0779
The Application of FunctIonal Renal MRI to improve assessment of Chronic Kidney Disease (AFiRM) Study1Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham, United Kingdom, 2Centre for Cardiovascular Science, University of Edinburgh, Edinburgh, United Kingdom, 3Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 4Department of Infection, Immunity and Cardiovascular Disease, University of Sheffield, Sheffield, United Kingdom, 5Neuroradiological Academic Unit, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 6Dementia Research Centre, Queen Square Institute of Neurology, University College London, London, United Kingdom, 7Wellcome Centre for Human Neuroimaging, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 8Obesity Institute, Leeds Beckett University, Leeds, United Kingdom, 9Salford Royal NHS Foundation Trust, Salford, United Kingdom, 10Department of Radiology, Addenbrooke’s Hospital, Cambridge, United Kingdom, 11Centre for Kidney Research and Innovation, University of Nottingham, Nottingham, United Kingdom, 12Lead study site: University of Nottingham, Nottingham, United Kingdom
Synopsis
Keywords: Kidney, Kidney
Motivation: The need for better biomarkers to assess progression of Chronic Kidney Disease (CKD).
Goal(s): To determine if multiparametric MRI can detect changes in structure and function in CKD.
Approach: In the Application of Functional Renal MRI (AFiRM) study, multiparametric MRI is to be collected on 400 CKD participants at baseline and Year 2. The MRI protocol comprises T2- and T1-weighted scans, B0 and B1 mapping, T1, T2 and T2* relaxometry, DWI, MTR, PC-MRI and ASL perfusion.
Results: To date, 387 have been scanned, with preliminary MRI analyses on 300 datasets for B0 and B1, T1, T2*, MTR, and Total Kidney Volume (TKV).
Impact: Application of the UKRIN-MAPS multiparametric renal MRI protocol to study changes in renal structure and function in CKD progression. This will provide definitive evidence on the question of whether MRI is better at tracking disease progression than conventional biomarkers.
Introduction
The global burden of chronic kidney disease (CKD) is significant, affecting ~10% of the world’s population. CKD can progress to kidney failure, increases cardiovascular risk and costs the UK health system >£1.4billion annually. Better imaging methods to determine cause and prognosis of kidney diseases are required for improved patient stratification and targeting of current treatments, and to underpin new drug development to identify those most likely to respond to therapeutics.Renal multiparametric MRI provides whole kidney structural and functional measurements in a single scan session. This allows multiple aspects of the pathology that contribute to CKD progression to be assessed, including altered tissue microstructure (inflammation/fibrosis), oxygenation and perfusion.
The Application of Functional Renal MRI to improve assessment of chronic kidney disease (AFiRM) study1 is funded by the National Institute for Health and Care Research (NIHR). It is a UK-wide multi-centre study to determine if multiparametric renal MRI as developed in UKRIN-MAPS2, can provide structural and functional assessments of the kidneys to deliver prognostic information and ultimately help guide treatment decisions. This abstract describes the MRI study design and analysis pipeline, and current progress since recruitment commenced in June 2021.
Methods
AFiRM is a multi-centre, prospective cohort study of 400 participants with CKD from 10 UK centres. Renal multiparametric MRI3-8 is being collected at baseline and Year 2. Subjects are being scanned across GE, Philips and Siemens 3T MR scanners (1 GE site, 4 Philips sites, 5 Siemens sites) following quality assurance using the ISMRM/NIST phantom (Figure 1). The MRI protocol (Figure 2) comprises B0 and B1 mapping (for scanner characterization, correction of quantitative measures, and distortion correction), relaxometry measures of T1 (both MOLLI and inversion recovery spin echo EPI), T2 and T2* mapping, Diffusion Weighted Imaging (DWI, multiple b-values and directions for an IVIM fit and estimation of fractional anisotropy (FA)) angiograms and phase contrast MRI (PC-MRI) of the renal arteries, magnetization transfer ratio (MTR) mapping, volumetric T2- and T1-weighted scans for estimation of total kidney volume (TKV) and cortex and medulla volume, mDIXON, and ASL perfusion scans.The analysis pipeline (Figure 3) consists of machine learning based segmentation from the T2-weighted (for total kidney9) and T1-mapping (for cortex and medulla10) scans. B0, B1 and MTR maps are generated, BOLD R2*/T2*-mapping data is fit to an exponential model, T2-mapping data is fit to both a simple exponential model and a StimFit model11. Distortion correction is applied to SE-EPI-based data and model driven registration (MDR) is used to realign T1 (MOLLI and SE-EPI), ASL and DWI data and quantitative maps subsequently generated.
