0790
Pediatric neuroimaging at 7 Tesla: towards building and validating VOPs for local SAR management in pTX1BAOBAB, NeuroSpin, University Paris-Saclay, CEA, CNRS, Gif-sur-Yvette, France, 2IRFU/DACM, University Paris-Saclay, CEA, Gif-sur-Yvette, France
Synopsis
Keywords: Safety, Safety, SAR, ultra-high field, pTX, pediatric
Motivation: Pediatric MRI neuroimaging has become common practice at 1.5 and 3 Tesla and we see the emergence of 7T and parallel transmission (pTX). However, today relevant local SAR prediction models are based on adult standards.
Goal(s): In this work, we study the local SAR at 7T with pTX for children population (6 to 14 years old) using RF electric field simulations.
Approach: We exploit a vast simulation database to build a pediatric local SAR prediction model and propose a methodology for its initial validation using convex optimization.
Results: A large simulation database (above 25) is desirable to combine RF safety and pTX performance.
Impact: This work aims to push pediatric MRI to ultra-high fields by developing safe SAR control for the children population. It also introduces a tool to determine appropriate safety margins to avoid excessive penalizing in the pTX pulse design.
Introduction
Local SAR control in parallel transmission (pTX) conventionally relies on virtual observation points (VOPs)1. These SAR control matrices are generally obtained from electromagnetic (EM) simulations on virtual body models. Due to modeling errors, inter-subject anatomical variability, and limited control of head position in the coil, the designed VOPs must incorporate safety margins2,3. In pediatric neuroimaging, the head size and position are more likely to vary, which makes adult VOPs possibly inapplicable without revising the safety margins. Increasing them will reduce the risk of SAR hotspots but will result in RF power over-restriction and suboptimal RF pulses. This work aims to develop a dedicated local SAR model for children aged 6 to 14 years and to compute adapted safety factors. Using EM simulations for various numerical head models ($$$\small{NHMs}$$$) for a pTX home-made coil, we construct pediatric VOPs and propose a method to test their safety level with a convex optimization algorithm.Theory
Let us denote by $$$\small{\left\{\mathbf{Q}\right\}_{n}≔\left\{\mathbf{Q}_{n}\left(\mathbf{r}\right)\in\mathbb{C}^{N_{ch}\text{x}N_{ch}}\middle|\mathbf{r}\in{NHM}_{n}\right\}}$$$ the local SAR matrices for the nth $$$\small{NHM}$$$ and by $$$\mathcal{V}$$$ the pTX RF excitation vector4. Suppose that VOP matrices $$$\small{\left\{\mathbf{Q^{*}}\right\}}$$$ are constructed for M $$$\small{NHMs^{VOP}}$$$, and we want to verify their safety potential on other set of N $$$\small{NHMs^{test}}$$$ represented by $$$\small{\left\{\mathbf{Q}\right\}_{n=1..N}}$$$. To test the set $$$\small{\left\{\mathbf{Q^{*}}\right\}}$$$ against each $$$\small{\mathbf{Q}_{n}\left(\mathbf{r}\right)\in\left\{\mathbf{Q}\right\}_{n}}$$$ independently on the RF excitation, we use the R-criterion: $$\small{R\left(\mathbf{Q}_{n}\left(\mathbf{r}\right),\left\{\mathbf{Q}^{*}\right\}\right)=\max_{\mathcal{V}\in\mathbb{C}^{Nch}}\left(\frac{SAR(\mathbf{Q}_{n}\left(\mathbf{r}\right),\mathcal{V})}{{SAR}^{*}\left(\left\{\mathbf{Q^{*}}\right\},\mathcal{V}\right)}\right) [Eq.1],}$$ where the maximization is amongst all static RF shims $$$\mathcal{V}$$$, and $$$\small{{SAR}^{*}\left(\left\{\mathbf{Q^{*}}\right\},\mathcal{V}\right):=\max_{\mathbf{Q^{*}}\in\left\{\mathbf{Q^{*}}\right\}}{\left(\mathcal{V}^{H}\mathbf{Q^{*}}\mathcal{V}\right)}}$$$. It was shown5 that i) computing R reduces to a numerically tractable convex optimization problem, and ii) the R criterion is in fact equal to the worst-case ratio of $$$\small{SAR}$$$ to the VOP-calculated $$$\small{SAR^{*}}$$$considering all dynamic RF excitations. Thus, the condition R<1 is sufficient for the VOP set to overestimate the SAR for the given $$$\small{\mathbf{Q}_{n}\left(\mathbf{r}\right)}$$$ for any pTX pulse. Moreover, since for any k>0: $$\small{R\left(\mathbf{Q}_{n}\left(\mathbf{r}\right),\left\{{k\mathbf{Q}}^{*}\right\}\right)=\frac{1}{k}R\left(\mathbf{Q}_{n}\left(\mathbf{r}\right),\left\{\mathbf{Q}^{*}\right\}\right) [Eq.2]}$$ the factor $$\small{k:=\max_{\mathbf{Q}_{n}\left(\mathbf{r}\right)\in\left\{\mathbf{Q}\right\}_{n}}\left(R\left(\mathbf{Q}_{n}\left(\mathbf{r}\right),\left\{Q^{*}\right\}\right)\right) [Eq.3]}$$ gives precisely the minimum multiplicative safety margin that we shall apply to the VOP set $$$\small{\left\{ \mathbf{Q}^{*} \right\}}$$$ to make them safe with respect to nth $$$\small{NHM^{test}}$$$.Methods
The SAR analysis builds on EM simulations made for 8TX/32RX head coil6 at 298MHz with the FDTD method (2x2x2mm3). We used a home-made NHM database7 containing 68 subjects aged between 4 and 16 years (Fig.1). This database was divided on two parts: subgroups $$$\small{NHMs^{VOP}}$$$ of different sizes were used to construct VOPs, other subgroups $$$\small{NHMs^{test}}$$$ represented the test sample.VOP construction: thirty-five VOP sets $$$\small{\left\{\mathbf{Q^{*}}\right\}_{[M]}}$$$ were constructed on an increasing number of head models M=2..30 spanning the age distribution (Fig.2). To compute VOPs, we used the R-criterion-based algorithm of ref. 5.
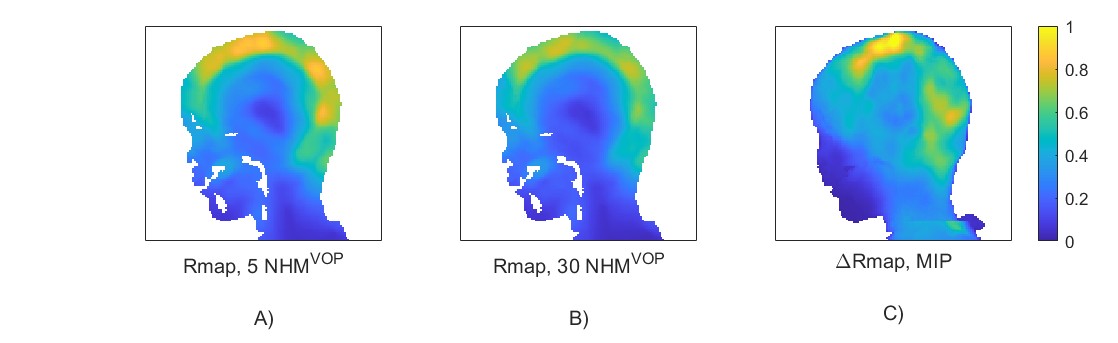
VOP testing: Each VOP set $$$\small{\left\{\mathbf{Q^{*}}\right\}_{[M]}}$$$ was tested on N=30 models not used for VOP construction. For every test subject $$$\small{NHM^{test}_{n=1..N}}$$$, we computed the R-criterion map $$$\small{Rmap(n):=\left\{R\left(\mathbf{Q}_{n}\left(\mathbf{r}\right),\left\{\mathbf{Q^{*}}\right\}_{[M]}\right)\middle|\mathbf{r}\in{NHM}_{n}^{test}\right\}}$$$, the maximum R-criterion value $$$\small{SubjRmax(n):=\max_{\mathbf{r}\in{NHM}_{n}^{test}}{Rmap\left(n\right)}}$$$, and the risk mass $$$\small{SubjRiskMass(n):=numel\left(Rmap\left(n\right)>1\right)·{(2mm)}^{3}·1kg/l}$$$ with numel denoting the voxel number. This allowed us to define
- strict multiplicative safety factor $$$\small{MSF(M)=\max_{n\in1..N}{SubjRmax(n)}}$$$ needed to provide VOP sets $$$\small{MSF(M)·\left\{\mathbf{Q^{*}}\right\}_{[M]}}$$$ passing the safety test on all the $$$\small{NHMs^{test}}$$$ (Eq. 3).
