0782
Quantification of renal oxygenation with field-insensitive T2-preparation and fast acquisition1Department of Biomedical Engineering, Zhejiang University, Hangzhou, China, 2Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 3MR Collaboration, Siemens Healthineers Ltd., Shanghai, China
Synopsis
Keywords: Kidney, Kidney
Motivation: T2-based method was recently extended to measure renal oxygen metabolism. However, MLEV T2-preparation can be less robust due to field inhomogeneity in abdomen.
Goal(s): The goal is to propose a field-insensitive method for renal oxygenation quantification.
Approach: An adiabetic T2-preparation (BIR-n) method was proposed. Simulation and phantom studies was performed to demonstrate the field-insensitivity. In-vivo experiements were conducted to examine the test-retest reproducibility.
Results: A robust T2 quantification at different B0 and B1 offsets were demonstrated. In-vivo experiments showed a good test-retest reproducibility. Oxygenation was also found to be consistent between left and right renal veins, and showed significant correlation with blood flow.
Impact: The proposed method has the potential to provide accurate and stable estimation of renal oxygen extraction and metabolism in a number of renal diseases.
INTRODUCTION
Tissue hypoxia played an important role in many kidney diseases1. BOLD-MRI was used to assess renal oxygenation but can be affected by many confounding factors. One important line of MRI-based oxygenation method relies on the T2-modulation effect of venous oxygenation (Yv), which was explored extensively in brain imaging2-5 and recently applied to kidney6-8. However, the frequently-used MLEV T2-preparation can be less robust due to field inhomogeneity in abdomen9-11, leading to estimation error. Thus, the goal of present work is to develop a fast and field-insensitive method with adiabatic T2-preparation, dubbed as T2-Relaxation-Under-Field-Insensitive-preparation-and-Fast-Acquisition (TRU-FIFA), for renal oxygenation measurement.METHODS
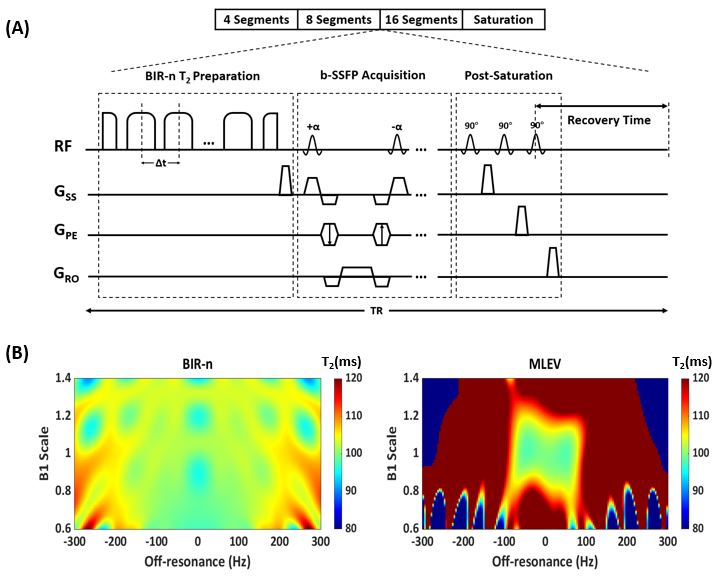
Pulse sequence and numerical simulationThe proposed sequence is illustrated in Figure 1A, composed of a B1-insensitive-rotation (BIR-n) T2-preparation, a bSSFP readout and a post-saturation. Here we designed an adiabatic T2-preparation consisting of a reverse adiabatic half passage (rAHP) segment, a series of fast passage (AFP) segments and an AHP segment. Duration between the middle of two AFP pulses were defined as Δt and kept constant. Thus, the number of AFP pulses determined the effective echo time (eTE). Monoexponential fitting of signals from different eTEs yields blood T2 which can be converted to oxygenation with a calibrated curve. In addition, bSSFP was known to be more suitable for abdominal imaging due to its high SNR efficiency, in-plane resolution and blood-tissue contrast12, thus was used in current sequence for readout. Numerical simulation was performed to compare the performance of BIR-n and MLEV (with composite refocusing) T2-preparation under different B0 and B1 offset.
