0768
Patella Shape is Associated with ACL Injury and Changes in KOOS and T1rho Following ACLR1The Cleveland Clinic Foundation, Cleveland, OH, United States, 2University of California, San Francisco, San Francisco, CA, United States, 3Hospital for Special Surgery, New York, NY, United States, 4Mayo Clinic, Rochester, MN, United States, 5Brigham and Women's Hospital, Boston, MA, United States
Synopsis
Keywords: Osteoarthritis, Bone, Patella, Shape, ACL, PTOA
Motivation: PTOA progression is poorly understood and there is a relative dearth of data available on the impact of the patellofemoral joint on PTOA.
Goal(s): The goal of this study was to elucidate the relationship between PTOA, knee function, and patella shape and to investigate possible indicators for PTOA progression.
Approach: A shape model of the patella was used to explore longitudinal shape changes and associations with injury, sex, KOOS, and cartilage T1rho in 67 patients following ALR and 11 controls.
Results: Ipsilateral patella shape was found to be associated with ACL injury, sex, and the degenerative changes accompanying PTOA.
Impact: This study suggests patella shape may play a role in ACL injury and PTOA. These results should inform future biomechanical studies of the knee joint which could lead to the development of preventative orthoses and novel interventions.
Introduction
Osteoarthritis (OA) is a heterogeneous disease characterized by progressive cartilage loss, subchondral bone remodeling, osteophyte formation, and synovial inflammation which can lead to joint pain and disability and affects an estimated 250 million people worldwide [1]. Osteoarthritic degeneration of the joint following an acute injury, such as an articular fracture, chondral injury, or ligament or meniscal tear is termed post-traumatic OA (PTOA) [2]. Despite treatment, between 23-50% of individuals who suffer a knee joint trauma eventually develop PTOA and the factors which may indicate PTOA progression are not well understood [3]. Previous studies have explored shape changes in the tibiofemoral joint following ACL reconstruction (ACLR), which may serve as an indicator of PTOA progression; however, there is relatively little reporting of similar data for the patellofemoral joint [4, 5]. The purpose of this study was to investigate patella bone shape as an early indicator for PTOA using longitudinal changes and associations with injury, sex, KOOS, and cartilage T1rho values.Methods
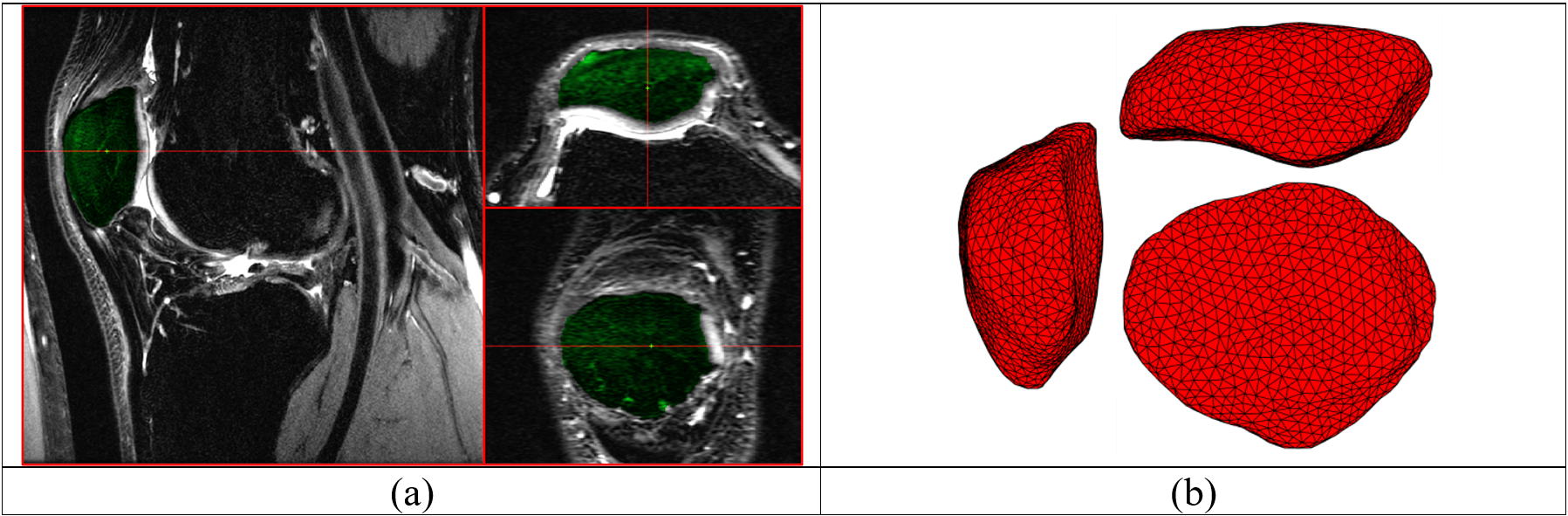
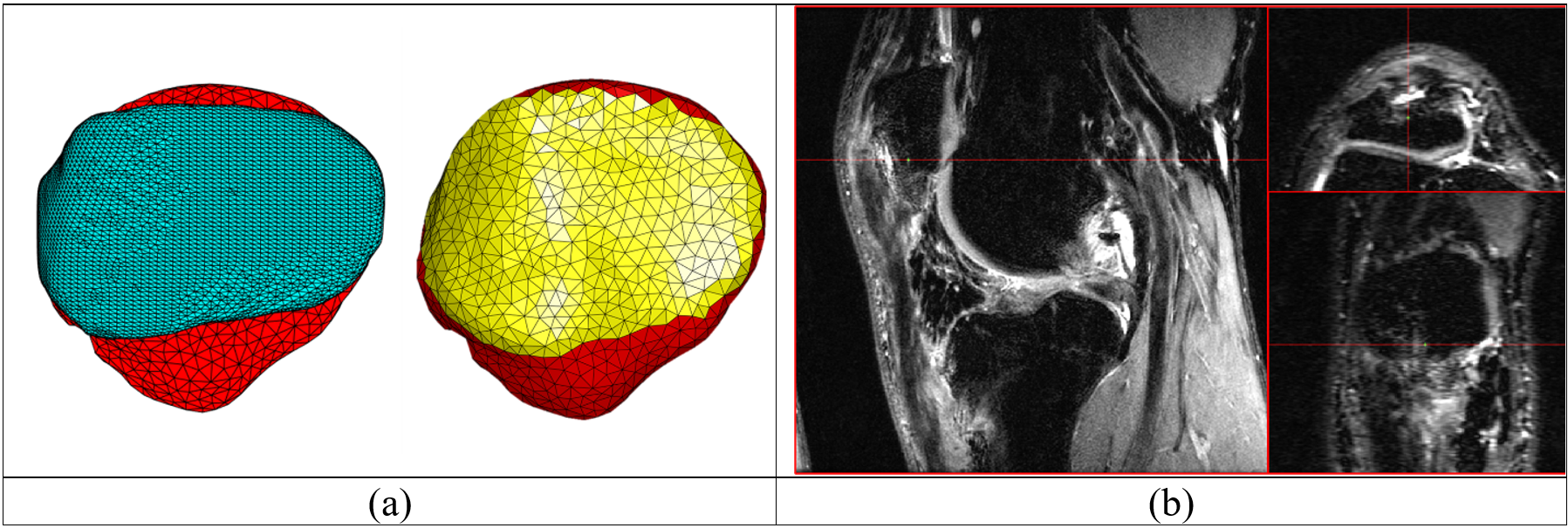
Bilateral knee MRIs from 67 patients (38 males, age: 29.2 ± 8.4 years, BMI: 24.6 ± 2.4 kg/m2, 29 females, age: 25.5 ± 10.3 years, BMI: 23.3 ± 3 kg/m2) who suffered a single complete ACL injury and 11 controls (5 males, age: 31.3 ± 4.5 years, BMI: 24.9 ± 0.9 kg/m2, 6 females, age: 33.4 ± 5.6 years, BMI: 23.9 ± 3.7 kg/m2) were collected as part of an IRB-approved multisite study using 3-T fat saturated CUBE sequences (GE Healthcare, Milwaukee, WI, USA). Patient MRIs were acquired prior to ACLR (baseline) and 6 months and 12 months following ACLR while control MRIs were collected twice, 12 months apart. In addition, KOOS and patella cartilage T1rho relaxation times were obtained for all subjects. A two-stage deep learning process (global and local 2D U-Net models) was used to automatically segment the patellae of each subject at each time point (Figure 1a) [6]. The automated segmentations of all 446 patellae were manually inspected and corrected as needed and then used to generate smoothed 3D surface reconstructions (Figure 1b) [7, 8]. Next, a minimum deformation template was deformably registered to each patella surface and the subchondral region of the bone was isolated by finding the area of overlap between the template and its patella cartilage segmentation (Figure 2a) [9]. The subchondral regions of the patellae were separated to account for substantial morphological alterations to the anterior and inferior surfaces caused by ACLR, particularly for bone-patella tendon-bone grafts (Figure 2b). Finally, a generalized Procrustes analysis produced size invariant point distributions from the registered surfaces and a statistical shape