0787
From Low-Field to High Risk: Analyzing RF Heating of Neuromodulation and Cardiac Devices during MRI at 0.55T relative to 1.5T1Radiology, Northwestern University, Chicago, IL, United States, 2Biomedical Engineering, Northwestern University, Evanston, IL, United States, 3Radiology, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Low-Field MRI, Safety, Medical Implants
Motivation: Radiofrequency-induced heating of elongated medical implants during MR imaging on newly introduced commercial 0.55T systems has not been thoroughly investigated.
Goal(s): We aim to evaluate and compare the RF heating of elongated medical implants during MRI at 0.55T and 1.5T scanners.
Approach: Neurological and cardiac implant leads were routed along different trajectories inside a tissue mimicking gel phantom, and the temperature increase during MRI at 0.55T and 1.5T was measured at the lead tip.
Results: For certain implant configurations, RF heating at 0.55T MRI can be an order of magnitude higher than that at 1.5T.
Impact: Our findings show that unsafe levels of RF heating, exceeding those at higher field strengths, are possible on commercial 0.55T MRI systems for certain implant configurations. Therefore, extra caution should be taken during low-field MRI of patients with long implants.
Introduction
By 2030, an estimated one-sixth of the global population will be 60 years of age or older1, with a substantial proportion managing chronic diseases necessitating continuous monitoring and timely interventions2. This scenario is forecasted to propel the active implantable medical devices (AIMDs) market to an impressive $42 billion valuation by 2031, with cardiac pacemakers, implantable cardioverter defibrillators, and neurostimulators emerging as pivotal contributors to this growth3. For the past twenty years, concerted efforts within the medical community have sought to render MRI accessible for AIMD patients, although significant challenges persist4-12. The recent advent of low-field MRI scanners (0.55 T and below) introduces a fresh avenue. MRI at these field strengths has been hypothesized as a potential solution of imaging patients with implants. However, the premature designation of these scanners as "implant-friendly" raises concerns. Although they mitigate issues associated with metal artifacts and device dislodgement risks due to reduced magnetic forces, there is a conspicuous absence of RF safety data to corroborate their safety profile.This scenario delineates a pivotal juncture where low-field scanners, while potentially transformative for many, concurrently pose substantial risks for others. The rise in off-label MRI scans among AIMD patients, driven by urgent medical needs and motivated by influential publications advocating off-label MRI usage, exacerbates this dilemma. Often, the assumption of RF safety in these studies is premised on limited phantom experiments, typically involving scant RF heating measurements markedly falling short of the FDA’s meticulous testing recommendations encompassing hundreds of thousands of scenarios. Given the intricacies of MRI RF heating phenomenon, these findings are disconcerting.
Here we report the results of RF heating measurements during MRI of commercial deep brain stimulation (DBS) and cardiac stimulation devices under various configurations. We compare the RF heating generated by these implants during MRI scans at 1.5T and 0.55T scanners. Our data illustrate stark disparities in RF heating at 0.55T contingent on implant type and length, with variations oscillating between twenty-five times less to nine times more than that observed with 1.5T scanners.