Phantom experiment
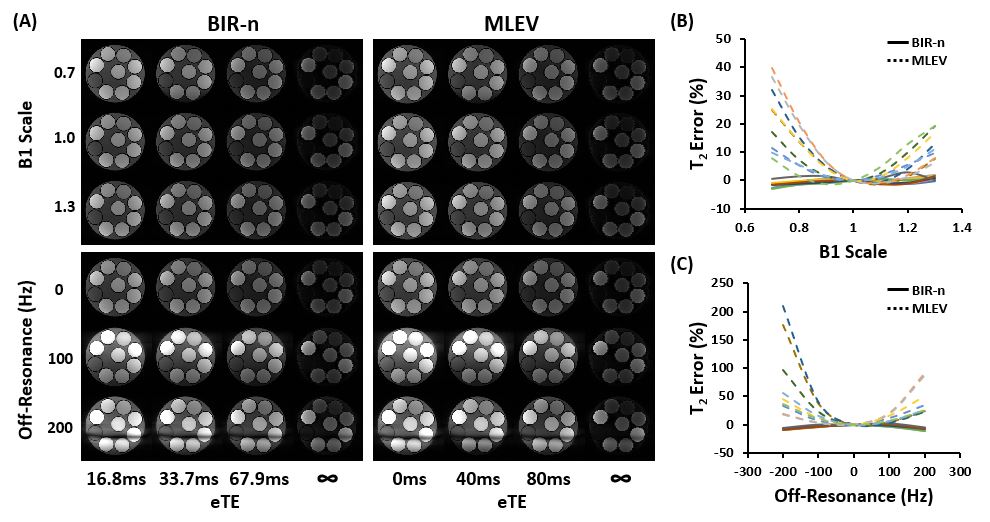
Sequences with BIR-n or MLEV T2-preparation were performed on a gel phantom containing nine tubes with different T2 values. For BIR-n sequence, T2-preparation with 1, 3 and 7 AFP segments were used with Δt=10ms, resulting in an eTE of 16.8, 33.7 and 67.9ms. For MLEV sequence, eTE of 0, 40, 80ms was used. In addition, the scan was performed with a saturation module before bSSFP readout representing an infinite eTE, which is used in the T2 fitting as describe previously13. The effect of B0 off-resonance on T2 quantification was tested by changing the transmitter frequency from -200Hz to 200Hz, and B1 sensitivity was tested by changing transmitter power from 0.7 to 1.3.
In-vivo experiment
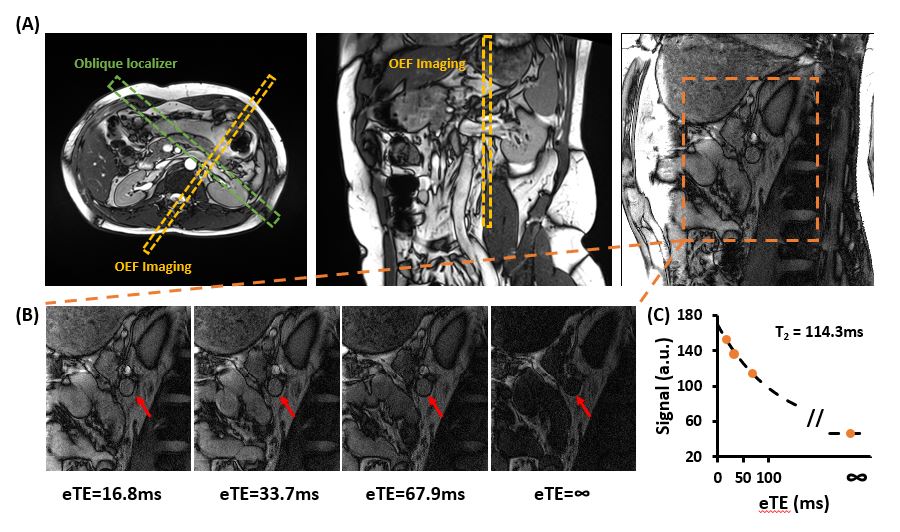
In-vivo position of TRU-FIFA sequence was shown in Figure 3A, where a double-oblique single-slice was placed to be perpendicular to the renal vein. Breath-holding was used with a scan duration of 18s. BIR-n and MLEV modules were compared in ten healthy volunteers (23.0±1.9yrs, 5F/5M). BIR-n T2 was converted to MLEV T2 using an equation determined by simulation, to account for different T1 recovery during preparation, before further calibrating to Yv14. Test-retest reproducibility was examined in ten participants (23.1±2.0yrs, 5F/5M). Both left and right renal Yv were measured in a subset of six participants. Finally, phase-contrast MRI with cardiac gating was performed, and the relationship between blood flow and oxygenation was assessed.
