0815
Retrospective Motion Correction for Fetal 4D Flow MRI1Department of Radiology & Nuclear Medicine, Amsterdam University Medical Center, location University of Amsterdam, Netherlands, 2Department of Radiology, Section of Pediatric Radiology, Children’s Hospital Colorado, University of Colorado Anschutz Medical Campus, Denver, CO, United States, 3Department of Pediatric Cardiology, Emma's Children's Hospital, Amsterdam University Medical Center, location University of Amsterdam, Netherlands, 4Department of Pediatrics, Section of Cardiology, Children’s Hospital Colorado, University of Colorado Anschutz Medical Campus, Denver, CO, United States, 5Department of Bioengineering, University of Colorado Anschutz Medical Campus, Denver, CO, United States
Synopsis
Keywords: Fetal, Motion Correction
Motivation: Maternal breathing and fetal bulk motion frequently limit the utility of fetal 4D flow MRI.
Goal(s): To demonstrate the effects of maternal respiratory and fetal bulk motion correction on 4D flow MRI
Approach: Prospective undersampled fetal 4D flow data were acquired in two subjects, followed by compressed sensing reconstruction that included maternal respiratory gating and bulk motion correction. Standard SENSE-accelerated 4D flow acquisitions without motion correction (N=22) provided reference for the ability to quantify flow.
Results: Comparisons of the motion corrected data to normative performance illustrate the technique’s potential for mitigating motion in fetal 4D flow, with equivalence to standard SENSE accelerated scans.
Impact: The proposed sequence and flexible reconstruction workflow provide motion robustness for fetal 4D flow MRI. Further exploration of motion correction techniques has potential to enhance spatial and temporal resolution and to mitigate motion-related errors over extended scanning durations.
Introduction
Fetal 4D flow MRI may improve diagnoses in congenital heart defects beyond echocardiography, but maternal breathing and fetal motion pose challenges for clinical adaptation. Earlier reports of fetal cardiac 4D flow MRI did not use any motion compensation1 or used 2D slice-to-volume motion compensation strategies2,3, which were optimized for non-gated acquisitions. Here, we demonstrate a pipeline for retrospective maternal respiratory and fetal bulk motion correction of fetal cardiac 4D flow using compressed sensing (CS) acceleration. The scans were compared to reference flow metrics established in healthy volunteers using SENSE accelerated acquisitions4.Methods
AcquisitionWith IRB approval, 22 healthy pregnant volunteers (gestational age=34±2 weeks) were prospectively recruited and scanned at 3T (Philips Ingenia). 4D flow data of the fetal heart and the proximal vasculature was acquired in free breathing conditions with scan parameters: acquired spatiotemporal resolution=(2.5mm)3, 38-50ms, reconstructed spatial resolution=(0.75×0.75×1.25-2.5mm), acquired cardiac phases=10, VENC=150cm/s, TR/TE/FA=2.85-3.39ms/1.67-2.12ms/6°, and scan time=140-260s4. SENSE acceleration was R=2/1.5 in phase/partition directions4. In addition, prospectively undersampled 4D flow MRI using pseudo-spiral sampling (PROUD5, R=5) was performed in two healthy pregnant volunteers (gestational age=36w, 34w) using matched scan parameters. Fetal cardiac gating was achieved with an MR-compatible Doppler ultrasound device (DUS) (Northh Medical6,7). Respiratory bellows provided maternal breathing information.
Reconstruction
The proposed PROUD 4D flow acquisition and motion correction reconstruction is illustrated and described in Figure 1.
The respiratory belt guided the inclusion of expiratory data at a ~60% efficiency window (R=7.7-8). 3D bulk motion correction began with sorting the raw data into 8 consecutive dynamic frames with a temporal resolution of 15 seconds per frame. CS reconstruction was performed, followed by creation of a phase-contrast angiogram (PC-MRA) per dynamic frame (phase contrast magnitude times absolute velocity). The resulting images were registered using a rigid monomodal method, and the obtained translations were applied back to
Visualization and quantification
Flow within major vessels was visualized and quantified using Ensight (Ansys). Volume segmentation of the aorta and ductus arteriosus (ductus) was performed in 3DSlicer using the cardiac time-averaged PC-MRA. Image quality was qualitatively assessed using peak-systolic streamlines. Data were quantitatively compared in terms of the coefficient of variation for net flow along the descending aorta (DAo). In comparing with the SENSE accelerated reference values, mass conservation was determined between ductus, distal aortic arch and DAo. The normative quality metric for within-subject coefficient of variation (WS-CV) of net flow was found for three planes each placed 1mm apart at three separate locations, i.e. the arch, ductus and DAo.