Methods
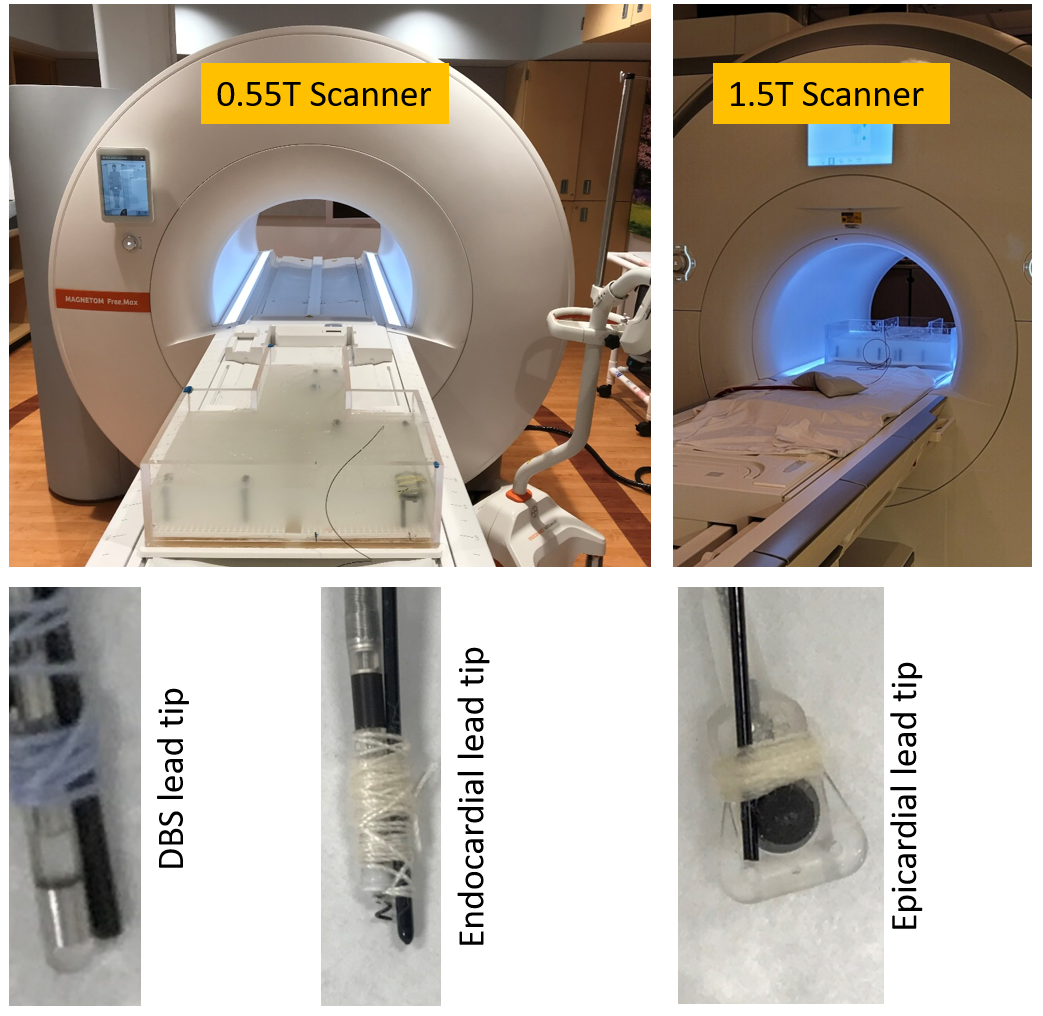
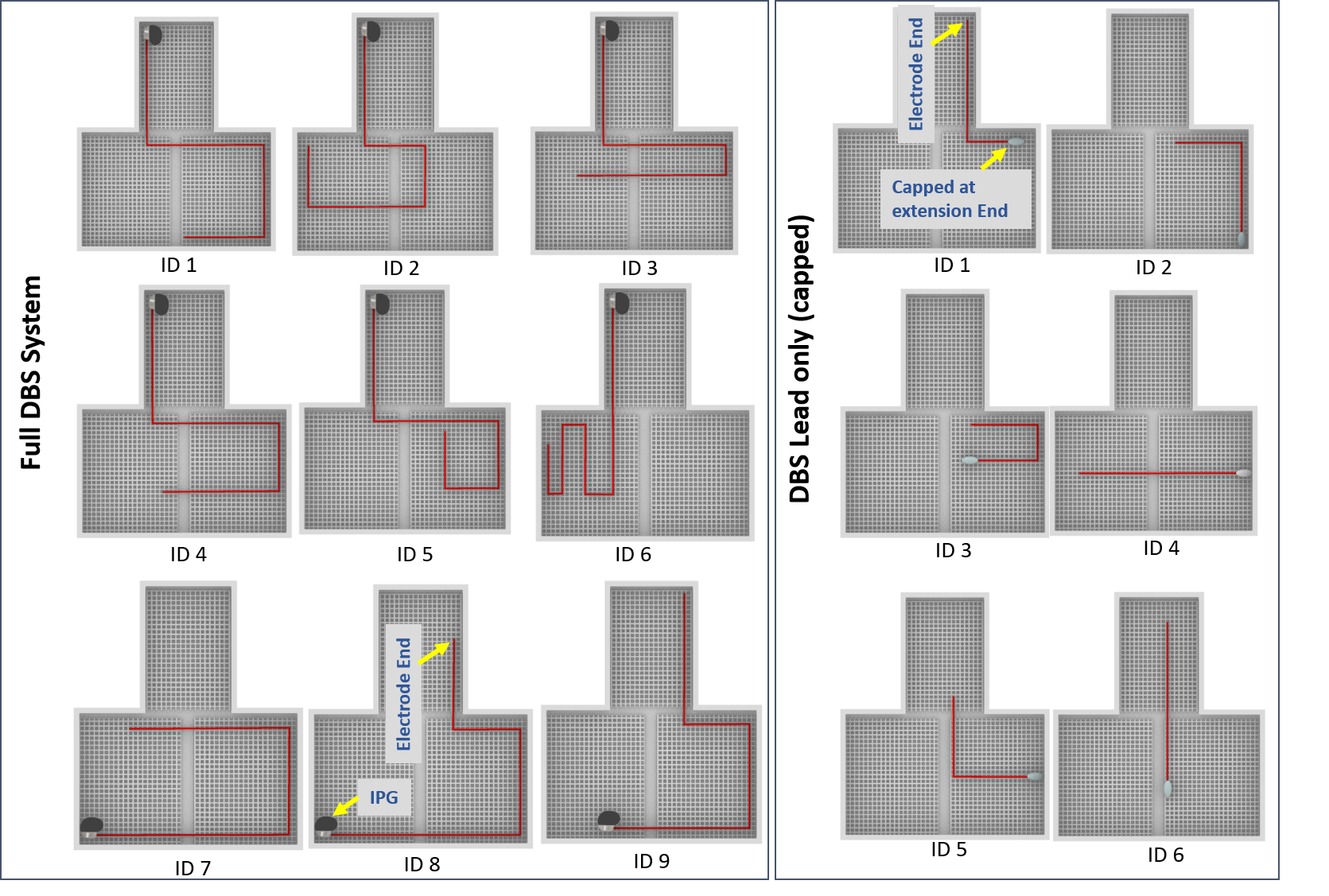
We assessed RF-induced heating of DBS and cardiac pacing devices at Siemens 1.5T Aera and 0.55T FreeMax scanners. We used a fiber optic temperature sensor (Osensa) on the DBS and cardiac leads' distal contacts to monitor temperature changes in a tissue simulating polyacrylic acid (PAA) gel phantom (conductivity = 0.47 S/m, Permittivity = 88 at 64 MHz) (Figure 1). Implant devices were placed in various trajectories within the phantom (Figures 2 & 3), and heating was