0785
Diagnosis of muscle-invasive urothelial carcinoma with variant histology using biparametric MRI and VI-RADS in a radical cystectomy cohort1Radiology, Keio University School of Medicine, Tokyo, Japan, 2Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 3Radiology, University Medical Center Groningen, Groningen, Netherlands, 4Urology, Keio University School of Medicine, Tokyo, Japan, 5Biostatistics, University of Tsukuba, Ibaraki, Japan, 6Radiology, National Defence Medical College, Saitama, Japan, 7Urology, Tokyo Medical and Dental University Graduate School, Tokyo, Japan, 8Radiology, University of Wisconsin–Madison, Madison, WI, United States, 9Urology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: Urogenital, Bladder, VI-RADS
Motivation: To determine if contrast-free biparametric MRI (bpMRI), which offers potential cost, comfort and safety advantages, could replace multiparametric MRI (mpMRI) in diagnosing muscle-invasive bladder cancer (MIBC) in patients with urothelial carcinoma of variant histology (VUC).
Goal(s): To compare the diagnostic accuracy of bpMRI and conventional mpMRI for detecting MIBC in patients with VUC who underwent radical cystectomy (the optimal reference standard).
Approach: A retrospective, multicenter diagnostic study using radical cystectomy as the reference standard.
Results: The diagnostic performance of bpMRI was confirmed to be weaker than that of mpMRI in the assessment of muscle invasion in bladder VUC.
Impact: When applying VI-RADS, bpMRI had weaker diagnostic performance than mpMRI in assessing muscle invasion in patients with bladder VUC who had radical cystectomy (the optimal reference standard). Consequently, we recommend employing mpMRI-based methods for evaluating muscle invasion in bladder VUC.
Introduction
Bladder cancer (BC) is the seventh-most prevalent cancer globally. Most BCs are categorized histologically as pure urothelial carcinoma (UC)1. UC with variant histology (VUC) accounts for 5%–10% of all UCs and is considered more aggressive than pure UC2-4. Recent studies reported that the accuracy of contrast-free bpMRI [including T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI)] for diagnosing muscle-invasive BC (MIBC) in patients with VUC was inferior to that of standard mpMRI [including T2WI, DWI, and dynamic contrast-enhanced (DCE)-MRI]5. However, studies investigating this topic have typically included transurethral resection of bladder tumor (TURB) as a reference standard, and there is a potential for upstaging by radical cystectomy (the optimal reference standard). Furthermore, to our knowledge, no prior studies on this topic have included solely patients who had radical prostatectomy without neoadjuvant chemotherapy. Therefore, we aimed to compare the performance of bpMRI and mpMRI for diagnosing muscle-invasive bladder VUC in patients who underwent radical cystectomy without neoadjuvant chemotherapy.Methods
This retrospective, multicenter study included 71 consecutive patients with pathologically confirmed VUC, who underwent bladder mpMRI before radical cystectomy between July 2007 and September 2019 from 3 centers (Fig.1). mpMRI of the bladder was performed using a 1.5-T MR system with a body-array coil (Fig.2). Three board-certified radiologists, blinded to surgical/pathological findings, evaluated muscle invasion by both bpMRI and mpMRI using the Vesical Imaging-Reporting and Data System (VI-RADS). bpMRI-based and mpMRI-based VI-RADS scores were determined based on published recommendations6. Interobserver agreement was assessed using Fleiss kappa values. The performance of the VI-RADS scores in predicting muscle invasion was assessed using areas under receiver operating characteristic (ROC) curves (AUCs). The Wald test was used to compare accuracy, specificity, and sensitivity between bpMRI and mpMRI.Results