Results
Figure 2 demonstrates a reduction of motion artifacts by excluding maternal inspiratory data. The investigated method provided an overall improved depiction of anatomical features in the magnitude image and the DAo in the corrected phase image.Figure 3 shows maximum intensity projections (MIPs) of the datasets. The blurriness of the aorta due to motion is more prominent in the coronal MIP of the SENSE scan and is sharpened in the corrected PROUD scan. The aorta contains more signal in the corrected than the uncorrected scan.
In Figure 4, streamlines depict inflow from the left heart to the DAo. Fig 4d shows that the corrected data had a lower CV along the DAo than the SENSE data and less variability than the uncorrected data. Using planes similar those in Fig5, the mean CV for flow through the ductus and DAo of the N=22 SENSE accelerated data was 5±4%. The corresponding CV for uncorrected/motion corrected PROUD data was participant1=4.24%/4.06% and participant2=27%/8.5%.
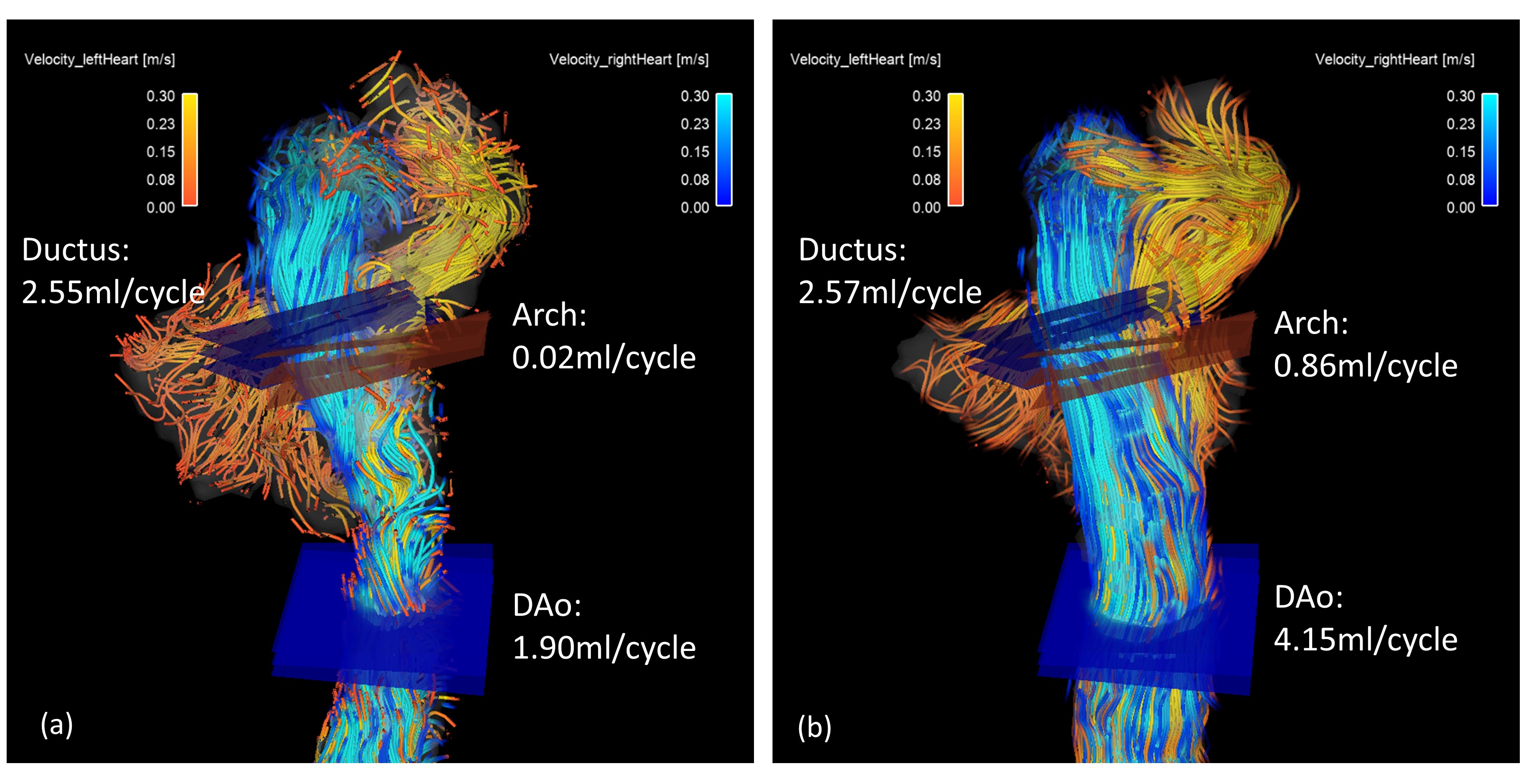
In Figure 5, peak systolic streamlines are displayed for the anatomical region where the aorta and ductus feed into the DAo. In the PROUD subjects, conservation of mass difference for uncorrected and corrected was participant1=35%/18% and participant2 = 9%/11% error. Mass conservation in the N=22 SENSE accelerated data had an average of 19±12% error between ductus and isthmus flow versus descending aorta.
Discussion and Conclusion
Comparison of the motion corrected data to normative values illustrate the technique’s potential for mitigating maternal respiratory and fetal bulk motion in fetal 4D flow, with shown equivalence to a less accelerated standard SENSE acquisition.PROUD provides motion robustness through its flexibility in reconstruction methods. The technique holds promise to reconstruct and retrospectively combine separate motion states as detected by the DUS for improved image quality. Further exploration of advanced motion correction techniques, including non-rigid registration and the incorporation of motion acceptance criteria, holds the potential to enhance spatial and temporal resolution, making it possible to mitigate motion-related errors over extended scanning durations.
Acknowledgements
No acknowledgement found.References
1. Knapp J, Tavares de Sousa M, Lenz A, et al. Fetal 4D flow MRI of the great thoracic vessels at 3 Tesla using Doppler-ultrasound gating: a feasibility study. Eur Radiol. Mar 2023;33(3):1698-1706. doi:10.1007/s00330-022-09167-7
