0793
3T Parallel-Transmit for Simultaneous Stereoelectroencephalography and MRI for Realistic Electrode Placement in Epilepsy Patients1King's College London, London, United Kingdom, 2École Polytechnique Fédérale de Lausanne, Lausanne, Switzerland
Synopsis
Keywords: Safety, Safety
Motivation: Investigating optimised RF heating and B1+ field disturbance with sEEG electrodes placement, covering epileptogenic zones in five configurations, using electromagnetic simulations with 16-channel parallel-transmit coil array at 3T for simultaneous sEEG-MRI.
Goal(s): The challenge is reducing RF heating from implanted electrodes.
Approach: We investigated five electrode placements covering epileptogenic zones to control RF heating and local signal increases using computational field simulations on a realistic computational human model.
Results: Implanting electrodes in the left hemisphere improved RF uniformity. Shimming optimisation, integrating B1+ and 0.1g SAR, showed negligible SAR differences from electrode-free setups. Lower SAR correlated with reduced RF strength, suggesting a necessary trade-off.
Impact: Our study advances simultaneous EEG/fMRI for drug-resistant epilepsy, optimising electrode safety to better localise seizure onset zones and refine surgical approaches, while ensuring patient safety. It allows for more precise epileptogenic zone resection, potentially advancing therapeutic outcomes.
Introduction
Stereoelectroencephalography electrodes (sEEG) facilitate identification of the seizure onset zone to ensure successful resective surgery for drug-resistant epilepsy. The electrode implantation can lead to brain shift, impacting the precision of spatial mapping when post-implantation CT is superimposed with fMRI1. The conductive nature of metallic implants introduces a risk of RF-induced tissue heating during MRI scans2. Previously, with experimental3 and with computational simulations4, simplified electrode