Of the 71 patients included, 47 (66.2%) had pathologically proven MIBC and 24 (33.8%) had non-MIBC (NMIBC). Baseline characteristics of the patients and bladder tumors are summarized in Figure 3. The bpMRI and mpMRI Fleiss kappa scores for the three readers were 0.76 and 0.81 for bpMRI-based and mpMRI-based VI-RADS scoring, respectively. Figure 4 displays the diagnostic performance of the readers for MIBC. For all readers, the AUCs for bpMRI were significantly lower than those for mpMRI (reader 1, 0.895 vs. 0.921, p=0.008; reader 2, 0.883 vs. 0.904, p=0.004; reader 3, 0.8730 vs. 0.901, p=0.014). At a VI-RADS cut-off value of 4, sensitivity was significantly lower for bpMRI than for mpMRI for all readers (reader 1, 68.0% vs. 80.9%, p=0.015; reader 2, 66.0% vs. 80.9%, p=0.012; reader 3, 66.0% vs. 78.7%, p=0.016), while specificity did not differ significantly between bpMRI and mpMRI for any readers (reader 1, 91.7% vs. 95.8%, p=0.42; reader 2, 87.5% vs. 91.7%, p=0.35; reader 3, 87.5% vs. 91.7%, p=0.35). When the VI-RADS cut-off value was 3, no significant differences in sensitivity between bpMRI and mpMRI were identified for any readers (reader 1, 89.4% vs. 93.6%, p=0.20; reader 2, 89.4% vs. 91.5%, p=0.42; reader 3, 89.4% vs. 91.5%, p=0.42), and only for reader 1, specificity was significantly lower for bpMRI than for mpMRI (reader 1, 70.8% vs. 79.2%, p=0.048; reader 2, 75.0% vs. 79.2%, p=0.12; reader 3, 70.8% vs. 75.0%, p=0.095). Figure 5 displays a VUC where bpMRI underestimated the extent of the disease.Discussion
We investigated whether bpMRI could effectively replace mpMRI in the evaluation of muscle invasion in a multicenter cohort of patients with bladder VUC who all underwent radical cystectomy without neoadjuvant chemotherapy. We found that the AUCs of bpMRI-based VI-RADS were considerably lower than those of conventional mpMRI-based VI-RADS in identifying MIBC. Moreover, when the VI-RADS cut-off value was set at 4 (muscle invasion is likely), the sensitivity of bpMRI for evaluating muscle invasion was significantly lower than that of mpMRI for all readers. These findings were comparable to those of a previous study that used TURB as a reference standard5. By omitting the DCE sequence, bpMRI shortens scanning times, avoids potential complications due to the use of contrast media, and lowers direct costs. However, based on the direct histopathological correlation established in the present study, it appears that the substantial cytoplasmic presence, coupled with fluctuating cell density and microinvasive patterns penetrating the muscular layer, induced heterogeneity in the DWI results within the muscle layer. The indistinct DWI signals could potentially have played a role in the underestimation of muscle invasion in VUC.Conclusion
Using radical cystectomy as a reference standard, this study confirmed that bpMRI-based VI-RADS scores have lower diagnostic efficacy than mpMRI-based VI-RADS scores for diagnosing MIBC in patients with VUC.Acknowledgements
The authors thank Mr. Hayato Ogawa for his help with data collection.References
1. Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol 2017;71:96–108.
2. Wang G, McKenney JK. Urinary bladder pathology: World Health Organization Classification and American Joint Committee on Cancer staging update. Arch Pathol Lab Med 2019;143:571–7.
3. Black PC, Brown GA, Dinney CP. The impact of variant histology on the outcome of bladder cancer treated with curative intent. Urol Oncol 2009;27:3–7.
4. Witjes JA, Bruins HM, Carrión A, et al. European Association of Urology Guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2023 guidelines. Eur Urol 2021;79:82–104.
5. Arita Y, Kwee TC, Woo S, et al. Biparametric versus Multiparametric Magnetic Resonance Imaging for Assessing Muscle Invasion in Bladder Urothelial Carcinoma with Variant Histology Using the Vesical Imaging-Reporting and Data System. Eur Urol Focus 2023:S2405-4569(23)00186-4.
6. Panebianco V, Narumi Y, Altun E, et al. Multiparametric magnetic resonance imaging for bladder cancer: development of VI-RADS (Vesical Imaging-Reporting and Data System). Eur Urol 2018;74:294–306.
