0789
Individual voxel models for head SAR estimation1Magnetic Resonance Center, Max Planck Institute for Biological Cybernetics, Tübingen, Germany, 2Department for Biomedical Magnetic Resonance, University of Tübingen, Tübingen, Germany
Synopsis
Keywords: High-Field MRI, Segmentation, voxel models, ultra-high field, EM simulation
Motivation: Accurate human tissue models for simulation of RF power absorption are a key safety requirement for transmit coil development especially at ultra-high field.
Goal(s): To create individual voxel models of the human head and torso.
Approach: A pipeline for head and torso segmentation was developed based on a 3T multi-contrast protocol and tailored post-processing. The resulting voxel models were used for electromagnetic simulation of a self-developed Tx array at 9.4T.
Results: Strong agreement was found between measured and simulated B1+ maps using the generated voxel model. Simulated worst-case SAR distributions differed significantly between individual and ‘off-the-shelf’ voxel models.
Impact: We present a pipeline for the creation of individual human tissue voxel models covering head and torso, which is based on multi-contrast MR image segmentation. This meets a central need in safety-related simulations of ultra-high field RF coil arrays.
Introduction
The RF energy absorbed by tissue is one of the major safety concerns in MRI, especially for multi-channel transmit coil (Tx) development at ultra-high field, where Specific Absorption Rate (SAR) hotspots are more spatially confined and depend on the individual’s anatomy and position inside the coil1,2. The required real-time SAR supervision is usually achieved by a compressed description of the complex E-field formation via so-called virtual observation points3. For that, tissue models for RF safety simulations of Tx coil arrays should represent the