0794
A Subject-Specific Workflow for Radiofrequency Safety of Infants Undergoing an MRI Head Scan at 7T1Center for Magnetic Resonance Research (CMRR), University of Minnesota, Minneapolis, MN, United States, 2Masonic Institute for the Developing Brain, University of Minnesota, Minneapolis, MN, United States, 3Institute of Child Development, University of Minnesota, Minneapolis, MN, United States, 4Department of Pediatrics, University of Minnesota, Minneapolis, MN, United States
Synopsis
Keywords: Safety, Safety
Motivation: Higher SNR promised at higher field strengths can be traded for higher spatial resolution, which is essential for imaging infant brains.
Goal(s): To assess and ensure safe operation of a commercially-available RF head coil at 7T for infant subjects.
Approach: We developed an EM model of the coil and experimentally validated it. Utilizing EM simulations, we calculated local and head SARs for an infant model to determine the safe operation limits.
Results: We showed that the head SAR limit is reached before the local SAR limit. We acquired structural and functional MRI data from an infant's brain at 7T.
Impact: Assessing and ensuring the safe operation of 7T MRI scanners for infant subjects can pave the way to exploring the early stages of human brain development, which is hardly possible at lower field strengths due to lower spatiotemporal resolution.
Introduction
Higher field strengths in ultrahigh field (UHF; ≥7T) MRI scanners promise increased SNR1-3. Higher SNR can be traded for higher spatiotemporal resolution, which has yielded promising outcomes in anatomical4,5 and functional6,7 MRI studies. In any case, due to the much smaller size of infant's brain compared to the adult, achieving higher spatial resolutions is paramount to understanding functional and anatomical structures with the spatial accuracy we routinely achieve in adults.The FDA has