Figures
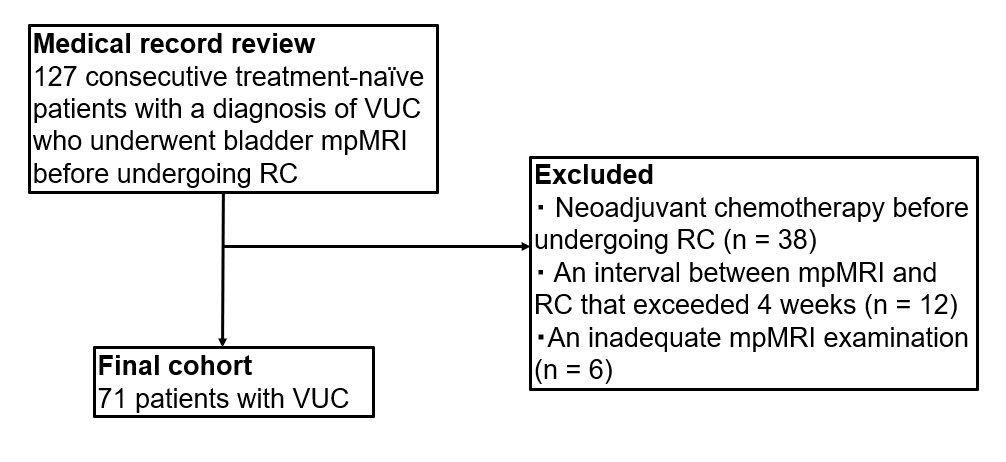
Figure 1. Flowchart of patient selection.
VUC, urothelial carcinoma with variant histology; mpMRI, multiparametric MRI; RC, radical cystectomy.
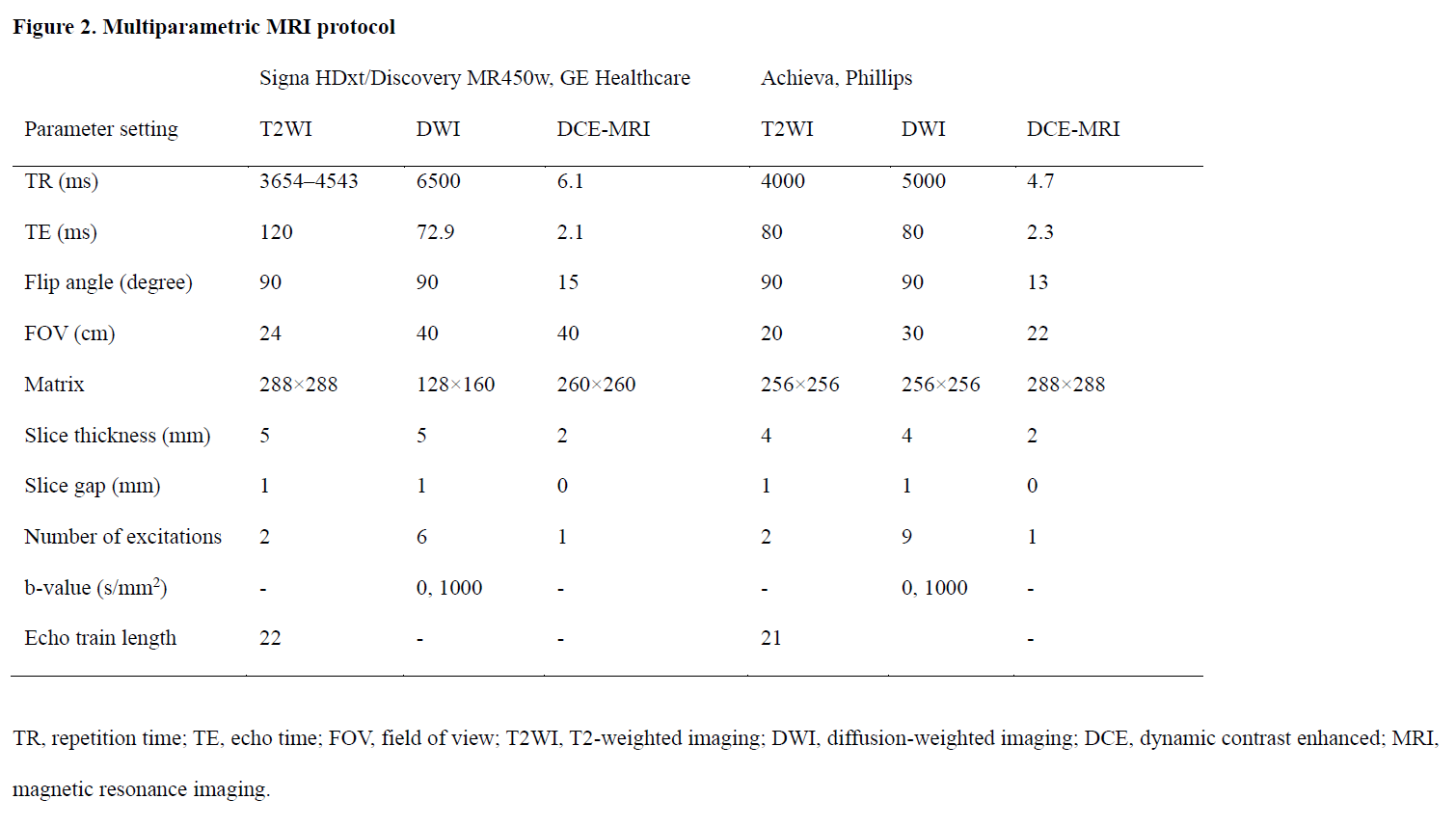
Figure 2. Multiparametric MRI protocol
TR, repetition time; TE, echo time; FOV, field of view; T2WI, T2-weighted imaging; DWI, diffusion-weighted imaging; DCE, dynamic contrast-enhanced; MRI, magnetic resonance imaging.