measured population as well as possible, which is often not the case with commercially available ‘off-the-shelf’ models. Thus, deviations between models and actual measured subjects are usually accounted for by rather arbitrary safety factors in SAR estimation. Several projects have attempted to addressed this uncertainty4,5, but they have neither addressed the impact of individual tissue models on VOP SAR nor included upper body anatomy6. Here, we present first results of creating models based on segmented MR images of the head and torso.Methods
MR measurementsThree healthy volunteers were scanned on a Siemens Healthineers PrismaFit 3 T whole-body MRI using a 20-channel head coil and a spine+breast array. For the head, imaging was performed with 1 mm resolution using an MPRAGE with CSF nulled signal, a T2-weighted 3D TSE with variable flip-angle (SPACE), an ultra-short TE sequence and a Fat-Water DIXON GRE. For the torso, an MPRAGE, a DIXON GRE and the 3D TSE were acquired at a resolution of 2 mm with anterior-posterior phase encoding without any respiratory/pulse triggering.
Tissue segmentation
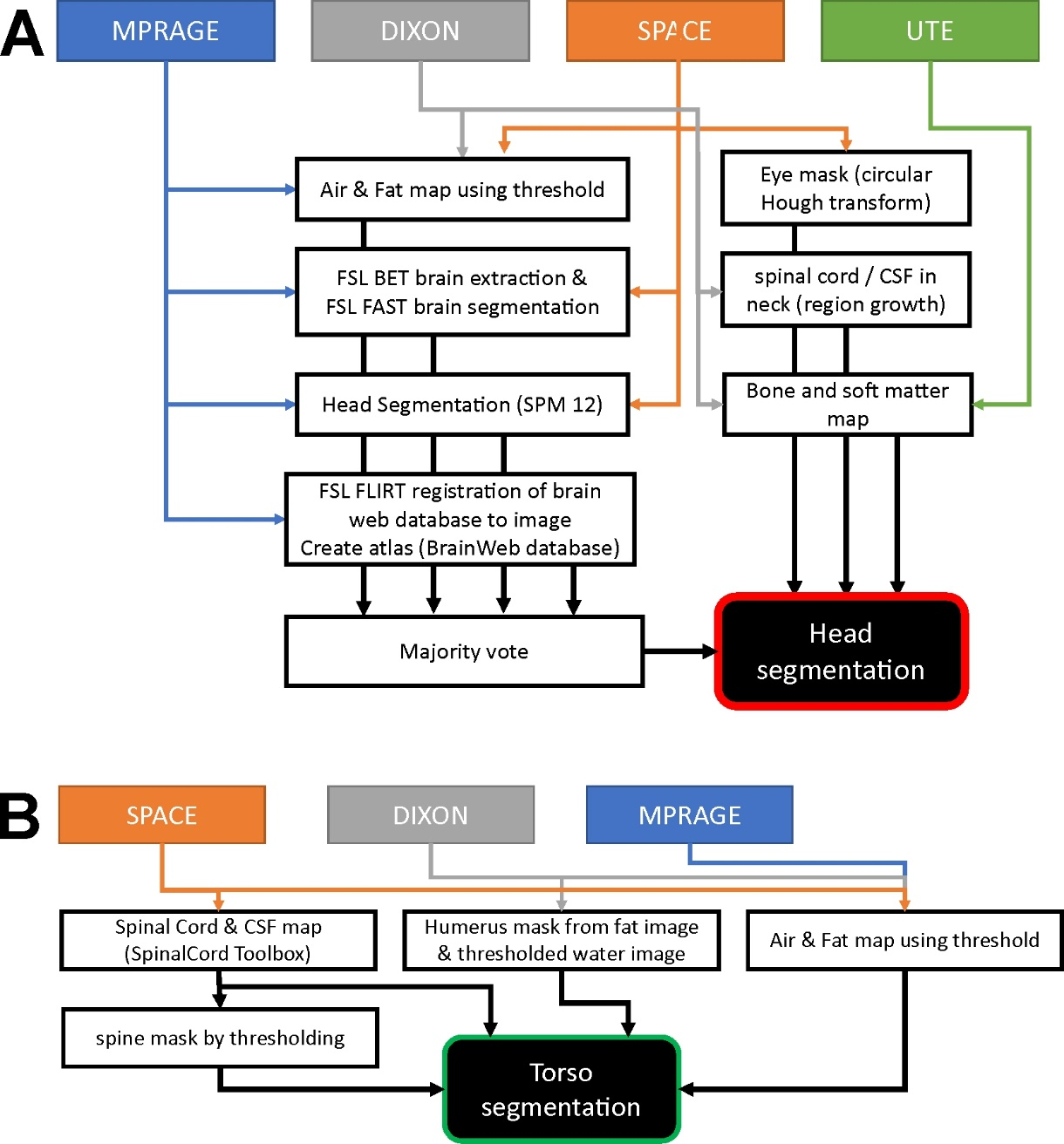
The images were segmented into eight different classes separately for head and body, as shown schematically in Fig. 1. A majority vote using the assigned tissue type by three different segmentation methods (FSL7,8, SPM129, BrainWeb database10) was performed and combined with an air/fat mask. The eye mask was created using a circular Hough transform after manually selecting the seed points. The torso segmentation included the extraction of the spinal cord and CSF11, the creation of a mask for the humerus bone, and of air and fat. The torso segmentation was up-sampled to 1 mm resolution and a combined model was created by warping the edge slices in the lower head and upper torso to create a smooth transition.