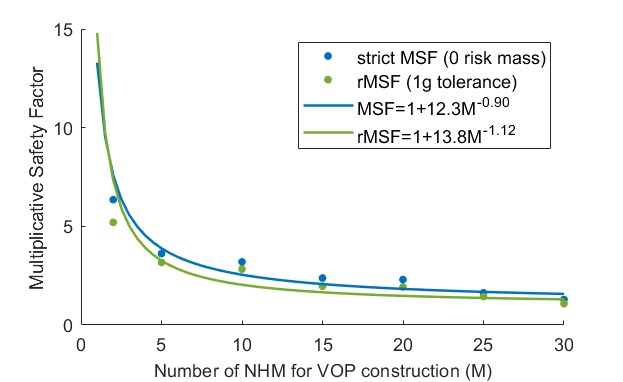
- relaxed safety factor $$$\small{{rMSF}(M)}$$$ by which one needs to multiply all matrices of $$$\small{\left\{\mathbf{Q^{*}}\right\}_{[M]}}$$$ to obtain $$$\small{\max_{n\in1..N}{SubjRiskMass(n)}<1g}$$$ .
Results
Fig.3 displays the $$$\small{SubjRmax}$$$ and $$$\small{SubjRiskMass}$$$ distributions as a function of M. The difference between the R-maps for the same test model obtained with two VOP sets $$$\small{\left\{\mathbf{Q^{*}}\right\}_{[5]}}$$$ and $$$\small{\left\{\mathbf{Q^{*}}\right\}_{[30]}}$$$ is shown in Fig.4. We can observe that $$$\small{SubjRmax}$$$ and $$$\small{SubjRiskMass}$$$ decrease with M. Fig.5 provides the plots of $$$\small{MSF}$$$ and $$$\small{rMSF}$$$ showing their convergence with M. A fit with the model: $$\small{MSF=1+A·M^{-p} [Eq.4]}$$ returns p=0.90 for $$$\small{MSF}$$$ and p=1.12 for $$$\small{rMSF}$$$, leading to the safety margins for 30 $$$\small{NHMs^{VOP}}$$$ of 1.57 and 1.31 respectively.Discussion and Conclusion
The described approach allows one to verify in simulation the safety level of a given VOP set and to determine the appropriate safety margins. The R-criterion gives directly the worst-case ratio of $$$\small{SAR}$$$ to $$$\small{SAR^{*}}$$$ and thus does not rely on Monte-Carlo simulations across RF shims4. We showed that, according to the criterion used, using only a few models for computing the VOPs requires exceedingly restrictive MSFs possibly leading to pTX performance issues. Reducing the MSF in turn poses a high risk of underestimating the local SAR due to variations in head size and position.Based on our simulation data, above 30 NHMs are recommended to compute the VOPs. To construct final VOPs on the entire database of 68 NHMs, we applied $$$\small{MSF}$$$ of 1.28 according to empirical formula 1+12.3M-0.9. Note that the form of the latest depends on additional safety margins. Provided our database is representative enough, we can use the simulation-based results for pediatric exams.
Acknowledgements
This work received the financial support of the French National research Agency (Collaborative research project MOSAR ANR-21-CE19-0028). We acknowledge the financial support of the Cross-Disciplinary Program on Numerical Simulation of CEA, the French Alternative Energies and Atomic Energy Commission. Edouard Chazel (University of Paris-Saclay, CEA) is thanked for assembling the RF coil.References
- Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med . 2011 Nov; 66(5):1468-76
- Sydney N Williams et al. Ultra-high field MRI: parallel-transmit arrays and RF pulse design. 2023 Phys. Med. Biol. 68 02TR02
- Boulant, N. et al. (2018) ‘Workflow proposal for defining SAR safety margins in parallel transmission’, in Proceedings of the 26th Annual Meeting of ISMRM. Paris.
- Ingmar Graesslin, Hanno Homann H, Biedere S, et al. A Specific Absorption Rate Prediction Concept for Parallel Transmission MR. Magnetic Resonance in Medicine 68:1664–1674 (2012)
- Gras V, Boulant N, Luong M. A mathematical analysis of clustering-free local SAR compression algorithms for MRI safety in parallel transmission. IEEE Transactions on Medical Imaging 2023
- Preliminary SNR comparison between the 11.7T Iseult RF coil and its twin coil at 7T. Amadon A, Gras V, Chazel E, et al. Proc. Intl. Soc. Mag. Reson. Med. 31 (2023). 4076
- Delbany, M. et al. ‘Variability of the specific absorption rate in the child’s head using a transmit array head coil at 7T: a simulation study’. ISMRM 2021, p. 3.
- International Electrotechnical Commission, “International standard, Medical equipment – IEC 60601-2-33: Particular requirements for the safety of Magnetic resonance equipment (3rd edition),” 2010.