recently approved multiple 7T MRI scanners for clinical use8,9. However, the most popular FDA-approved 7T system—the Siemens Magnetom Terra—is currently only certified for subject weights above 30kg. Therefore, rigorous safety assessments must be conducted on-site in compliance with international guidelines10. One potential risk is due to the radiofrequency (RF) energy deposition in the tissue by the transmit coil, which can be minimized by limiting multiple factors10, including head specific absorption rate (SAR) and peak 10g-averaged local SAR (pSAR10g). Recently, in addition to a report of initial 7T infant imaging11, Malik et al12 performed comprehensive numerical studies with neonate models at 7T and concluded that the head SAR limit is highly likely to be reached before the pSAR10g limit.
In this study, we develop an EM model of an RF head coil at 7T and experimentally validate it with B1+ measurement studies. We use the simulation model of the coil along with an infant model to assess the head and body SARs, as well as the pSAR10g. Building upon the simulation outcome, we propose a subject-specific workflow for safe MRI of infants at 7T and report our preliminary data.
Methods
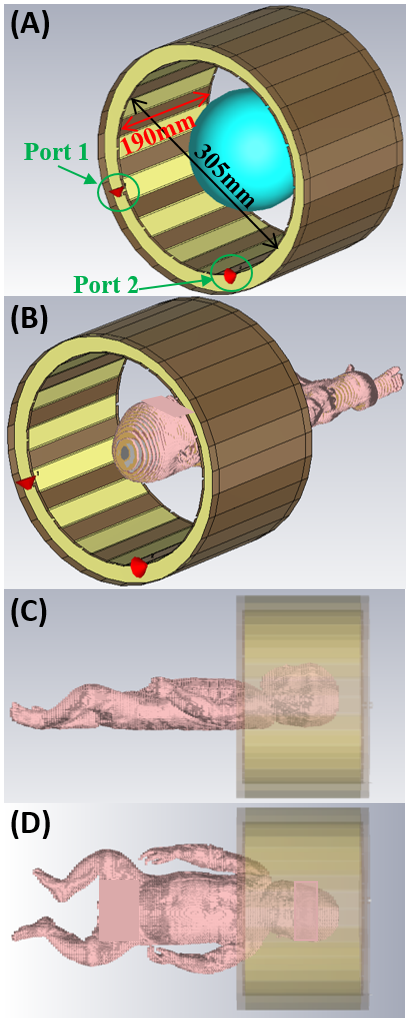
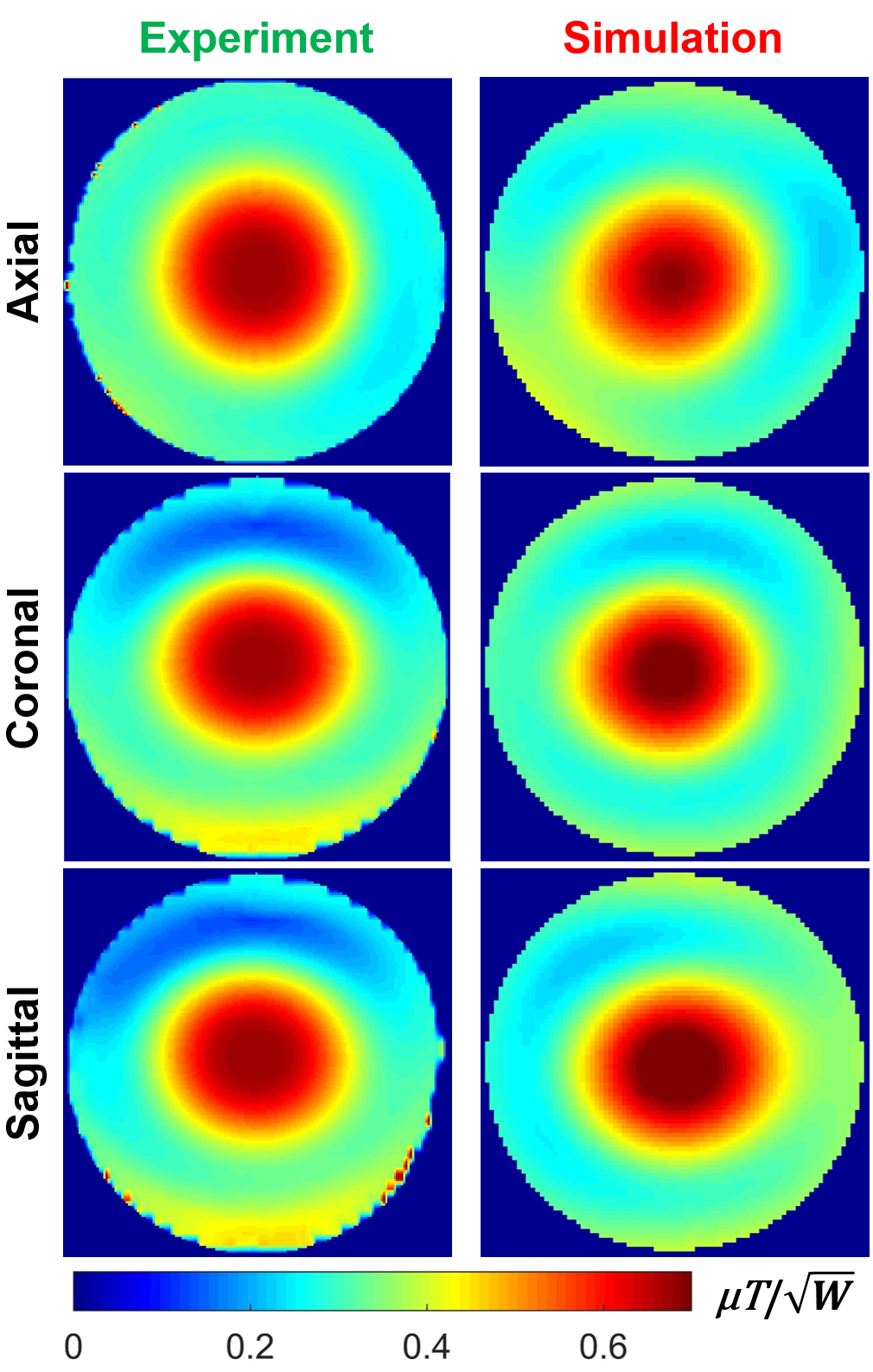
Coil Model and ValidationBased on informed conjecture and existing literature12, an EM simulation coil model was developed to emulate a commercially-available 7T head transmit coil (Nova Medical). Using CST Studio, EM simulations were conducted within a spherical phantom (Figure 1A) with εr=50, σ=0.56S/m. Both coil ports were matched to 50Ω better than -16dB at 297MHz. The simulation model was validated through experimental B1+-mapping within a similar spherical phantom using the Nova coil. The numerical and experimental B1+-maps were quantitatively compared using the normalized root-mean-square error (NRMSE).