Simulation of RF fields
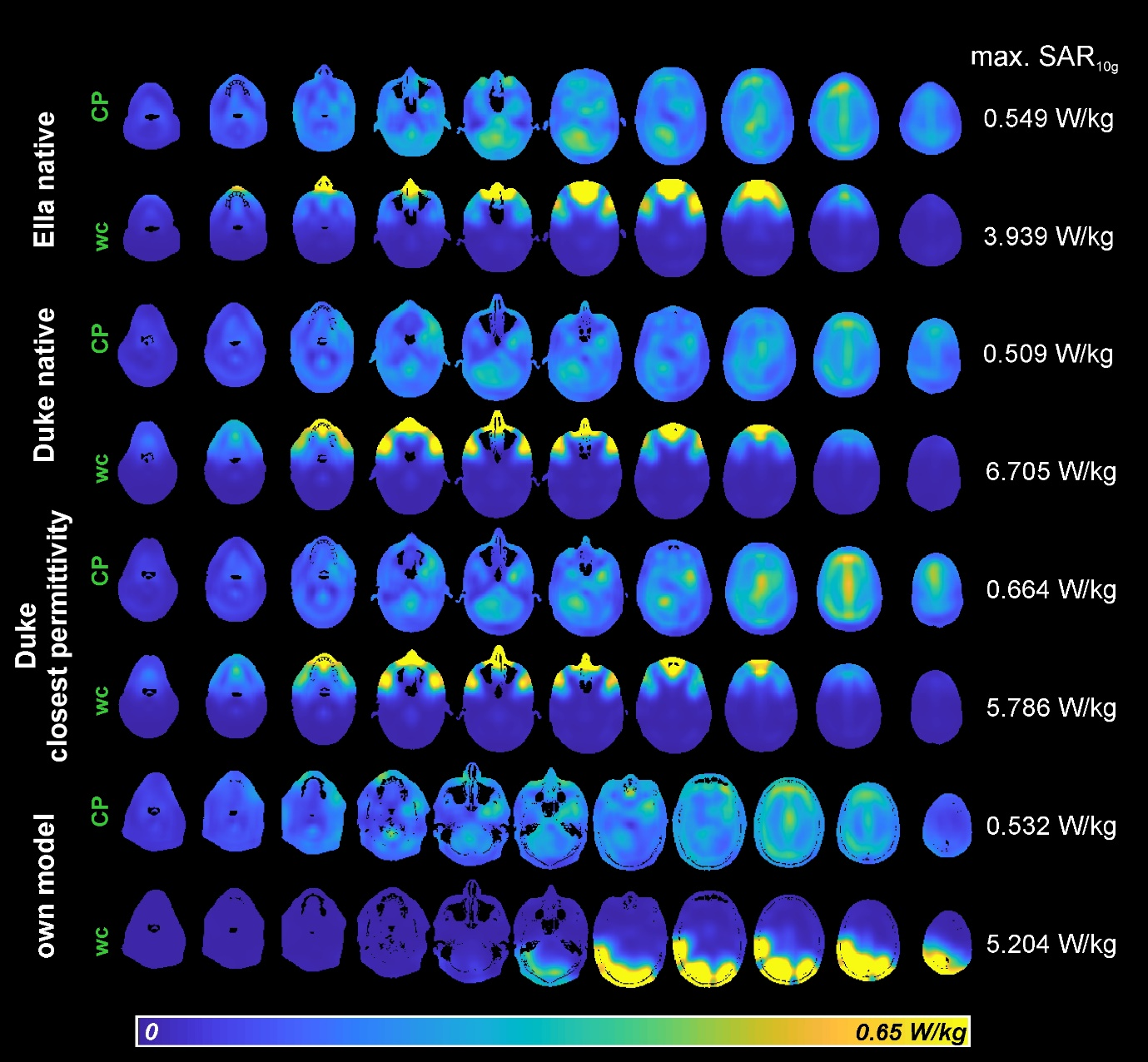
The typical position of one of the three volunteers in the coil was determined by placing reference tubes at the edges of a 16 Tx array12 and performing an MPRAGE scan with 0.8 mm resolution at our 9.4 T MRI scanner. Additionally, we acquired single-channel B1+ maps13. The segmented model was placed accordingly into the corresponding coil model for the RF simulations with CST (Dassault Systèmes, Vélizy-Villacoublay, France). Additional simulations were performed to estimate the impact of a reduced number of tissues in the generated voxel models compared to the ‘off-the-shelf’ models14 (Duke and Ella). For this, tissue types not present in our model were replaced in the Duke model by the tissue type with the closest matching permittivity. The resulting SAR10g values were compared to those obtained from the native model for different RF modes including CP and worst-case15.