Figures
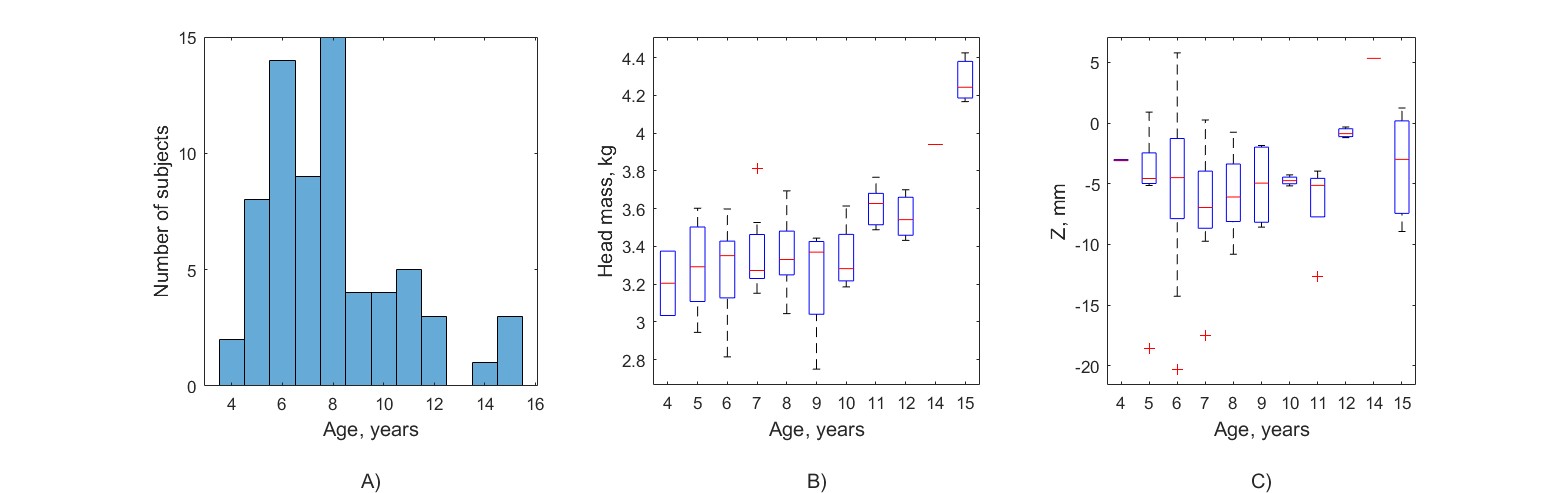
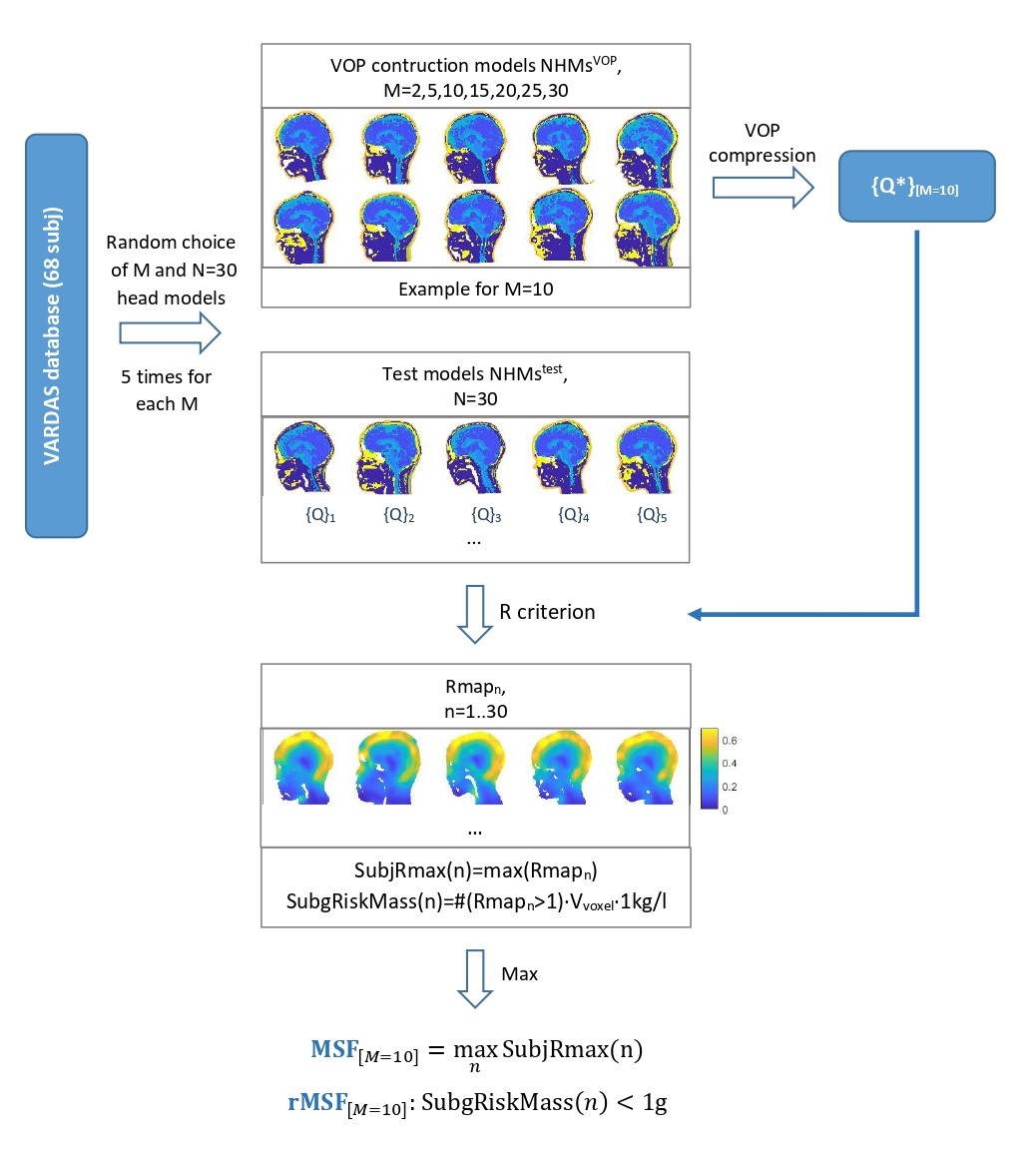
Figure 2. The simulation database VARDAS containing 68 numerical head models (NHM) of children aged 4-16 years was used. From this database, we chose subgroups NHMsVOP of size M (M varied from 2 to 30) to construct VOPs. These latest were tested on other 30 NHMstest from the database, providing R maps and corresponding Multiplicative Safety Factors. For each M, random selection of NHMVOP and NHMtest was performed 5 times.
