotic sac, allowing both ultrasound beam penetration and MR acquisition5,6.Data Acquisition: Within one week of constructing the fetus phantom, MRI data were collected on 1.5T (Avanto Fit) and 3T (Prisma) Siemens MRI systems, using clinically relevant protocols. These included a T2-weighted anatomical acquisition (HASTE) from three orthogonal planes, a T1-weighted 3D anatomical scan (FLASH), and T1 and T2 mapping sequences to measure the varying T1 and T2 values designed for each organ and amniotic fluid. The detailed imaging parameters are listed in Table 1. An 18-element abdominal coil and a 32-element spine coil, routinely used for clinical fetal assessment, were used during the acquisitions. Ultrasound images were then captured using a GE Healthcare Vivid S60 system, equipped with standard obstetric functions, by a qualified ultrasound technician.
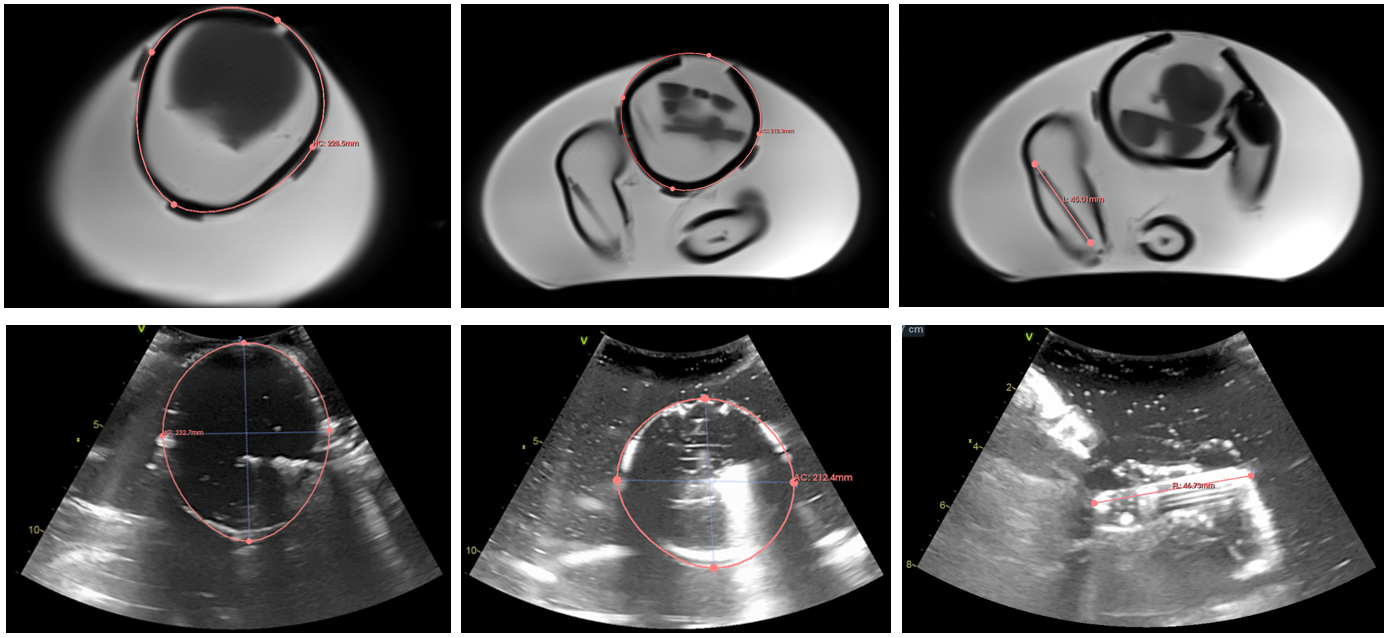
Data Analysis: . A super-resolution algorithm refined the MRI data resolution from 5 mm to 1 mm isotropic, creating a high-resolution MR dataset7. The T1 and T2 maps were generated by the MR console. Fetal biometrics, including head circumference (HC), abdominal circumference (AC), femur length (FL), and biparietal diameter (BPD), were measured on the super-resolution reconstructed MRI data, following the same protocol as in ultrasound. These were then compared with the actual dimensions of the doll to verify the accuracy of the constructed fetus, utilizing 3D Slicer (version 5.2).