Results
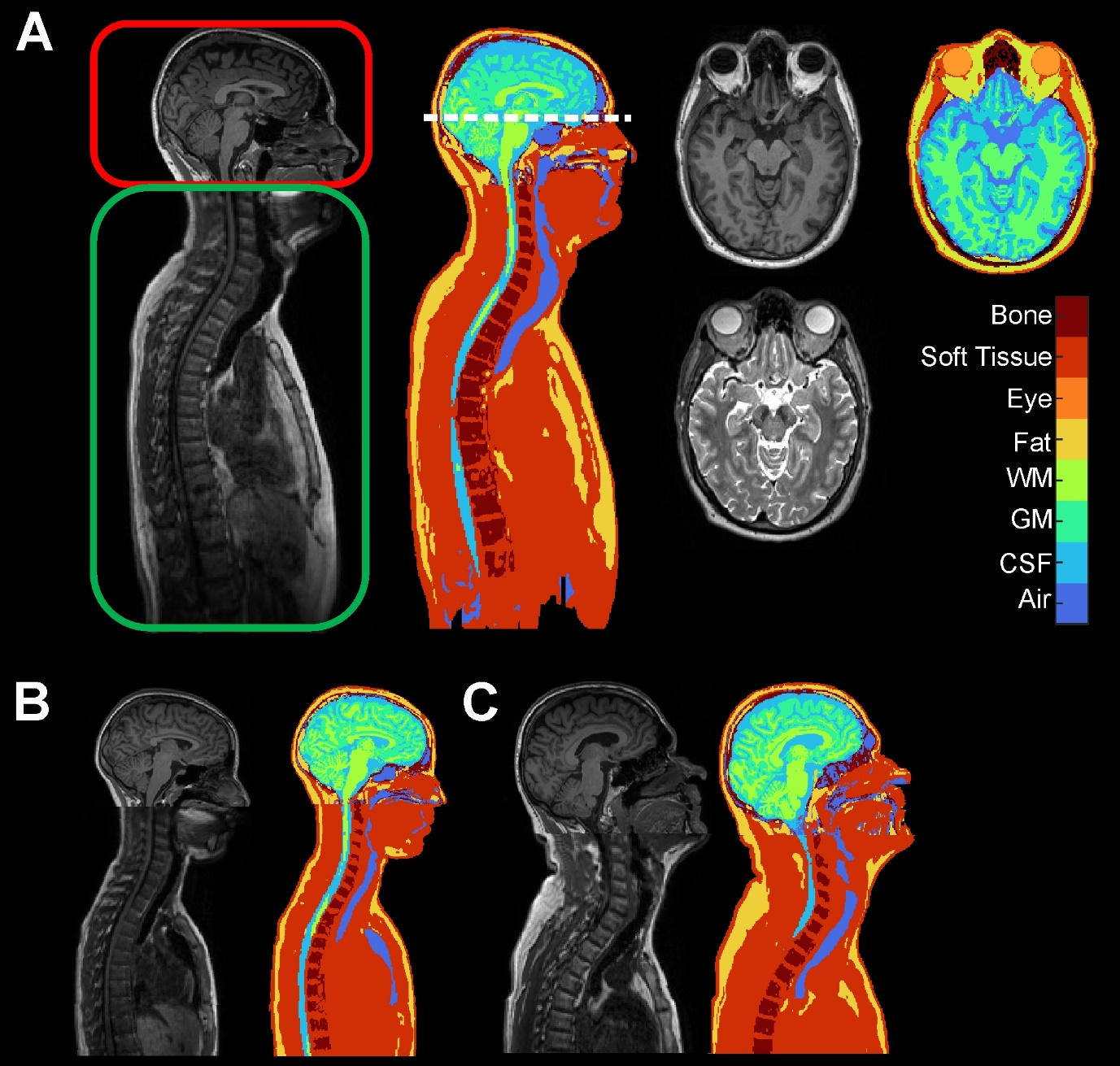
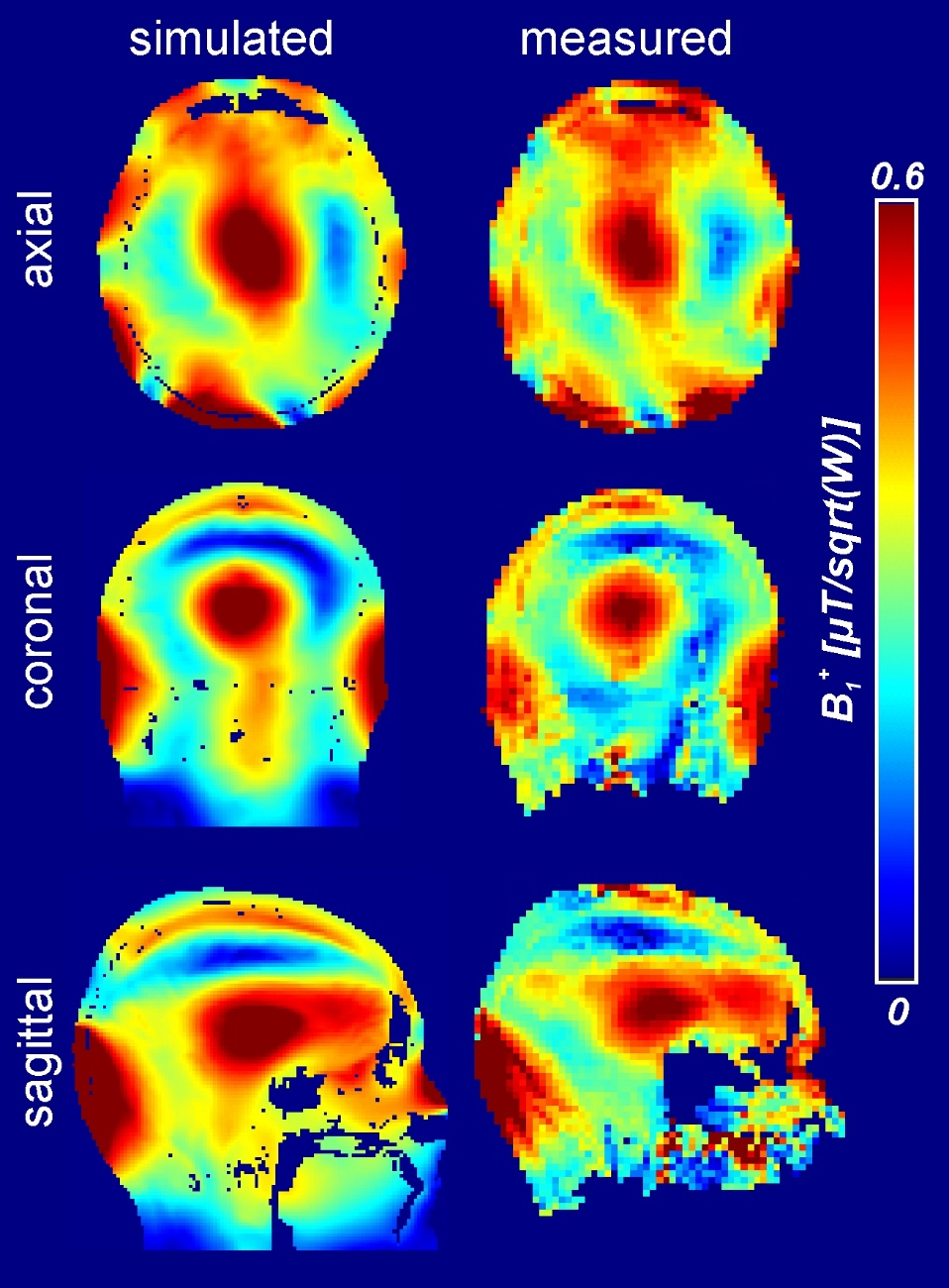
The tissue models created by the developed pipeline are shown in Fig. 2. The simulated and measured B1+-maps of the actual human body are in good agreement (Fig. 3), indicating a realistic modeling in the simulations. Reducing the number of tissue types by replacing them with the closest permittivity leads to an increase of simulated SAR10g in the CP mode (Fig. 4). Although no change in the SAR distribution of the worst-case mode is observed, simulated SAR10g was 14 % lower for the reduced tissue model. Interestingly, the self-created model shows a very different worst case SAR distribution.Discussion and Conclusion
The proposed pipeline allows the creation of voxel models covering the head and torso for transmit field and SAR simulations. We have focused on the accurate modeling of the head and torso, but an extension to other body regions should be feasible if imaging artifacts e.g. due to breathing can be avoided by triggering. We plan the creation of more models covering a wider age-range in the near future. Since the self-created models have a reduced number of tissue types, which may affect the accuracy of SAR simulations, further simulations are needed to investigate the impact of this simplification and to compare the chosen approach to other clustering methods.Acknowledgements
Financial support of the Max-Planck-Society and ERC Advanced Grant “SpreadMRI”, No 834940 is gratefully acknowledged.References