2. Roberts TA, van Amerom JFP, Uus A, et al. Author Correction: Fetal whole heart blood flow imaging using 4D cine MRI. Nat Commun. Dec 14 2020;11(1):6413. doi:10.1038/s41467-020-20353-3
3. Goolaub DS, Xu J, Schrauben EM, et al. Volumetric Fetal Flow Imaging With Magnetic Resonance Imaging. IEEE Trans Med Imaging. Oct 2022;41(10):2941-2952. doi:10.1109/TMI.2022.3176814
4. Englund EKF, T.; Smith, S.: Cuneo, B.: Moghari, M.; Meyers, M.L.; Friesen, R.M.; Browne, L.P.; Barker, A.J. . 4D flow MRI for investigation of fetal cardiovascular hemodynamics in healthy development and ductal dependent lesions presented at: Proceedings of the International Society for Magnetic Resonance in Medicine; 2023; Toronto Session 31st Scientific Meeting and Exhibition.
5. Blanken CPS, Gottwald LM, Westenberg JJM, et al. Whole-Heart 4D Flow MRI for Evaluation of Normal and Regurgitant Valvular Flow: A Quantitative Comparison Between Pseudo-Spiral Sampling and EPI Readout. J Magn Reson Imaging. Apr 2022;55(4):1120-1130. doi:10.1002/jmri.27905
6. Kording F, Yamamura J, de Sousa MT, et al. Dynamic fetal cardiovascular magnetic resonance imaging using Doppler ultrasound gating. J Cardiovasc Magn Reson. Mar 12 2018;20(1):17. doi:10.1186/s12968-018-0440-4
7. Kording F, Schoennagel BP, de Sousa MT, Fehrs K, Adam G, Yamamura J, Ruprecht C. Evaluation of a Portable Doppler Ultrasound Gating Device for Fetal Cardiac MR Imaging: Initial Results at 1.5T and 3T. Magn Reson Med Sci. Oct 10 2018;17(4):308-317. doi:10.2463/mrms.mp.2017-0100
8. Schrauben EM, Lim JM, Goolaub DS, Marini D, Seed M, Macgowan CK. Motion robust respiratory-resolved 3D radial flow MRI and its application in neonatal congenital heart disease. Magn Reson Med. Feb 2020;83(2):535-548. doi:10.1002/mrm.27945
Figures
Figure 2. 4D flow MRI magnitude (top) and foot-head velocity (bottom) images of the PROUD acquisition (a) without (R=5.1) and (b) with motion compensation (R=7.7) , with (c) Cartesian SENSE accelerated acquisition of the same subject (R=3). Motion compensation enhances overall anatomical visibility, with the fetal spine (in the dotted circle) more visible without the signal negating effects of maternal respiration. Flow through the DAo (arrows) is marked by respiratory motion artifact in the uncorrected image and aliasing from fetal motion in the DAo of the cartesian SENSE data.