model of the subchondral region was created using a principal components analysis (PCA) [10]. The first 15 shape modes, which explained approximately 95% of the variance in the data, were retained for further analysis and their PC scores were calculated. Mixed effects models were used to investigate differences across ipsilateral, contralateral, and control patella shapes, sex differences, longitudinal shape changes, and associations with changes in KOOS and ipsilateral T1rho values from baseline to 12 months following ACLR [11]. To help control for the increase in false discovery rate due to the testing of multiple hypotheses, a significance cutoff of 0.01 was chosen for this study.Results
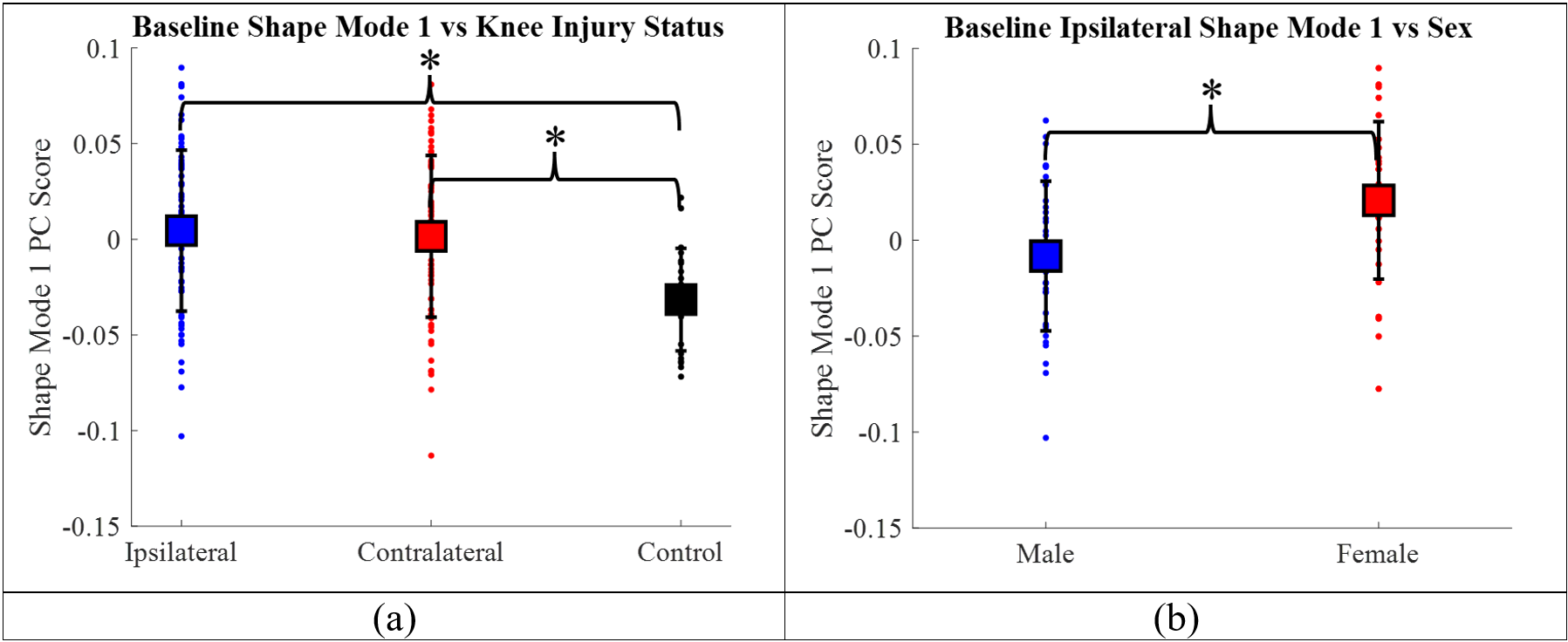
At baseline, significant (p < 0.01) differences between ipsilateral, contralateral and control patella shapes were found for mode 1 (Figure 3a), while significant (p < 0.01) sexual dimorphisms were observed for modes 1 (Figure 3b) and 5. No significant longitudinal changes were found for ipsilateral, contralateral, or control patella shapes. Changes in KOOS pain were found to be significantly (p < 0.01) associated with baseline, ipsilateral shape modes 5 and 6 while changes in ipsilateral T1rho were significantly (p < 0.01) associated with mode 13 (Table 1).Discussion
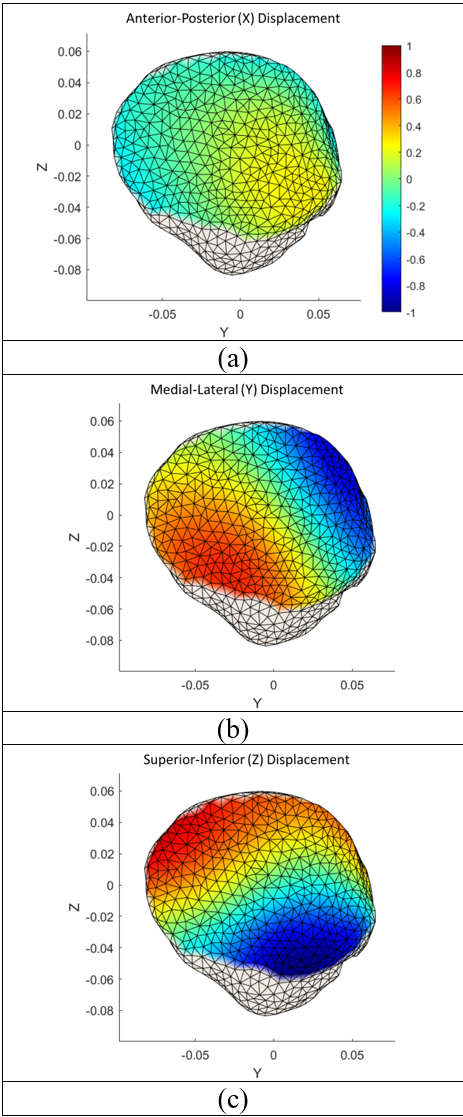
Shape mode 1, which accounted for approximately 24% of the total patella shape variation was found to be predictive of knee injury status (ipsilateral/contralateral vs. control) and sex. Figures 3 and 4 show that taller, narrower patellae with a protruding inferior vertical ridge are correlated with ACL injury and are more indicative of females. Shape modes 5 and 6 were associated with changes in KOOS pain while mode 13 was associated with changes in T1rho relaxation times. This suggests a potential link between patella shape and the degenerative changes accompanying PTOA.Conclusions
This study suggest that patella shape may contribute to ACL injury and to PTOA development after ACLR. Further studies will be needed to confirm these results and to determine the biomechanical connection between patella shape, ACL injury, and PTOA.Acknowledgements