positioning at 3T was demonstrated for safe imaging limits for simultaneous sEEG/MRI.This work examines optimised safe RF exposure limits for five different realistic electrode positioning for up to ten-contacts seven to eleven depth electrodes placement in conjunction with a 16-channel parallel transmit RF coil array to minimise local power deposition around the electrodes utilising computational field simulations to improve the accuracy of intra-/post-surgical simultaneous fMRI-EEG measurements, thereby enhancing the safety and effectiveness of surgical interventions for epilepsy.
Method
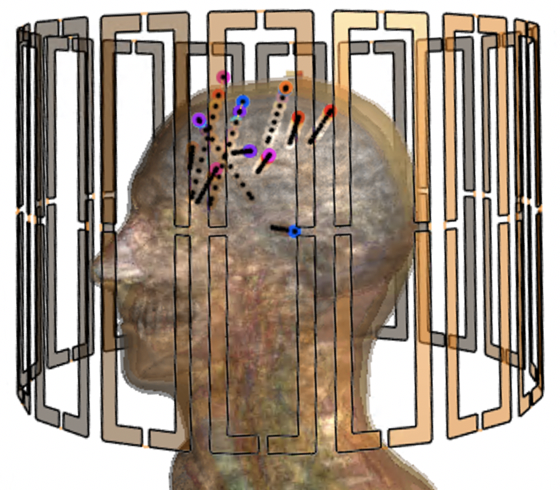
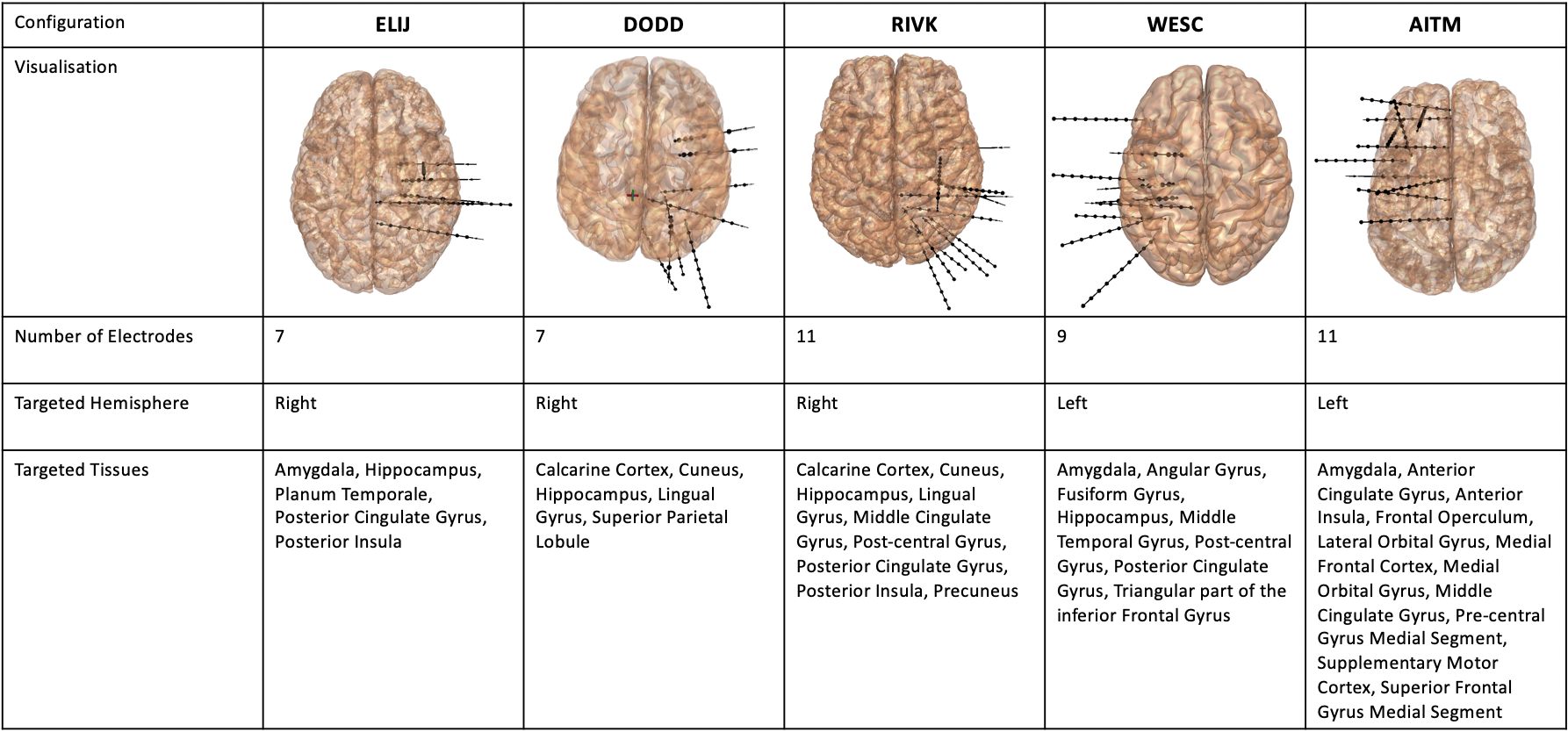
Electromagnetic field simulations were performed using FDTD on Sim4Life 7.0 (ZMT AG, Zurich Switzerland) with a human phantom model Duke(v3.1)5 for 3 Tesla 16-channel head loop array (360mm diameter, 250mm length, 60mm width/loop), placed inside a cylindrical RF shield (1560mm length, 752mm diameter, modelled as PEC) (Figure 1).The pTx coil loops introduced a harmonic excitation signal at 123MHz with a 50Ohm reference load. The simulation convergence level was set to -20dB. Five realistic electrode configurations were simulated to assess the B1+ and local SAR averaged over 1g and 0.1g tissue. Three configurations target common seizure onset zones in the right hemisphere (ELIG, DODD, RIVK), and two cover the left hemisphere (WESC, AITM) (Figure 2).
The electrode design was based off Ad Tech manufactured depth platinum electrodes (epilepsy/LTM spencer probe depth electrodes) containing contacts of length 2.29mm and diameter of 0.86mm. The number of electrodes differs from 7 to 11 with minimum 2 to 10 contacts on each electrode. Each electrode contains a non-extending wire of 0.4mm diameter, connecting all the contacts, and a cylindrical insulator of 0.8mm in diameter, leaving only itself and the contacts exposed to the surrounding tissue.