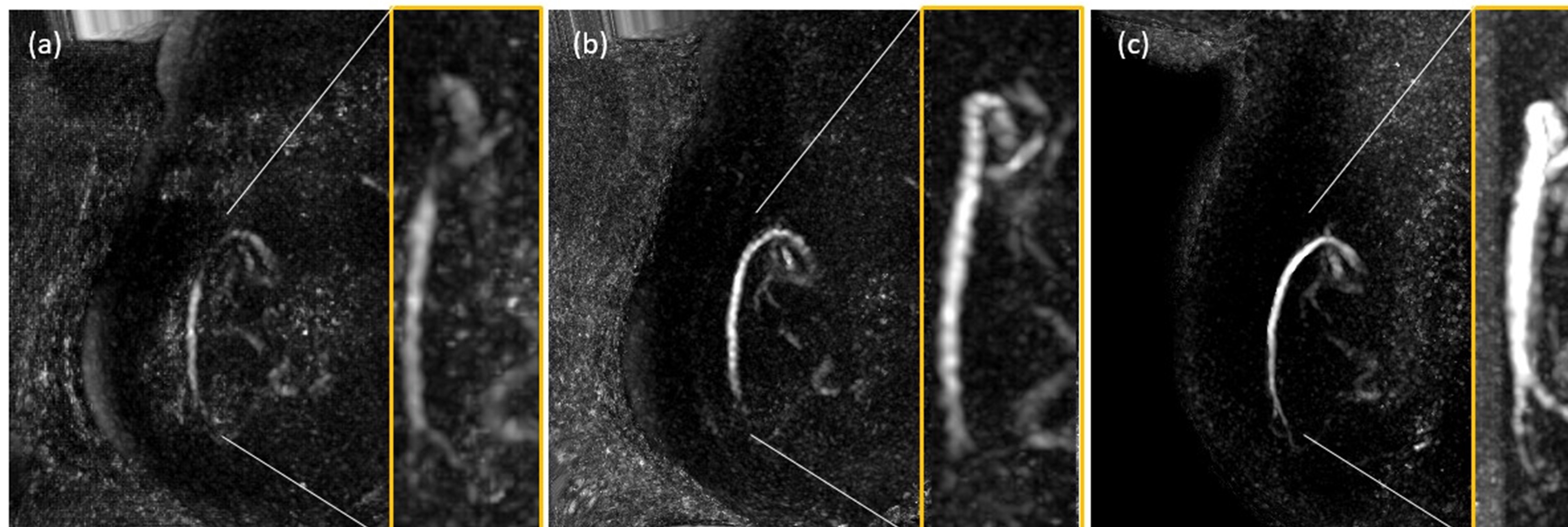
Figure 3. Maximum intensity projections in sagittal direction and magnified inserts (in yellow) of the coronal direction of the PC-MRA created with (a) the uncorrected PROUD data, (b) the corrected PROUD data and (c) the data acquired with SENSE acceleration. In the coronal view, the descending aorta of (b) the motion corrected data has less blurring than what is seen in (a) and (c), which corresponds to the aliasing and noise observed in Figure 2.