Results
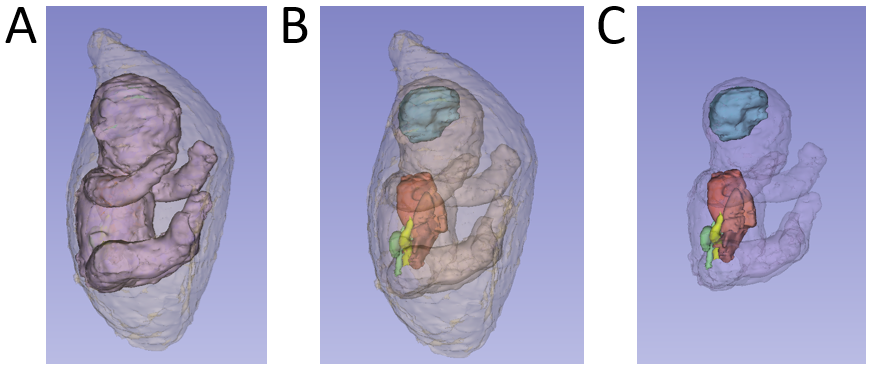
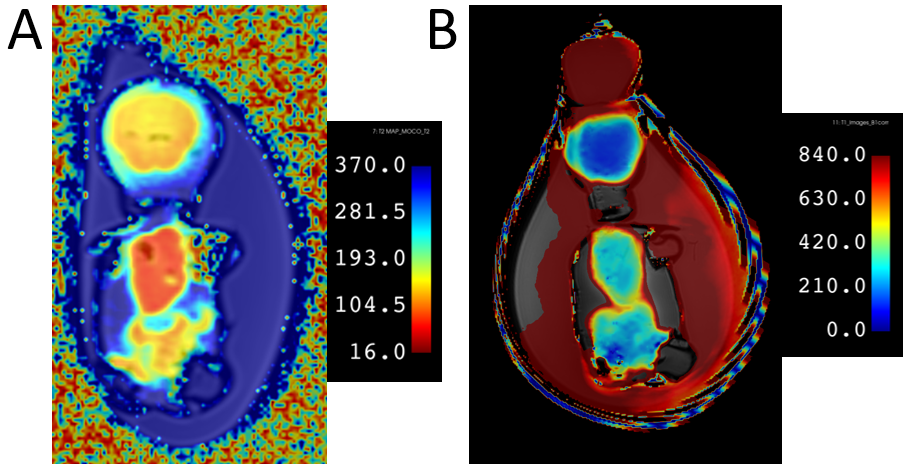
3D geometry model of the phantom after segmentation from super-resolution reconstructed MRI data were shown in Figure 2 to illustrate the anatomical details. Example slice from T1 and T2 maps were shown in Figure 3, illustrating the feasibility of organ-level tissue mimicking ability. In Figure 4, fetal biometric analysis procedure were presented in Figure 3, in which examples of MR and ultrasound acquisition were also included. Fetal biometric measurements from 1.5T and 3T MRIs and ultrasound were shown in Table 2.Discussion
The feasibility of a cross-modality tissue-mimicking and anatomically accurate fetal phantom were presented in this work. Since actual T1 and T2 values at the fetal organ level currently lacks solid data, we did not assign particular values to the phantom organs and amniotic fluid, but just ensured that our phantom's organs had distinct contrasts in anatomical images. The current work only presented fetus corresponding to one size and one GA but it is possible to construct phantoms representing different gestational ages using the proposed method. Our setup is also flexible enough to be extended to include maternal anatomical structure. Other MR properties can also be considered using our methodology. Future work includes accounting for morphological changes in organs during fetal development at different gestational stages.Conclusion
Our study presents the development of an economical, anatomically mimicking fetal phantom to facilitate the advancement of MR techniques in obstetric imaging. It will also allow a more thorough comparison of fetal biometry measurements between MRI and ultrasound. It may potentially offer a reliable way for refining imaging protocols and serve as a practical tool for education and cross-modality calibration.Acknowledgements
No acknowledgement found.References
1. Callec, R., Lamy, C., Perdriolle‐Galet, E., Patte, C., Heude, B., Morel, O., & EDEN Mother–Child Cohort Study Group. (2015). Impact on obstetric outcome of third‐trimester screening for small‐for‐gestational‐age fetuses. Ultrasound in Obstetrics & Gynecology, 46(2), 216-220.
2. Carvalho, J. S., Allan, L. D., Chaoui, R., Copel, J. A., DeVore, G. R., Hecher, K., ... & Yagel, S. (2013). ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart.
3. Bulas, D., & Egloff, A. (2013, October). Benefits and risks of MRI in pregnancy. In Seminars in perinatology (Vol. 37, No. 5, pp. 301-304). WB Saunders.
4. Menikou, G., Yiannakou, M., Yiallouras, C., Ioannides, C., & Damianou, C. (2016). MRI-compatible bone phantom for evaluating ultrasonic thermal exposures. Ultrasonics, 71, 12-19.
5. Yoshida, A., Kato, H., Kuroda, M., Hanamoto, K., Yoshimura, K., Shibuya, K., ... & Hiraki, Y. (2004). Development of a phantom compatible for MRI and hyperthermia using carrageenan gel—relationship between T 1 and T 2 values and NaCl concentration. International journal of hyperthermia, 20(8), 803-814.
6. Benzie, R. J., Doran, T. A., Harkins, J. L., Owen, V. J., & Porter, C. J. (1974). Composition of the amniotic fluid and maternal serum in pregnancy. American Journal of Obstetrics and Gynecology, 119(6), 798-810.
7. Gholipour, A., Estroff, J. A., & Warfield, S. K. (2010). Robust super-resolution volume reconstruction from slice acquisitions: application to fetal brain MRI. IEEE transactions on medical imaging, 29(10), 1739-1758.
Figures
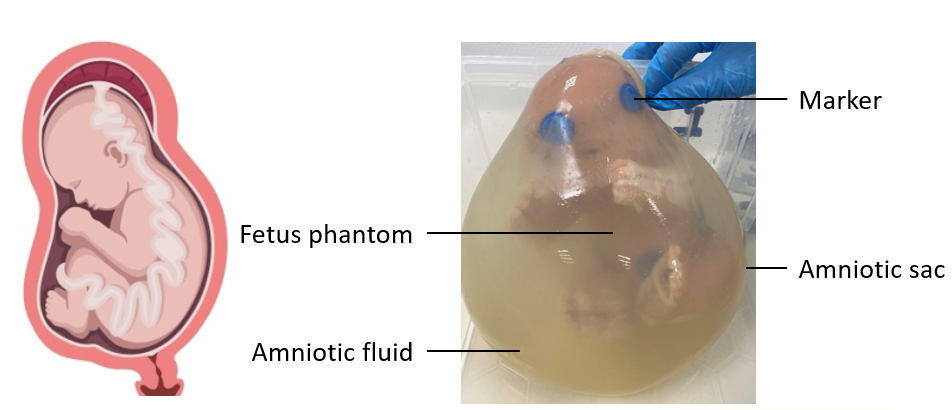
Figure 1. Design idea of the phantom is based on the sketch on the left. The actual phantom picture was presented on the right.