B1+ and SAR calculations
B1+-fields, E-fields, J-fields and SAR fields are exported from Sim4Life. Q matrices6 were computed for 0.1gram and 1gram of tissue in Duke head. Virtual observations points (VOPs) were derived from the SAR matrices calculation. All results were normalised to 1W total input power.
The B1+ only and combined B1+ and local SAR optimisations were applied to increase B1+ in the whole head, while decreasing the local SAR (1gram of tissue or 0.1gram of tissue) using static RF shimming algorithm7. While transverse slice optimisation was applied at the coil centre with the Gaussian coefficient of 2, sagittal slice optimisation was performed on two sagittal slices, depending on the hemisphere targeted by the implantation to cut through most of the electrodes, both located the same distance from the centre of the model, with Gaussian coefficients of 1 for SAR1g and 2 for SAR0.1g. All results were presented using maximum intensity projection (MIP) of B1+ and local SAR (1g, 0.1g) maps over the whole head.
Results
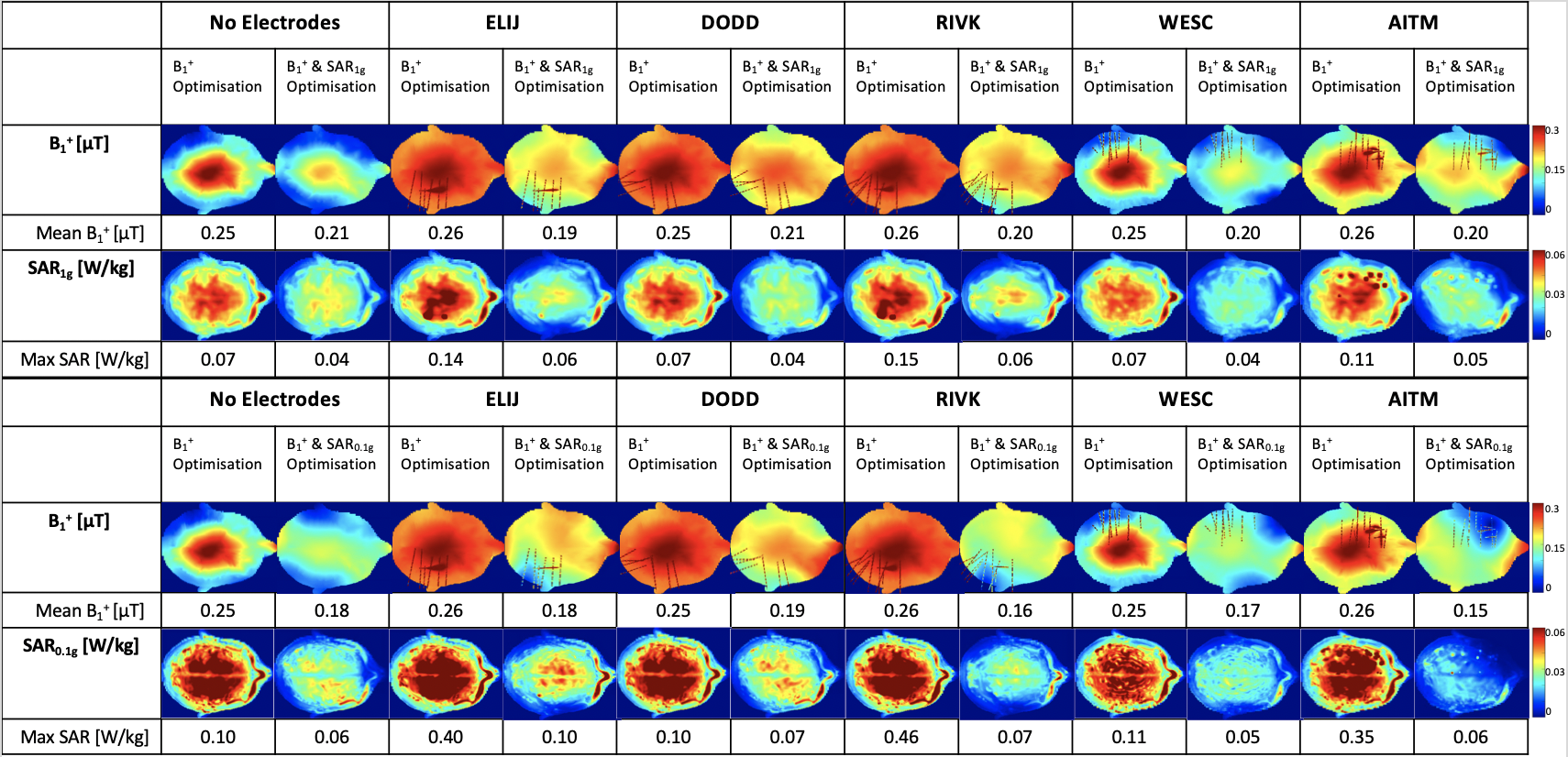
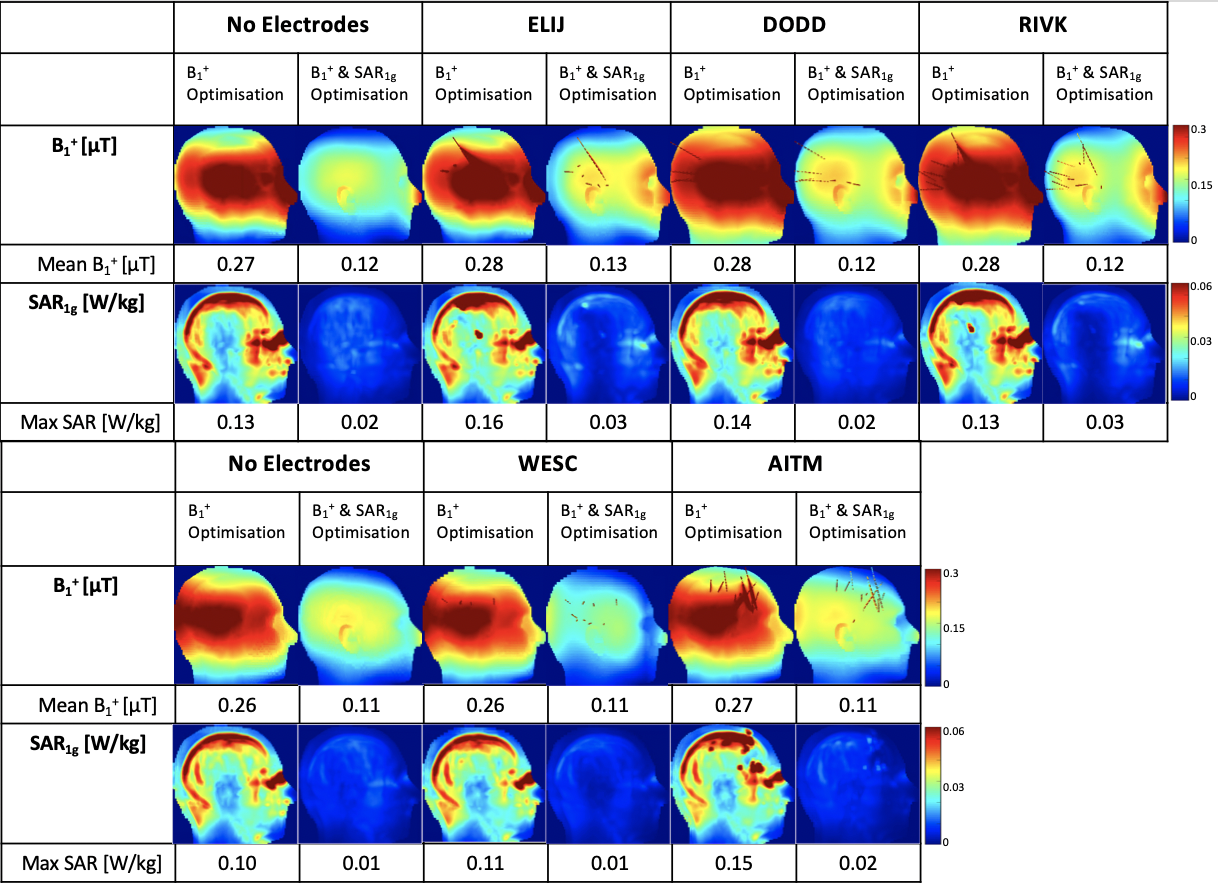
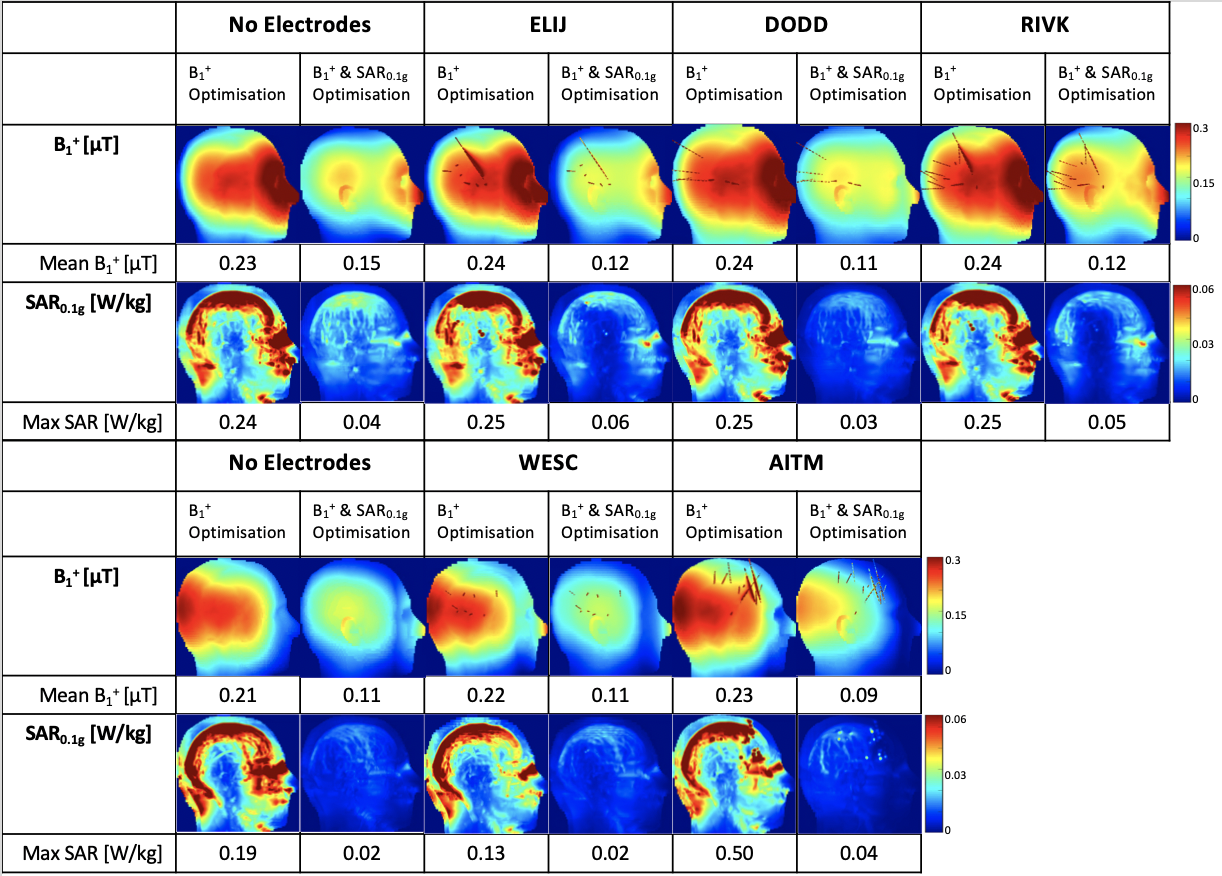
Figure 3 presents the maximum intensity projection in the transverse plane of optimised B1+ and SAR maps. Combined B1+ and SAR optimisation reduces maximum local SAR value by 40% while sacrificing 28% mean B1+ over the head compared to B1+ optimisation, when no electrodes were placed. B1+ distribution decreases where the electrodes were populated to keep the maximum local SAR value under control at the level of no-electrodes case for DODD, RIVK, WESC and AITM configurations.Figure 4 presents the maximum intensity projection in the sagittal plane of optimised B1+ and SAR maps for five different configurations. Mean B1+ and maximum local SAR values were maintained in similar levels as no-electrodes case for all configurations with combined B1+ and SAR optimisation and B1+ only optimisation.