recorded during chest landmark scans with spin echo sequences at identical settings (TA = 4:21 min, B1+rms = 4.5 μT). For DBS lead-only cases, the extra-cranial end was capped.Results
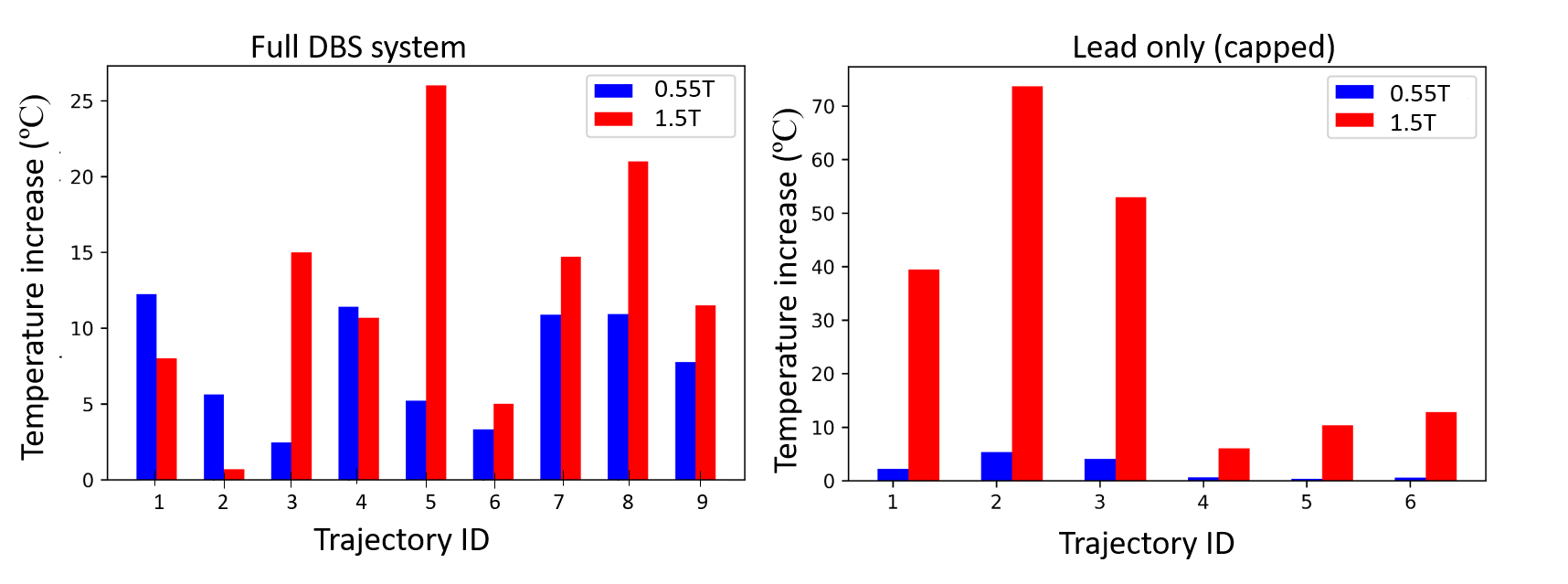
The temperature increases at the tip of the DBS lead are depicted in Figure 4. For trajectory 'ID 2' within the complete DBS system, the temperature increase at 0.55T was over seven times higher than at 1.5T MRI (5.62 vs. 0.72 ºC). Similarly, the temperature rise for trajectories 'ID 1' and 'ID 4' was higher by 51% and 7%, respectively, at the 0.55T scanner compared to the 1.5T scanner (12.23 vs. 8.1 ºC for 'ID 1' and 11.41 vs. 10.68 ºC for 'ID 4'). The mean temperature increase was 7.8 ± 3.5 ºC at 0.55T and 12.5 ± 7.3 ºC at 1.5T scanner.For DBS lead-only cases, RF-induced temperature increase at the lead tip was significantly lower at 0.55T MRI compared to that at 1.5T MRI for all the tested configurations. The mean temperature increase was 2.2 ± 1.9 ºC at 0.55T and 32.5 ± 24.9 ºC at 1.5T, indicating an approximately 15-fold higher average heating at 1.5T compared to that at 0.55T.