A mechanistic sub-study aims to compare MRI measures in 45 participants with renal biopsy findings. Tissue blocks will undergo quantitative analysis of fibrosis, capillary density and inflammation using immunohistochemistry techniques.
For all participants, annual clinical follow-up visits will collect eGFR, albuminuria and change in clinical status until Year 4. Long-term outcomes will be determined with individual patient tracking of kidney failure events via the UK Renal Registry at Year 5 and 10. Cause and effect between the renal MRI measures (alone and in combination) and the progression of CKD will be determined.
Results
As of October 2023, 627 potential participants have been screened of whom 466 have been recruited. Mean age is 55 years, 293 (63%) are male and 39 (6%) have had a renal biopsy within six months prior to recruitment. Distribution across CKD stages is: stage G1/2 16%; stage G3A 22%; stage 3B 34%; and stage G4 28%. The most common identified causes of CKD are IgA nephropathy (20%), CKD of unknown cause (16%) and diabetic kidney disease (15%), as shown in Figure 4. To date, 387 MRI scans have been completed, 379 baseline scans and 8 Year 2 visits (187 Philips, 178 Siemens, 22 GE datasets) Preliminary MRI analyses have been completed in 300 datasets for B0 and B1 mapping, T1 MOLLI and T2* mapping as well as estimation of TKV from T2-weighted scans3 as shown in Figure 5.Discussion
The AFiRM study is a UK-wide large-scale multicentre clinical study of renal multiparametric MRI in people with CKD, applying the UKRIN-MAPS harmonised renal MRI protocol, storage, and quality assurance and centralised analysis. Recruitment to AFiRM is scheduled to complete by December 2023, after which results of the full cohort baseline measures are expected.Conclusion
This study applies the UKRIN-MAPS multiparametric renal MRI protocol to understand changes in renal structure and function in CKD disease progression. This has the potential to transform the study of novel drugs for CKD progression, assessing changes earlier than traditional clinical measures.Acknowledgements
This work was funded by the UKRIN-MAPS MRC Partnership grant (MR/R02264X/1) and the NIHR AFiRM project (NIHR128494).References
1. Application of Functional Renal MRI to improve assessment of chronic kidney disease (AFiRM) study website: https://www.uhdb.nhs.uk/afirm-study/
2. UKRIN-MAPS (MRI Acquisition and Processing Standardisation) website: https://www.nottingham.ac.uk/research/groups/spmic/research/uk-renal-imaging-network/ukrin-maps.aspx
3. Mendichovszky, I.; Pullens, P.; Dekkers, I.; Nery, F.; Bane, O.; Pohlmann, A.; de Boer, A.; Ljimani, A.; Odudu, A.; Buchanan, C.; Sharma, K.; Laustsen, C.; Harteveld, A.; Golay, X.; Pedrosa, I.; Alsop, D.; Fain, S.; Caroli, A.; Prasad, P.; Francis, S.; Sigmund, E.; Fernández‐Seara, M.; Sourbron, S. Technical recommendations for clinical translation of renal MRI: a consensus project of the Cooperation in Science and Technology Action PARENCHIMA. Magn. Reson. Mater. Physics, Biol. Med. 2019, doi:10.1007/s10334-019-00784-w.
4. Bane, O.; Mendichovszky, I. A.; Milani, B.; Dekkers, I. A.; Deux, J.-F.; Eckerbom, P.; Grenier, N.; Hall, M. E.; Inoue, T.; Laustsen, C.; Lerman, L. O.; Liu, C.; Morrell, G.; Pedersen, M.; Pruijm, M.; Sadowski, E. A.; Seeliger, E.; Sharma, K.; Thoeny, H. C.; Vermathen, P.; Wang, Z. J.; Serafin, Z.; Zhang, J. L.; Francis, S. T.; Sourbron, S.; Pohlmann, A.; Fain, S. B.; Prasad, P. V. Consen-sus-based technical recommendations for clinical translation of renal BOLD MRI. Magn. Reson. Mater. Physics, Biol. Med. 2019, doi:10.1007/s10334-019-00802-x.