Power Calculations
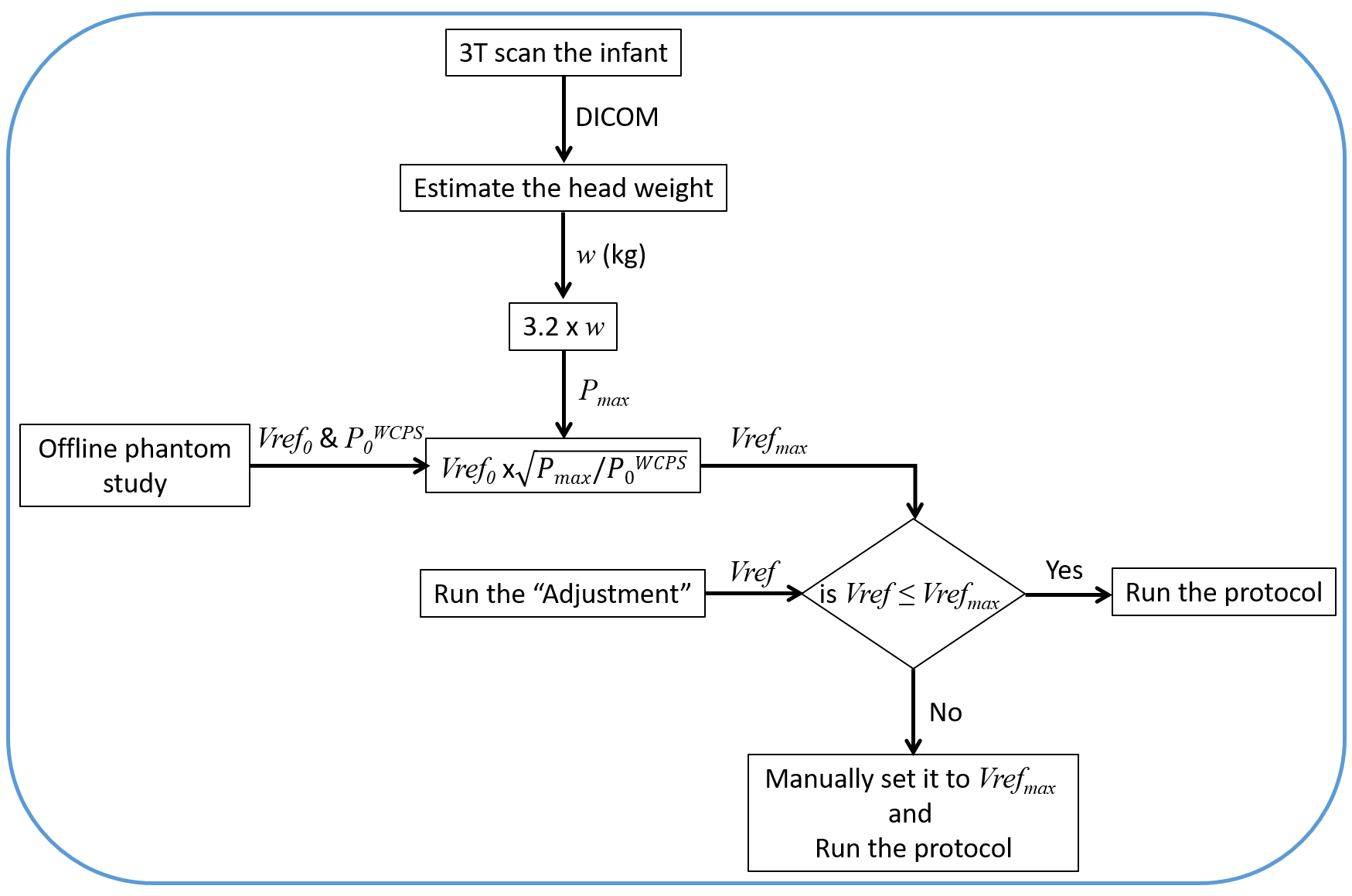
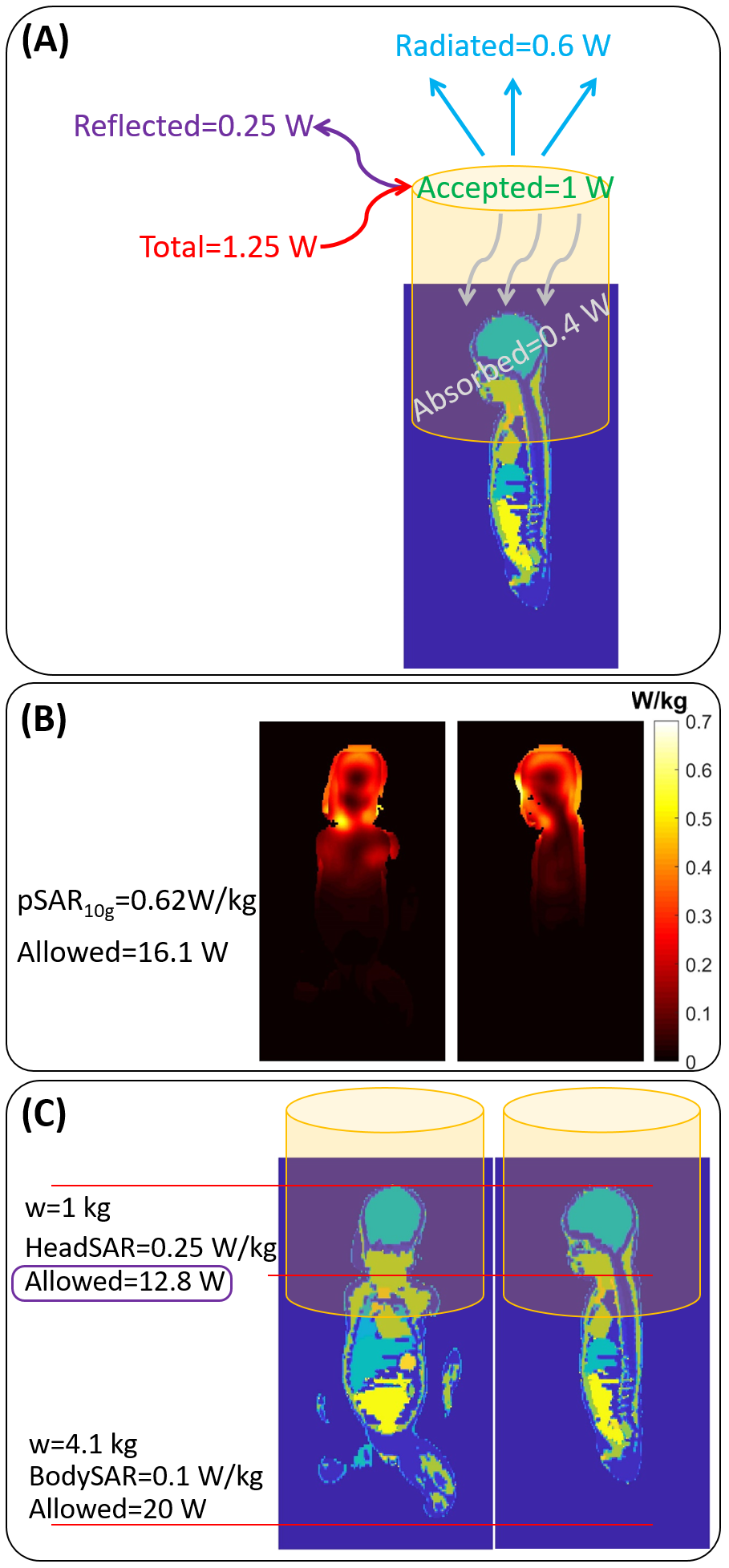
The phantom was replaced with an eight-week-old infant voxel model (Figure 1B-D). To assess the safe operating power limits, a list of different parameters was monitored: input, reflected, accepted, radiated, and tissue-absorbed powers, peak local, head, and body SARs. Ensuring compliance with safety limits10, the conclusion was that the head SAR limit was reached before the local SAR limit. Based on this conclusion, a workflow (Figure 2) was proposed to ensure the safe operation of a 7T Siemens scanner for infant imaging. First, the head weight ($$$w$$$) of the infant was estimated using a 3T anatomical scan. The multiplication of this weight and 3.2W/kg head SAR limit determined the maximum allowable input power of the coil. Additionally, an offline study is conducted with the imaging protocol to determine the worst-case pulse sequence (WCPS: with highest power requirement), as well as its power level (P0WCPS) for a given input voltage (Vref0). Based on this information, a protocol with a fixed maximum voltage for a particular head weight can be selected by the operator. Lastly, a power calibration scan can be done at the beginning of the in-vivo session to determine if less voltage is needed for optimal imaging performance.