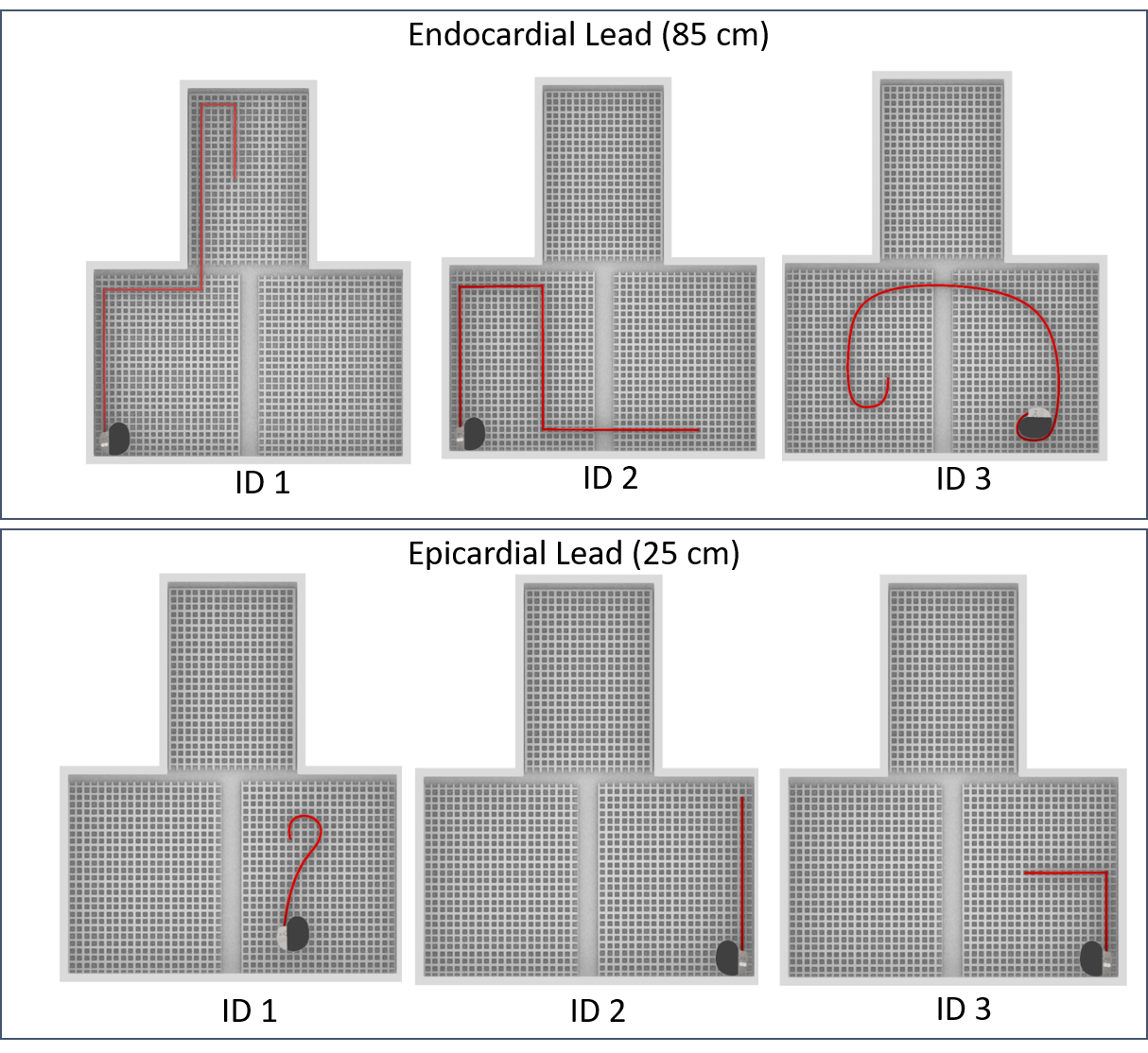
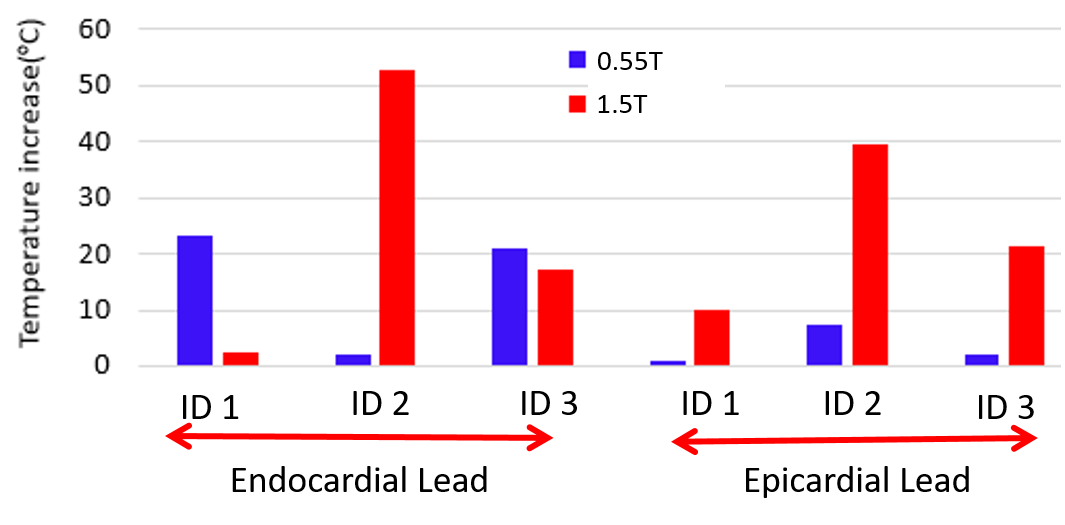
Additionally, as Figure 5 indicates, the RF heating at the tip of the endocardial lead was 9-folds higher at 0.55T than at 1.5T (23.08 vs. 2.51 ºC) for 'ID 1' and 21% higher for 'ID 3' (21.09 vs. 17.36 ºC). Conversely, RF heating for the epicardial lead at 0.55T was substantially lower than at 1.5T for all three evaluated trajectories.