5. Dekkers, I. A.; Boer, A. de; Sharma, K.; Cox, E.; Lamb, H.; Buckley, D. L.; Bane, O.; Morris, D. M.; Prasad, P. V; Semple, S. I.; Gillis, K. A.; Hockings, P.; Buchanan, C.; Wolf, M.; Laustsen, C.; Leiner, T.; Haddock, B.; Hogenduin, J. M.; Pullens, P.; Sourbron, S.; Francis, S. Consensus-based technical recommendations for clinical translation of renal T1 and T2 mapping MRI. Magn. Reson. Mater. Physics, Biol. Med. 2019, doi:10.1007/s10334-019-00797-5.
6. Fabio Nery, PhD, Charlotte E. Buchanan, PhD, Anita A. Harteveld, PhD, Aghogho Odudu, PhD, Octavia Bane, PhD, Eleanor F. Cox, PhD, Katja Derlin, MD, H. Michael Gach, PhD, Xavier Golay, PhD, Marcel Gutberlet, PhD, Christoffer Laustsen, PhD, Al-exandra Ljiman, M. A. F. Consensus-based technical recommendations for clinical translation of renal ASL MRI. MAGMA 2020.
7. Ljimani, A.; Caroli, A.; Laustsen, C.; Francis, S.; Mendichovszky, I. A.; Bane, O.; Nery, F.; Sharma, K.; Pohlmann, A.; Dek-kers, I. A.; Vallee, J. P.; Derlin, K.; Notohamiprodjo, M.; Lim, R. P.; Palmucci, S.; Serai, S. D.; Periquito, J.; Wang, Z. J.; Froeling, M.; Thoeny, H. C.; Prasad, P.; Schneider, M.; Niendorf, T.; Pullens, P.; Sourbron, S.; Sigmund, E. E. Consensus-based technical recom-mendations for clinical translation of renal diffusion-weighted MRI. Magn. Reson. Mater. Physics, Biol. Med. 2019, doi:10.1007/s10334-019-00790-y.
8. Villa G, Ringgaard S, Hermann I, Noble R, Brambilla P, Khatir DS, Zöllner FG, Francis ST, Selby NM, Remuzzi A, Caroli A. Phase-contrast magnetic resonance imaging to assess renal perfusion: a systematic review and statement paper. MAGMA. 2020 Feb;33(1):3-21. doi: 10.1007/s10334-019-00772-0. Epub 2019 Aug 17. Erratum in: MAGMA. 2020 Oct;33(5):747. PMID: 31422518; PMCID: PMC7210220.
9. Daniel AJ, Buchanan CE, Allcock T, Scerri D, Cox EF, Prestwich BL, Francis ST. Automated renal segmentation in healthy and chronic kidney disease subjects using a convolutional neural network, Magn. Reson. Med. Volume86, Issue2, 1125-113, 2021.
10. Cox EC, Gong Z, Craig M, Mohammadi-Nejad A-R, Auer D, Sotiropoulos S, Chen X, Francis S. Automated Analysis of Kidney MRI data in the UK Biobank. 5th Renal MRI meeting Ghent, 2023.
11. Li H, Buchanan CE, Morris DM, Daniel AJ, Sousa J, Sourbron S, Thomas DL, Francis ST, Priest AN. Improved Harmonization of Renal T2 Mapping Between Vendors using Stimulated Echo Compensation. ISMRM 2022, 4409.