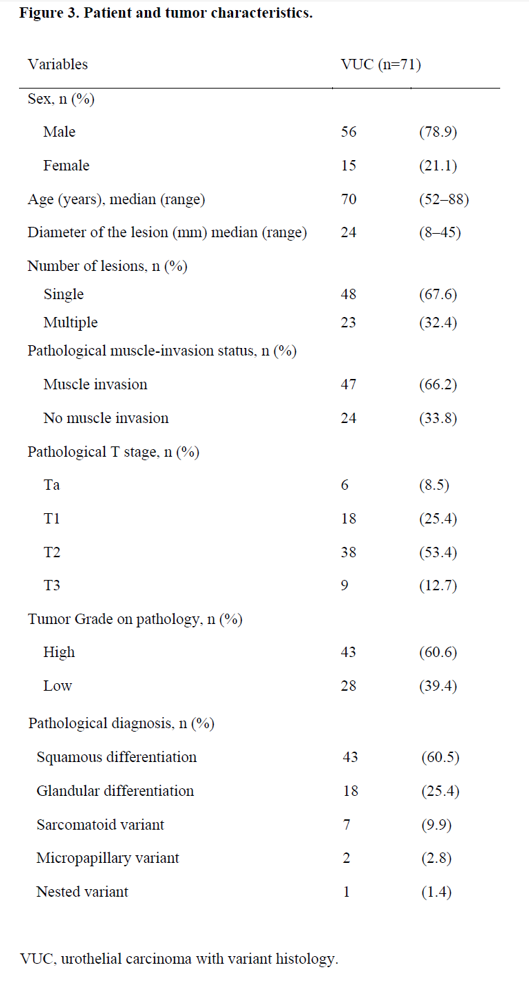
Figure 3. Patient and tumor characteristics
VUC, urothelial carcinoma with variant histology.
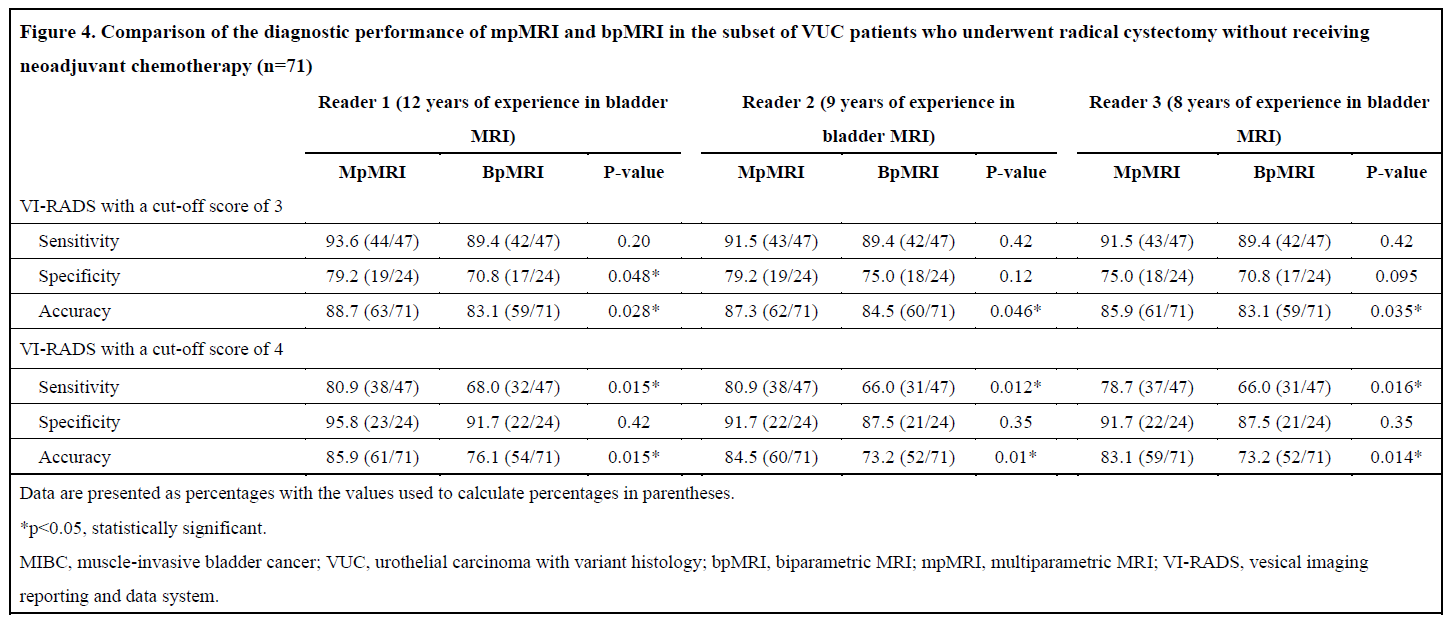
Figure 4. Comparison of the diagnostic performance of mpMRI and bpMRI in the subset of VUC patients who underwent radical cystectomy without receiving neoadjuvant chemotherapy (n=71)
Data are presented as percentages, with the values used to calculate rates in parentheses. *p<0.05, statistically significant.
MIBC, muscle-invasive bladder cancer; VUC, urothelial carcinoma with variant histology; bpMRI, biparametric MRI; mpMRI, multiparametric MRI; VI-RADS, vesical imaging reporting and data system.