Discussions and Conclusions
RF heating of implanted leads depends on the configuration and length, with resonance from varying lengths and RF frequencies playing a key role. Longer leads near resonance at lower MRI field strengths, leading to significant heating, even surpassing the heating observed at higher field strengths. Temperature increases at low-field scanners may surpass safe thresholds with longer implants, questioning the presumed safety of such scanners for active implants.Acknowledgements
This work was supported by NIH grant R01EB033864.References
[1] WHO. Aging and Health (https://www.who.int/news-room/fact-sheets/detail/ageing-and-health#:~:text=By%202030%2C%201%20in%206,will%20double%20(2.1%20billion), 2022).
[2] C. J. Murray et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. The Lancet 386, 2145-2191 (2015).
[3] Global Opportunity Analysis and Industry Forecast, 2020 - 2027: Medical Implants Market By Type (Orthopedic Implants, cardiac implants, Stents, Spinal Implants, Neurostimulators, dental implants, Breast Implants, facial Implants) and By Materials (Metallic, Ceramic, Polymers, Natural) (https://www.alliedmarketresearch.com/request-sample/71).
[4] K. B. Baker et al., F. G. Shellock, and A. R. Rezai, "Reduction of magnetic resonance imaging-related heating in deep brain stimulation leads using a lead management device," Neurosurgery, vol. 57, no. 4 Suppl, pp. 392-7; discussion 392-7, Oct 2005.
[5] L. Golestanirad et al., "RF-induced heating in tissue near bilateral DBS implants during MRI at 1.5 T and 3T: The role of surgical lead management," (in English), Neuroimage, vol. 184, pp. 566-576, Jan 1 2019.
[6] B. T. Nguyen et al., "Safety of MRI in patients with retained cardiac leads," Magn Reson Med, vol. 87, no. 5, pp. 2464-2480, May 2022.
[7] Y. Eryaman et al., "Reduction of the radiofrequency heating of metallic devices using a dual-drive birdcage coil," Magn Reson Med, vol. 69, no. 3, pp. 845-52, Mar 1 2013.
[8] Y. Wang et al., "A technique for the reduction of RF-induced heating of active implantable medical devices during MRI," Magn Reson Med, vol. 87, no. 1, pp. 349-364, Jan 2022.
[9] F. Jiang et al., "Modifying the trajectory of epicardial leads can substantially reduce MRI‐induced RF heating in pediatric patients with a cardiac implantable electronic device at 1.5 T," Magnetic resonance in medicine, vol. 90, no. 6, pp. 2510-2523, 2023.
[10] J. Vu et al., "A comparative study of RF heating of deep brain stimulation devices in vertical vs. horizontal MRI systems," Plos one, vol. 17, no. 12, p. e0278187, 2022.
[11] P. Sanpitak et al., "Low-field MRI’s Spark on Implant Safety: A Closer Look at Radiofrequency Heating."
[12] B. Guerin et al., "Parallel transmission to reduce absorbed power around deep brain stimulation devices in MRI: Impact of number and arrangement of transmit channels," Magn Reson Med, vol. 83, no. 1, pp. 299-311, Jan 2020.
Figures