Figures
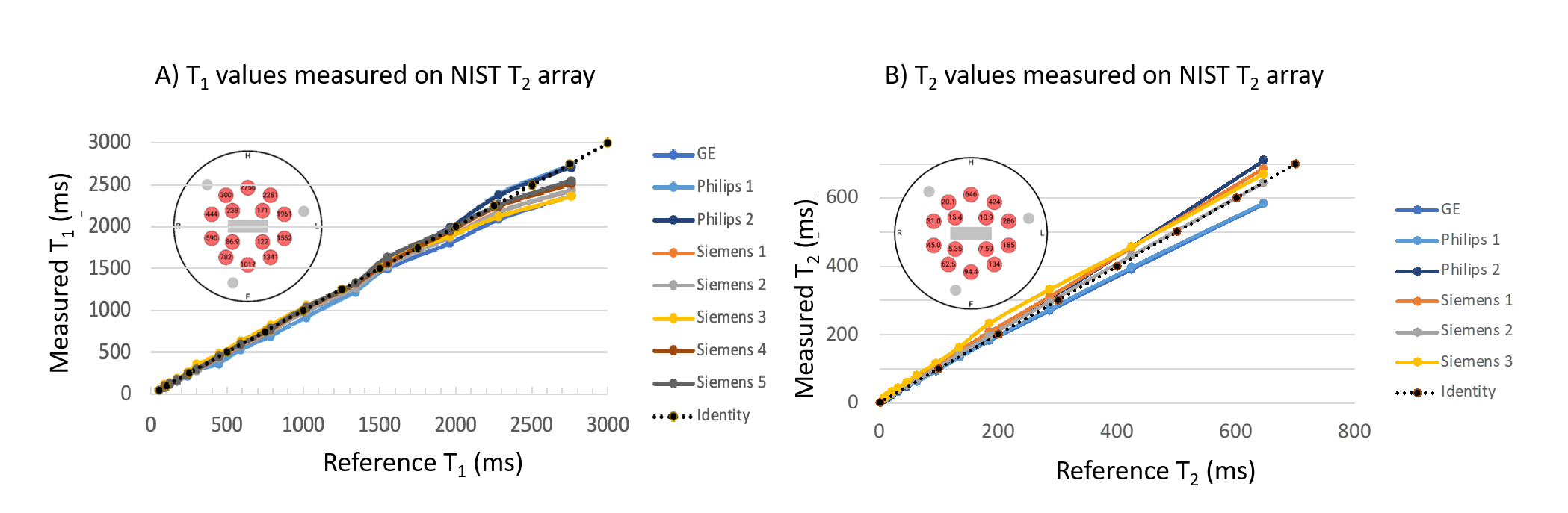
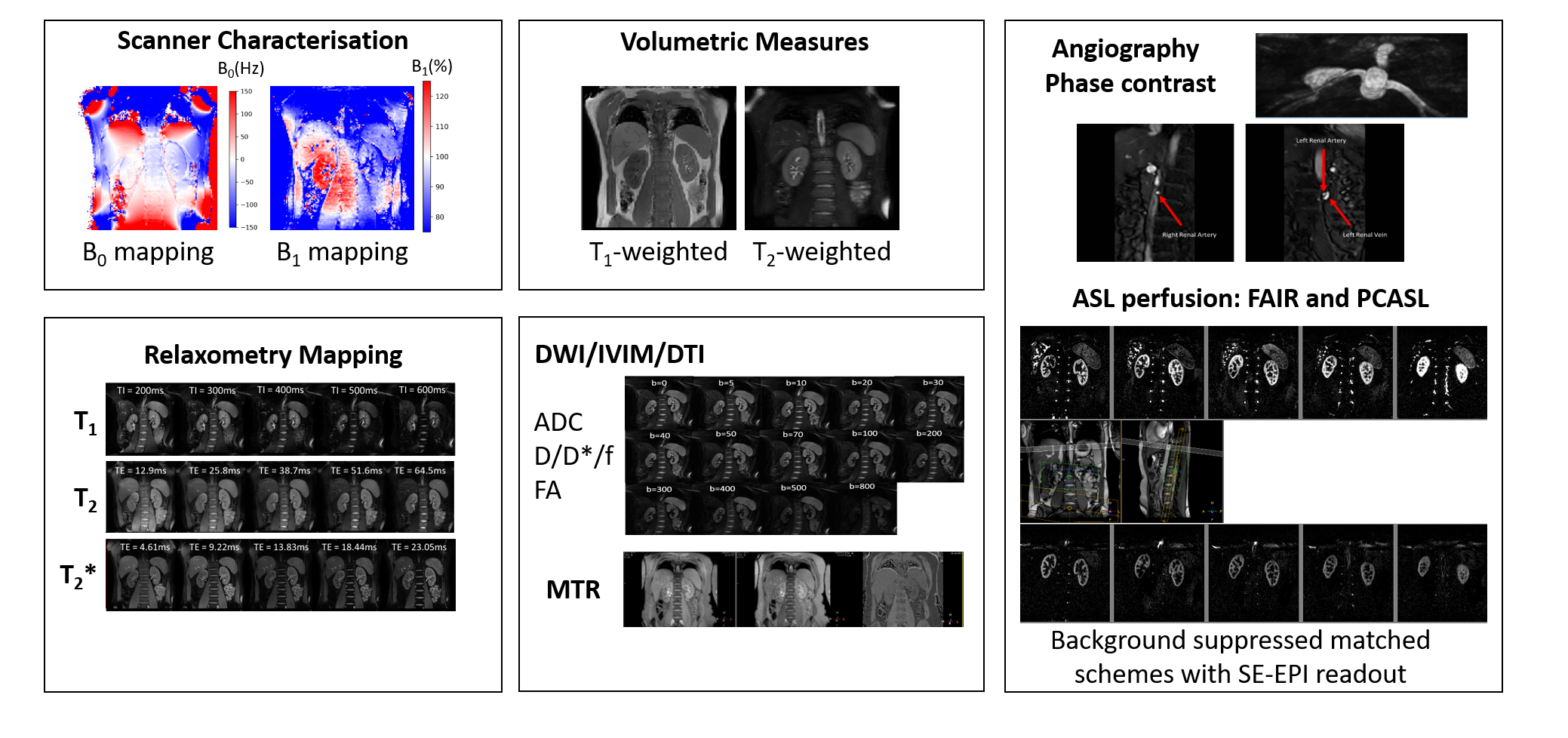
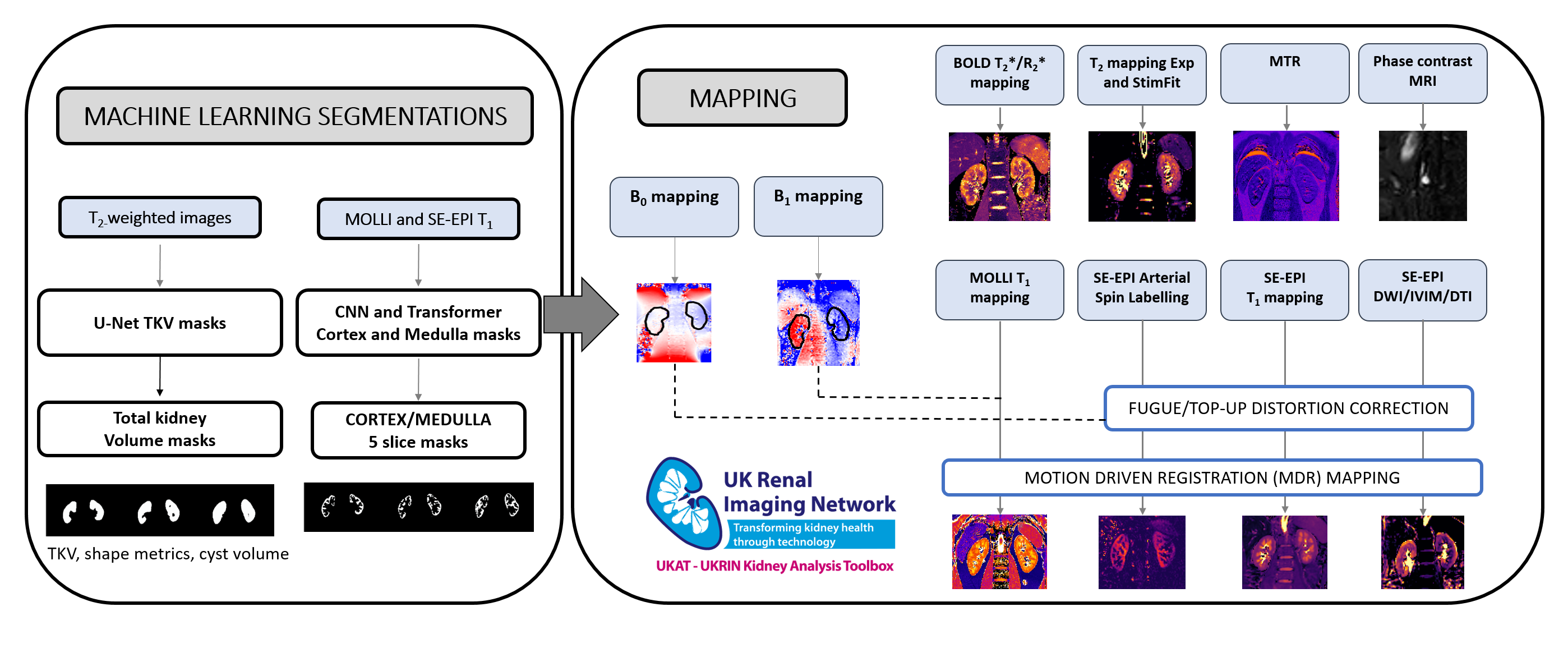
Figure 3: Analysis pipeline for multiparametric protocol showing machine learning U-net, and CNN and transformer to generate total kidney volume and cortex and medulla masks, and multiparametric mapping methods incorporating B0 and B1 corrections.