RESULTS
Simulation showed that T2 obtained from BIR-n preparation was robust against different B0 and B1 offset, while MLEV preparation can give a big error in T2 estimation (Figure 1B).Representative phantom images with different B1 and B0 offsets were shown in Figure 2A. It was found that T2 error was much larger under MLEV preparation than BIR-n. The latter gave a stable T2 estimation even when the images showed strong artifact caused by B0 off-resonance (Figure 2B-C).
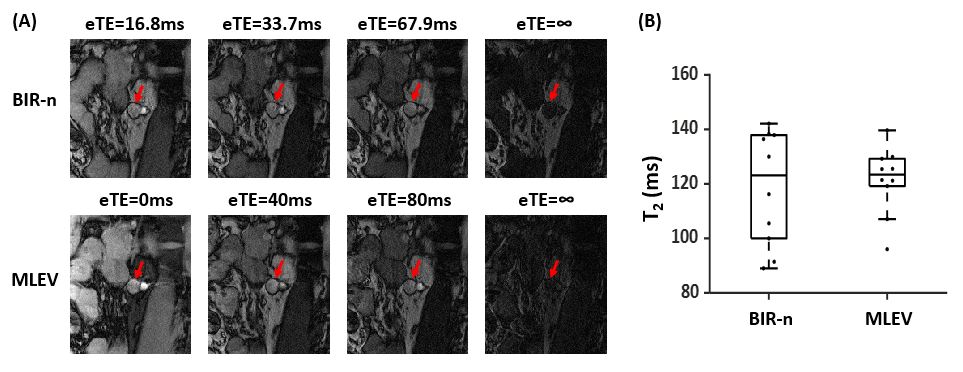
Figure 3B illustrated representative in-vivo images. Comparison of BIR-n and MLEV preparation showed no significant difference in T2 estimation (Figure 4).
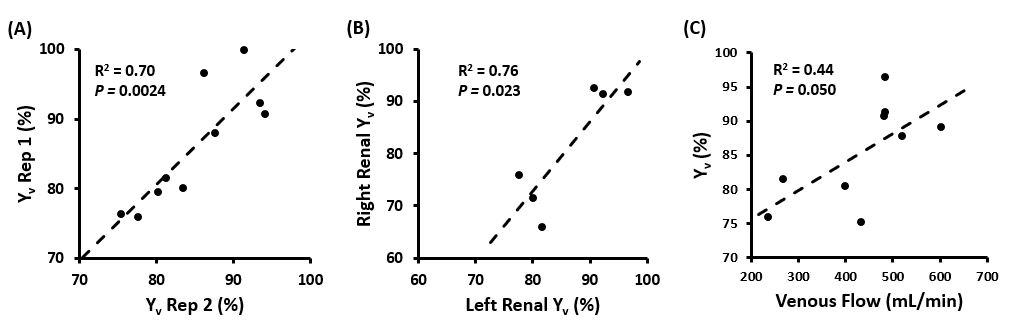
Significant correlation of Yv values from two repetitions was found (R2=0.70, P=0.0024, Figure 5A). A consistency between left and right renal Yv was also shown in healthy volunteers (R2=0.76, P=0.023, Figure 5B). Finally, we found that individuals with higher venous flow had a higher Yv (R2=0.44, P=0.050, Figure 5C).
DISCUSSION AND CONCLUSION
In this study, we proposed a B1/B0-insensitive T2-preparation module for more robust quantification of venous oxygenation in kidney and demonstrated it with both simulation and phantom experiments. MLEV can cause both under and over-estimation of T2 depending on specific combination of B0 and B1 offset, which may explain why in-vivo data showed no significant difference between two methods but a larger range of T2 from BIR-n.The consistency between left and right Yv suggested a similar oxygen consumption between two kidneys in healthy volunteers. The positive correlation between Yv and blood flow indicated a coupling between oxygen supply and extraction and is consistent with previous findings in the brain15, further demonstrating the validity of proposed technique.