This study was supported by the Arthritis Foundation and NIH/NIAMS R01AR075422References
1. Hunter DJ, Guermazi A, Roemer F, et al. Structural correlates of pain in joints with osteoarthritis. Osteoarthritis Cartilage. 2013 Sep;21(9):1170-8 2. Brown TD, Johnston RC, Saltzman CL, et al. Posttraumatic osteoarthritis: a first estimate of incidence, prevalence, and burden of disease. J Orthop Trauma. 2006 Nov-Dec;20(10):739-44 3. Khella CM, Asgarian R, Horvath JM, et al. An Evidence-Based Systematic Review of Human Knee Post-Traumatic Osteoarthritis (PTOA): Timeline of Clinical Presentation and Disease Markers, Comparison of Knee Joint PTOA Models and Early Disease Implications. Int J Mol Sci. 2021 Feb 17;22(4):1996 4. Pedoia V, Lansdown DA, Zaid M, et al. Three-dimensional MRI-based statistical shape model and application to a cohort of knees with acute ACL injury. Osteoarthritis Cartilage. 2015 Oct;23(10):1695-703 5. Zhong Q, Pedoia V, Tanaka M, et al. 3D bone-shape changes and their correlations with cartilage T1ρ and T2 relaxation times and patient-reported outcomes over 3-years after ACL reconstruction. Osteoarthritis Cartilage. 2019 Jun;27(6):915-921 6. Ronneberger O, Fischer P, Brox T. U-Net: Convolutional Networks for Biomedical Image Segmentation. MICCAI 2015. Lecture Notes in Computer Science. 2015 Nov; 9351 7. Lorensen WE, Cline HE. Marching cubes: A high resolution 3D surface construction algorithm. ACM SIGGRAPH Computer Graphics. 1987 Jul;21(4):163-169 8. Vollmer J, Mencl R, Muller H. Improved Laplacian Smoothing of Noisy Surface Meshes. Computer Graphics forum. 1999 Sep;18(3):131-138 9. Myronenko A, Song X. Point set registration: coherent point drift. IEEE Trans Pattern Anal Mach Intell. 2010 Dec;32(12):2262-75 10. Rohlf JF, Slice D. Extensions of the Procrustes Method for the Optimal Superimposition of Landmarks. Syst Zoo. 1990 Mar;39(1):40-59 11. Hardin JW, Hilbe JM (2018). Generalized Linear Models and Extensions (4th ed.). Stata PressFigures