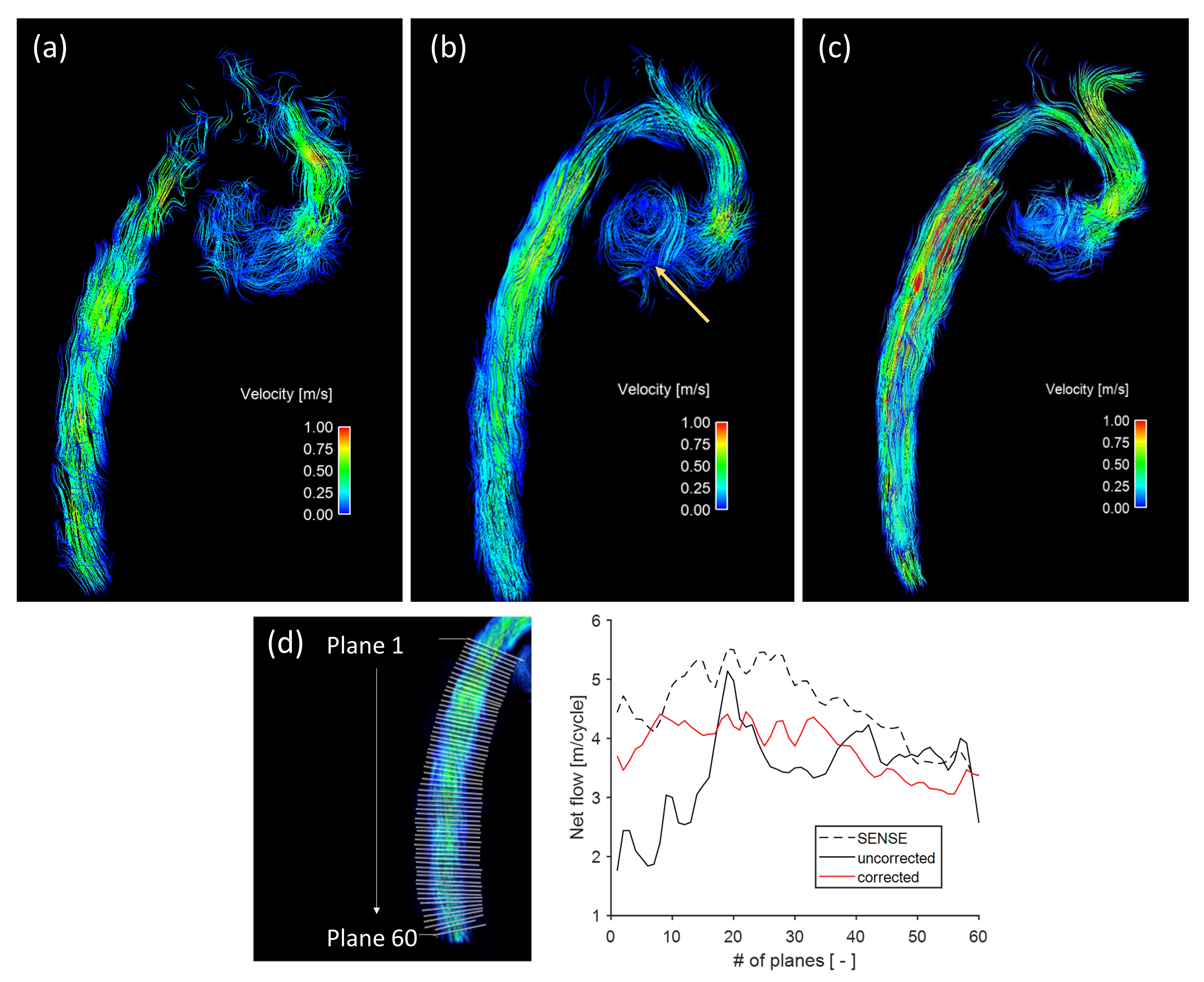
Figure 4. Streamline visualizations show the capability of (a) the uncorrected and (b) corrected PROUD data and (c) SENSE accelerated data to resolve flow in the healthy fetus, with noticeably less noise in motion correction. Flow in the arch and through the foramen ovale (yellow arrow) can be seen better in the corrected data. 60 adjacent planes were placed along the DAo (d) and net flow was quantified. The resulting coefficient of variation (CV) for net-flow through sequential planes was lower for the corrected data (CV=0.11) than for the uncorrected (CV=0.21) and SENSE data (CV=0.14).