Acknowledgements
No acknowledgement found.References
1. Pruijm M, Mendichovszky IA, Liss P, et al. Renal blood oxygenation level-dependent magnetic resonance imaging to measure renal tissue oxygenation: a statement paper and systematic review. Nephrol Dial Transplant 2018; 33: ii22-ii28. 2018/08/24. DOI: 10.1093/ndt/gfy243.
2. Lu H and Ge Y. Quantitative evaluation of oxygenation in venous vessels using T2-Relaxation-Under-Spin-Tagging MRI. Magn Reson Med 2008; 60: 357-363. 2008/07/31. DOI: 10.1002/mrm.21627.
3. Bolar DS, Rosen BR, Sorensen AG, et al. QUantitative Imaging of eXtraction of oxygen and TIssue consumption (QUIXOTIC) using venular-targeted velocity-selective spin labeling. Magnetic Resonance in Medicine 2011; 66: 1550-1562. DOI: https://doi.org/10.1002/mrm.22946.
4. De Vis JB, Petersen ET, Alderliesten T, et al. Non-invasive MRI measurements of venous oxygenation, oxygen extraction fraction and oxygen consumption in neonates. NeuroImage 2014; 95: 185-192. DOI: https://doi.org/10.1016/j.neuroimage.2014.03.060.
5. Guo J and Wong EC. Venous oxygenation mapping using velocity-selective excitation and arterial nulling. Magn Reson Med 2012; 68: 1458-1471. 2012/02/02. DOI: 10.1002/mrm.24145.
6. Daniel A, Cox E, Buchanan C, et al. Applying T2 Relaxation Under Spin Tagging (TRUST) to assess renal oxygenation in the kidney. In: Joint Annual Meeting ISMRM-ESMRMB; Abstract #1262 2018.
7. Deshpande RS, Langham MC, Cheng CC, et al. Quantification of bilateral kidney oxygen consumption with MOTIVE-bSSFP. In: ISMRM & ISMRT Annual Meeting & Exhibition; Abstract #4014 2023.
8. Deshpande RS, Langham MC and Wehrli FW. Quantification of bilateral whole-organ renal metabolic rate of O2 by exploiting conservation of flow and mass principle: a preliminary study. In: Joint Annual Meeting ISMRM-ESMRMB; Abstract #4011 2022.
9. Jenista ER, Rehwald WG, Chen EL, et al. Motion and flow insensitive adiabatic T2 -preparation module for cardiac MR imaging at 3 Tesla. Magn Reson Med 2013; 70: 1360-1368. 2012/12/06. DOI: 10.1002/mrm.24564.
10. Nezafat R, Ouwerkerk R, Derbyshire AJ, et al. Spectrally selective B1-insensitive T2 magnetization preparation sequence. Magn Reson Med 2009; 61: 1326-1335. 2009/03/26. DOI: 10.1002/mrm.21742.
11. Nezafat R, Stuber M, Ouwerkerk R, et al. B1-insensitive T2 preparation for improved coronary magnetic resonance angiography at 3 T. Magn Reson Med 2006; 55: 858-864. 2006/03/16. DOI: 10.1002/mrm.20835.
12. Rodríguez-Soto AE, Abdulmalik O, Langham MC, et al. T(2) -prepared balanced steady-state free precession (bSSFP) for quantifying whole-blood oxygen saturation at 1.5T. Magn Reson Med 2018; 79: 1893-1900. 2017/07/19. DOI: 10.1002/mrm.26835.
13. Akçakaya M, Basha TA, Weingärtner S, et al. Improved quantitative myocardial T(2) mapping: Impact of the fitting model. Magn Reson Med 2015; 74: 93-105. 2014/08/12. DOI: 10.1002/mrm.25377.
14. Lu H, Xu F, Grgac K, et al. Calibration and validation of TRUST MRI for the estimation of cerebral blood oxygenation. Magn Reson Med 2012; 67: 42-49. 2011/05/19. DOI: 10.1002/mrm.22970.
15. Peng SL, Dumas JA, Park DC, et al. Age-related increase of resting metabolic rate in the human brain. Neuroimage 2014; 98: 176-183. 2014/05/13. DOI: 10.1016/j.neuroimage.2014.04.078.
Figures