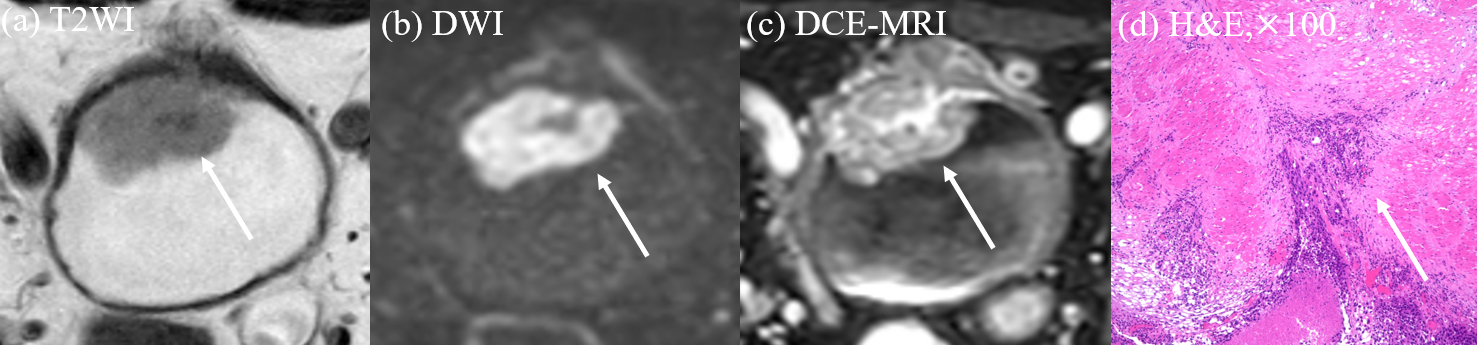
Figure 5. A 68-year-old man, MIBC with squamous differentiation
(a) Lobular tumor with an intermediate SI infiltrating into the muscularis propria. (b) Lobular tumor with a high SI with a low SI stalk. (c) Contrast-enhanced tumor with an infiltration into the muscularis propria. The corresponding scores for the three readers were 3/2/2 for bpMRI and 4/4/4 for mpMRI, respectively. (d) MIBC was determined by pathology.
MIBC, muscle-invasive bladder cancer; bpMRI, biparametric MRI; multiparametric MRI; SI, signal-intensity VI-RADS, Vesical Imaging-Reporting and Data System.