Infant Imaging
A seven-week-old infant (5.5kg) was scanned at 7T complying with the power limit calculated following the workflow in Figure 2. The head weight was conservatively estimated as 1kg, and the Pmax was set to 3.2W/kg. A multi-echo T2* weighted fMRI sequence (ME-EPI) was acquired, along with T1 and T2 weighted structural scans to demonstrate proof-of-concept and feasibility.
Results
Figure 3 shows an NRMSE of less than 7% between experimentally and numerically acquired B1+ maps.Figure 4 shows the power budget in the transmit coil in the presence of the infant model, the 10g-averaged SAR map, and head and body SAR calculations for this infant model.
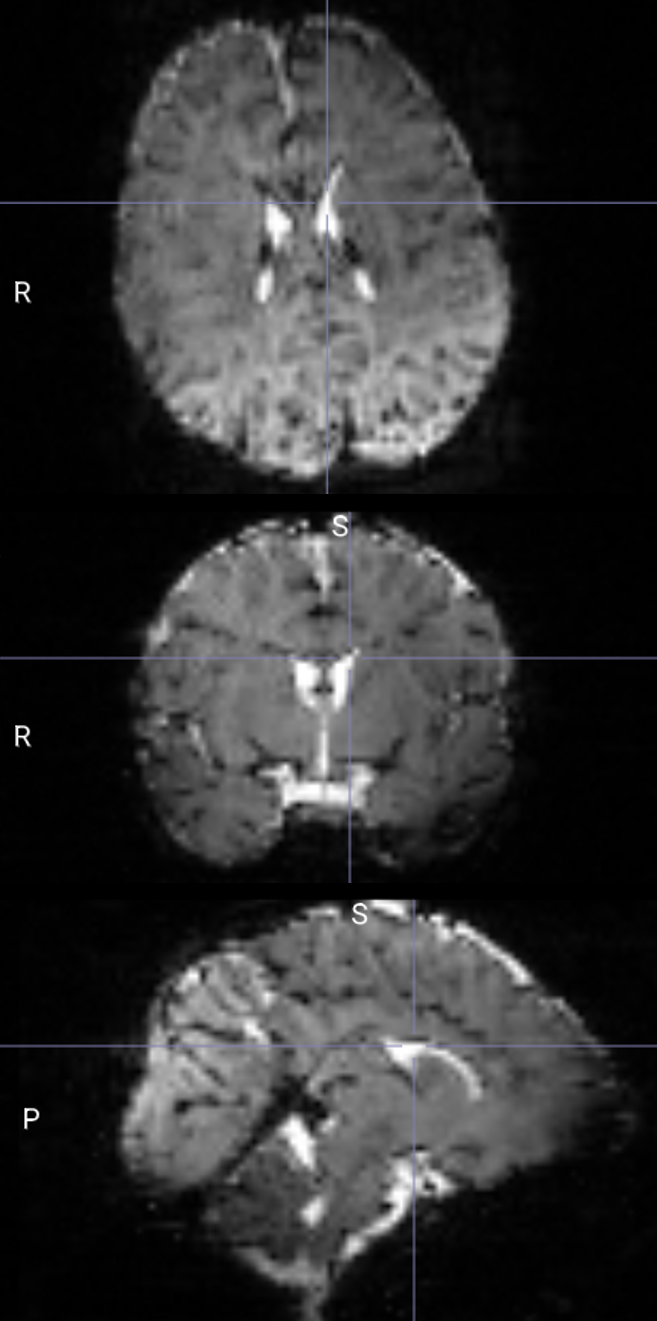
Figure 5 shows the single-echo EPI image of the infant’s brain.