1. Avdievich NI., Hoffmann J, Shajan G, et al. Evaluation of transmit efficiency and SAR for a tight fit transceiver human head phased array at 9.4 T. NMR Biomed. 2017;30(2):e3680. doi:10.1002/nbm.3680
2. Williams SN, McElhinney P, Gunamony S. Ultra-high field MRI: parallel-transmit arrays and RF pulse design. Phys Med Biol. 2023;68(2):02TR02. doi:10.1088/1361-6560/aca4b7
3. Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med. 2011;66(5):1468-1476. doi:10.1002/mrm.22927
4. Brink WM, Yousefi S, Bhatnagar P, Remis RF, Staring M, Webb AG. Personalized local SAR prediction for parallel transmit neuroimaging at 7T from a single T1-weighted dataset. Magn Reson Med. 2022;88(1):464-475. doi:10.1002/mrm.29215
5. Kalloch B, Bode J, Kozlov M, et al. Semi-automated generation of individual computational models of the human head and torso from MR images. Magn Reson Med. 2019;81(3):2090-2105. doi:10.1002/mrm.27508
6. Berezko E, Solomokha G, Scheffler K, Avdievich N. 2703: Numerical Evaluation of Specific Absorption Rate of Local Transceiver Coil Arrays for Ultra-High Field MRI with Different Local Mesh Properties. 2023 ISMRM & ISMRT Annual Meeting & Exhibition (ISMRM 2023), Toronto (CA).
7. Smith SM. Fast robust automated brain extraction. Hum Brain Mapp. 2002;17(3):143-155. doi:10.1002/hbm.10062
8. Zhang Y, Brady M, Smith S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE Trans Med Imaging. 2001;20(1):45-57. doi:10.1109/42.906424