Figure 5 is similar to Figure 4, except SAR is averaged to 0.1g of tissue and the Gaussian coefficient used in the shimming algorithm is 2. With higher resolution of local SAR, still we maintained the mean B1+ and maximum local SAR values similar to the no-electrodes case for all configurations with realistic electrode placements.
Discussion and Conclusion
16-channel parallel-transmit single-row loop coil array allows the control of mean B1+ and maximum local SAR values for 1g and 0.1g of tissue successfully, using static RF shimming applied with in-house developed B1+ and SAR optimisation method for five different realistic sEEG configurations applied on the epilepsy patients.Acknowledgements
This work was supported by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London and/or the NIHR Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.References
- Carmichael DW, Vulliemoz S, Rodionov R, Thornton JS, McEvoy AW, Lemieux L. Simultaneous intracranial EEG–fMRI in humans: Protocol considerations and data quality. NeuroImage. 2012;63(1):301-309. doi:10.1016/j.neuroimage.2012.05.056.
- Carmichael DW, Thornton JS, Rodionov R, Thornton R, McEvoy A, Allen PJ, Lemieux L. Safety of localizing epilepsy monitoring intracranial electroencephalograph electrodes using MRI: Radiofrequency-induced heating. J Magn Reson Imaging. 2008;28(5):1233-1244. doi:10.1002/jmri.21583.
- Fujita Y, Khoo HM, Hirayama M, Kawahara M, Koyama Y, Tarewaki H, Arisawa A, Yanagisawa T, Tani N, Oshino S, Lemieux L, Kishima H. Evaluating the safety of simultaneous intracranial electroencephalography and functional magnetic resonance imaging acquisition using a 3 Tesla magnetic resonance imaging scanner. Front Neurosci. 2022;16:921922. doi:10.3389/fnins.2022.921922.
- Guarnotta F, Clement J, Sparks R, Ipek Ö. Safe-MRI with stereo-electroencephalography (sEEG) for epilepsy patients. Abstract presented at: ISMRM & SMRT Annual Meeting & Exhibition; May 15-20, 2021; Online. Abstract No. 0363. Available from: https://archive.ismrm.org/2021/0363.html.
- Gosselin MC, Neufeld E, Moser H, Huber E, Farcito S, Gerber L, Jedensjö M, Hilber I, Di Gennaro F, Lloyd B, Cherubini E, Szczerba D, Kainz W, Kuster N. Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0. Phys Med Biol. 2014;59(18):5287-5303. doi:10.1088/0031-9155/59/18/5287.
- Ipek Ö, Raaijmakers AJ, Lagendijk JJ, Luijten PR, van den Berg CAT. Intersubject local SAR variation for 7T prostate MR imaging with an eight-channel single-side adapted dipole antenna array. Magn Reson Med. 2014;71(4):1559–67.
- Clément J, Tomi-Tricot R, Malik SJ, et al. Towards an integrated neonatal brain and cardiac examination capability at 7 T: electromagnetic field simulations and early phantom experiments using an 8-channel dipole array. Magn Reson Mater Phy. 2022;35(5):765-778. doi:10.1007/s10334-021-00988-z.
Figures