Discussions and Conclusion
In this study, we proposed a workflow for safe MRI of infants at 7T, based on an EM model of the Nova coil validated with B1+ measurements. According to Figure 4, less than 25% of the input power was dissipated in the head. However, to add an additional safety buffer in the proposed workflow, the total input power was used to calculate the head SAR. While preliminary data were acquired to demonstrate feasibility, further studies are ongoing to optimize functional and anatomical contrast and sensitivity.Acknowledgements
This work was supported by the following grants: NIH P41 EB027061 and NIH R01NS115180.References
1. Vaughan JT, Garwood M, Collins CM, Liu W, DelaBarre L, Adriany G, Andersen P, Merkle H, Goebel R, Smith MB. 7T vs. 4T: RF power, homogeneity, and signal‐to‐noise comparison in head images. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2001;46(1):24-30.
2. Pohmann R, Speck O, Scheffler K. Signal‐to‐noise ratio and MR tissue parameters in human brain imaging at 3, 7, and 9.4 tesla using current receive coil arrays. Magnetic resonance in medicine. 2016;75(2):801-9.
3. Ocali O, Atalar E. Ultimate intrinsic signal‐to‐noise ratio in MRI. Magnetic resonance in medicine. 1998;39(3):462-73.
4. Duyn JH, van Gelderen P, Li TQ, de Zwart JA, Koretsky AP, Fukunaga M. High-field MRI of brain cortical substructure based on signal phase. Proceedings of the National Academy of Sciences. 2007 Jul 10;104(28):11796-801.
5. Budde J, Shajan G, Hoffmann J, Uğurbil K, Pohmann R. Human imaging at 9.4 T using T2*‐, phase‐, and susceptibility‐weighted contrast. Magnetic resonance in medicine. 2011 Feb;65(2):544-50.
6. Uğurbil K. Imaging at ultrahigh magnetic fields: History, challenges, and solutions. Neuroimage. 2018 Mar 1;168:7-32.
7. De Martino F, Yacoub E, Kemper V, Moerel M, Uludağ K, De Weerd P, Ugurbil K, Goebel R, Formisano E. The impact of ultra-high field MRI on cognitive and computational neuroimaging. Neuroimage. 2018 Mar 1;168:366-82.
8. Siemens Healthineers. FDA clears MAGNETOM Terra 7T MRI scanner from Siemens Healthineers. 2017. Accessed July 27, 2023. https://www.siemens-healthineers.com/en-us/news/magnetomterrafdaclearance.html
9. GE Healthcare. Bringing ultra-high field MR imaging from research to clinical: SIGNA 7.0T FDA cleared. 2020. Accessed July 27, 2023. https://www.ge.com/news/press-releases/bringing-ultra-high-field-mr-imaging-from-research-to-clinical-signa-70t-fda-cleared
10. International Electrotechnical Commission. IEC 60601-2-33-Edition 4.0: Medical Electrical Equipment—Particular Requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis. 2022.
11. Annink KV, Van Der Aa NE, Dudink J, Alderliesten T, Groenendaal F, Lequin M, Jansen FE, Rhebergen KS, Luijten P, Hendrikse J, Hoogduin HJ. Introduction of ultra-high-field MR imaging in infants: preparations and feasibility. American Journal of Neuroradiology. 2020 Aug 1;41(8):1532-7.
12. Malik SJ, Hand JW, Satnarine R, Price AN, Hajnal JV. Specific absorption rate and temperature in neonate models resulting from exposure to a 7T head coil. Magnetic Resonance in Medicine. 2021 Sep;86(3):1299-313.
Figures