9. SPM12 Software - Statistical Parametric Mapping. https://www.fil.ion.ucl.ac.uk/spm/software/spm12/.
10. Aubert-Broche B, Griffin M, Pike GB, Evans AC, Collins DL. Twenty New Digital Brain Phantoms for Creation of Validation Image Data Bases. IEEE Trans Med Imaging. 2006;25(11):1410-1416. doi:10.1109/TMI.2006.883453
11. De Leener B, Lévy S, Dupont SM, et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. NeuroImage. 2017;145:24-43. doi:10.1016/j.neuroimage.2016.10.009
12. Avdievich NI, Giapitzakis IA, Bause J, Shajan G, Scheffler K, Henning A. Double-row 18-loop transceive-32-loop receive tight-fit array provides for whole-brain coverage, high transmit performance, and SNR improvement near the brain center at 9.4T. Magn Reson Med. 2019;81(5):3392-3405. doi:10.1002/mrm.27602
13. Bosch D, Bause J, Geldschläger O, Scheffler K. Optimized ultrahigh field parallel transmission workflow using rapid presaturated TurboFLASH transmit field mapping with a three-dimensional centric single-shot readout. Magn Reson Med. 2023;89(1):322-330. doi:10.1002/mrm.29459
14. Christ A, Kainz W, Hahn EG, et al. The Virtual Family—development of surface-based anatomical models of two adults and two children for dosimetric simulations. Phys Med Biol. 2009;55(2):N23. doi:10.1088/0031-9155/55/2/N01
15. Glang F, Bosch D, Solomakha G, Bause J, Avdievich N, Scheffler K. SAR safety procedure for self-built pTx human head RF array coils at 9.4T. Submitted to 2024 ISMRM & ISMRT Annual Meeting & Exhibition, Singapur.
Figures