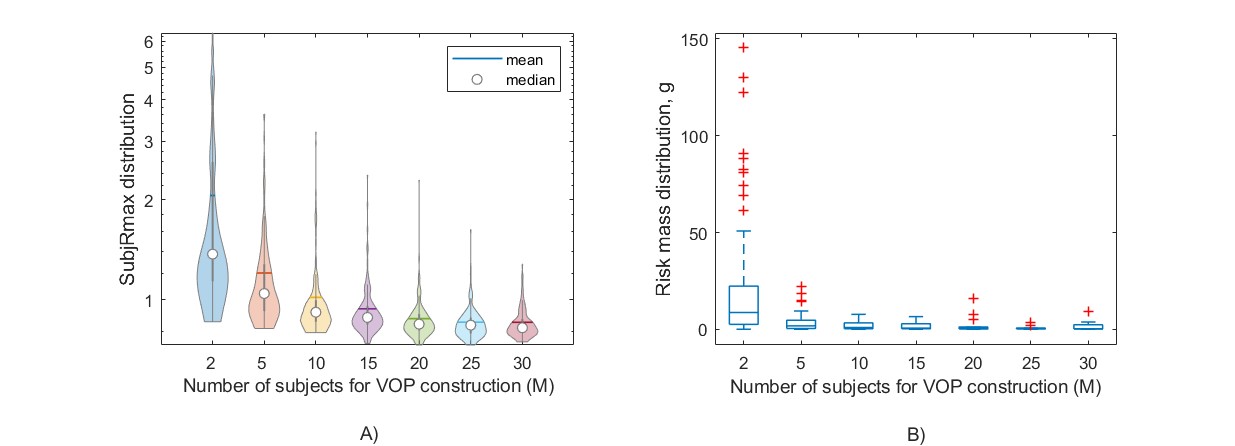
Figure 3. Test of the VOPs constructed using NHMsVOP subgroups with different sizes M (2 to 30) on 30 NHMstest. In (A), the distribution of the maximum R criterion for NHMstest (SubjRmax) as a function of M is shown on a semi-logarithmic scale. (B) shows the distribution of the risk mass with R>1 for test subjects (SubjRiskMass) against M.