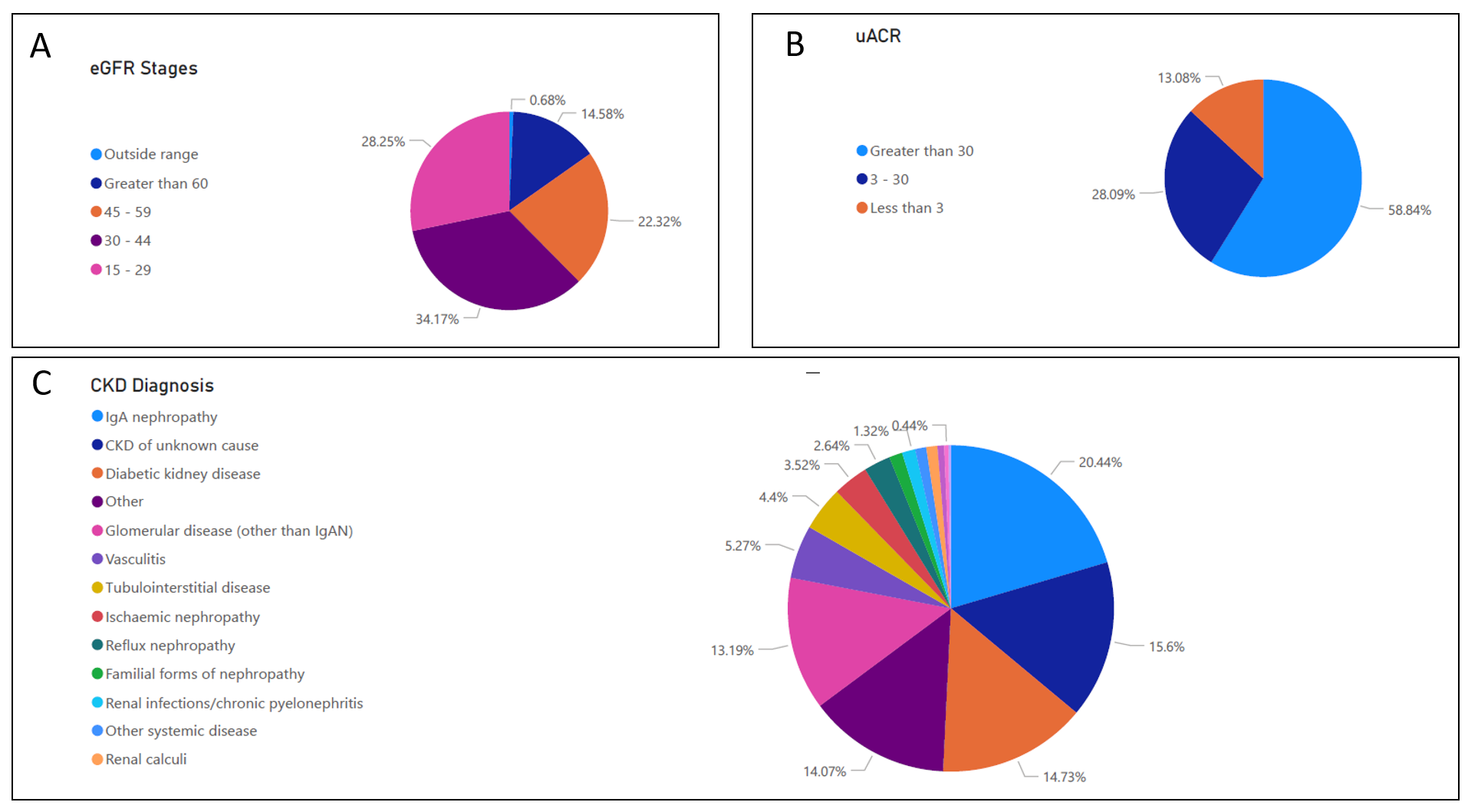
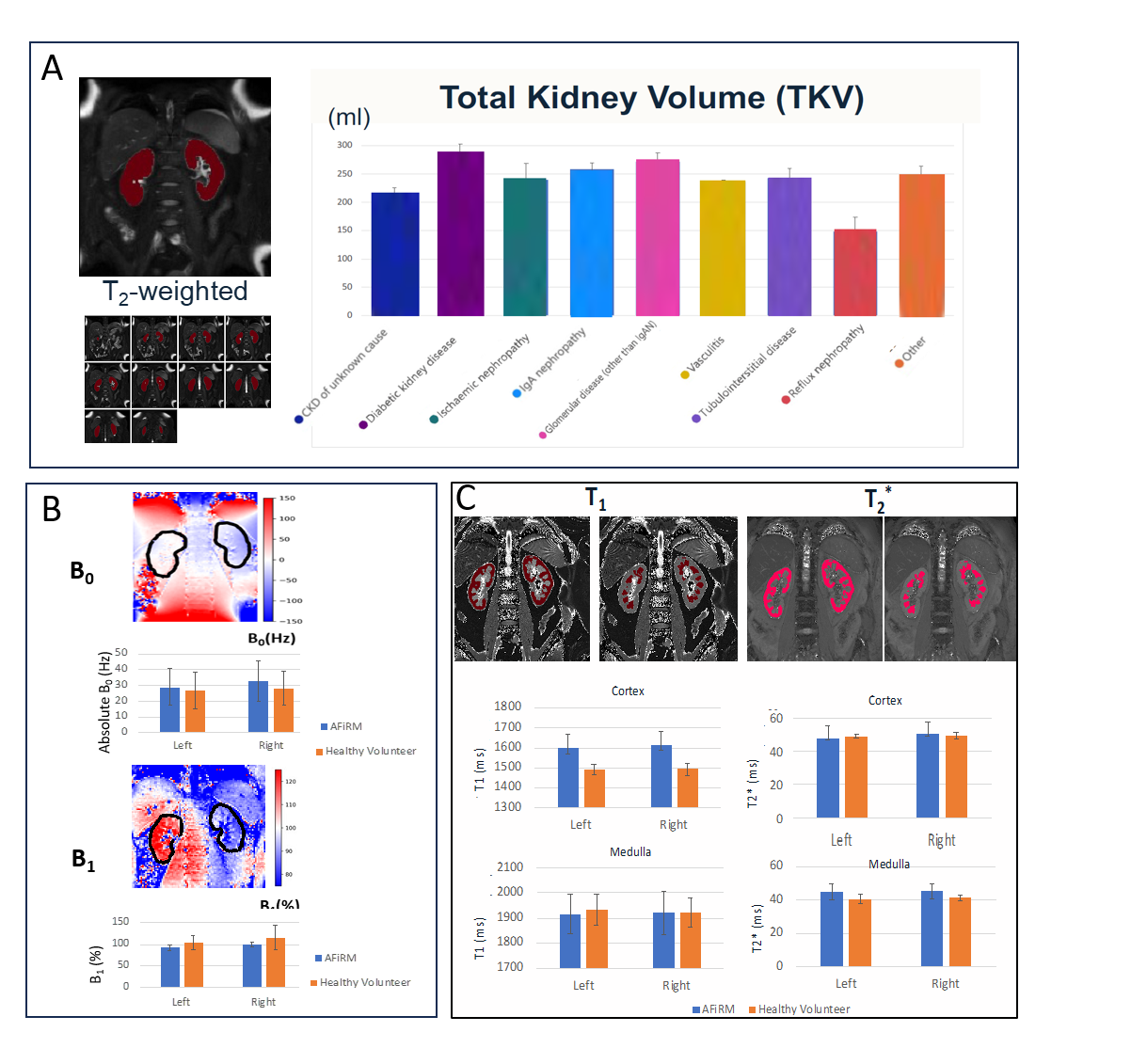
Figure 5: Results of preliminary MRI analyses of 300 datasets from the AFiRM study showing A) Example T2-weighted scan and U-net masks, and TKV values separated by CKD aetiology. B) Example B0 and B1 maps with absolute values within the TKV mask for Left and Right kidney in AFiRM patients and healthy volunteers, C) Example T1 MOLLI and T2* maps, CNN cortex and medulla masks, and associated T1 and T2* values in cortex and medulla in AFiRM patients and healthy volunteers. Healthy volunteer values are taken from UKRIN-MAPS travelling kidney data.