0767
Comprehensive evaluation of wrist kinematics using 3D real-time MRI1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Department of Radiology, University of California Davis, Davis, CA, United States
Synopsis
Keywords: Functional/Dynamic, MSK, wrist, low-field, real-time
Motivation: A thorough understanding of wrist kinematics and kinetics is essential for diagnosing and treating wrist pain and instability. Current MRI methods are limited to tracking just a few thick slices and therefore use hand supports to restrict motion to pre-selected, simplified orientations.
Goal(s): To develop a 3D real-time MRI method at 0.55T for comprehensive evaluation of wrist kinematics.
Approach: A bSSFP 3D stack-of-spiral sequence with long spiral readout was implemented for evaluating wrist kinematics during maneuvers.
Results: Comprehensive 3D coverage at 10 frames/second was achieved without any restriction on wrist motion, providing measurements of ligament intervals in 3D and during active wrist motion.
Impact: The proposed 3D real-time method can potentially improve diagnosis of wrist injury and dysfunction and treatment planning, by providing a unique 3D evaluation of wrist kinematics and kinetics during the performance of clinically-important maneuvers involved in activities of daily living.
Introduction
There is currently an incomplete understanding of wrist kinematics and kinetics when performing routine tasks as part of activities of daily living. Therefore, wrist instability, resulting from trauma or injury, is difficult to diagnose and treat. Dynamic MRI (1-4) or CT (5) have been employed for these assessments, with MRI being the preferred modality as it is part of routine clinical care. However, current dynamic MRI methods are limited to 2D (1,3) or 3D (2) acquisitions with limited spatial coverage. To address this, the hand and arm are restrained to move in only a few pre-determined planes (2, 3), significantly reducing degrees of freedom. This arrangement makes it challenging to resolve and understand off-plane motion of wrist tissues during clinically-relevant maneuvers such as dart-throw (DT) and wrist flexion-extension (FE) (6).The new generation of mid-field MRI scanners (0.1-1.0T) (7,8) have substantially reduced B0 inhomogeneity and specific absorption rate (SAR), enabling the use of spiral balanced steady-state free precession (bSSFP) sequences with longer readouts and greater flexibility in the flip angle selection, while avoiding banding artifacts and exceeding SAR limitation. These advancements have the potential to greatly enhance the capabilities of real-time MRI, by providing more spatial coverage at a higher temporal resolution.
In this study, we implemented a real-time 3D bSSFP pulse sequence that combines a non-selective hard-pulse and a stack-of-spiral readout. This pulse sequence achieves exceptional scan efficiency for wrist imaging, allowing us to capture 3D real-time wrist movements at a frame rate of 10 frames/second. This approach permits a wide range of wrist maneuvers, including radial-ulnar deviation (RUD), DT, and FE, all without the need to restrict hand movement during the imaging process.
Methods
Pulse sequenceFigure 1 illustrates the 3D golden-angle stack-of-spiral sampling pattern. By using a non-selective hard-pulse (TRF=0.7ms) and long spiral readout (Tread=6.48 ms), this pulse sequence has an acquisition duty cycle of 77% (Tread/TR), which is much larger than Cartesian or radial acquisitions (~30-40%).
Data acquisition
Experiments were performed on a whole-body 0.55T system (prototype MAGNETOM Area, Siemens Healthineers, Erlangen Germany) with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate). RTHawk real-time interactive platform (Vista.ai, Palo Alto, California) was used to program the pulse sequence, perform online reconstruction for preliminary quality check, and acquire the data. One healthy adult male volunteer was scanned, under a protocol approved by our IRB.
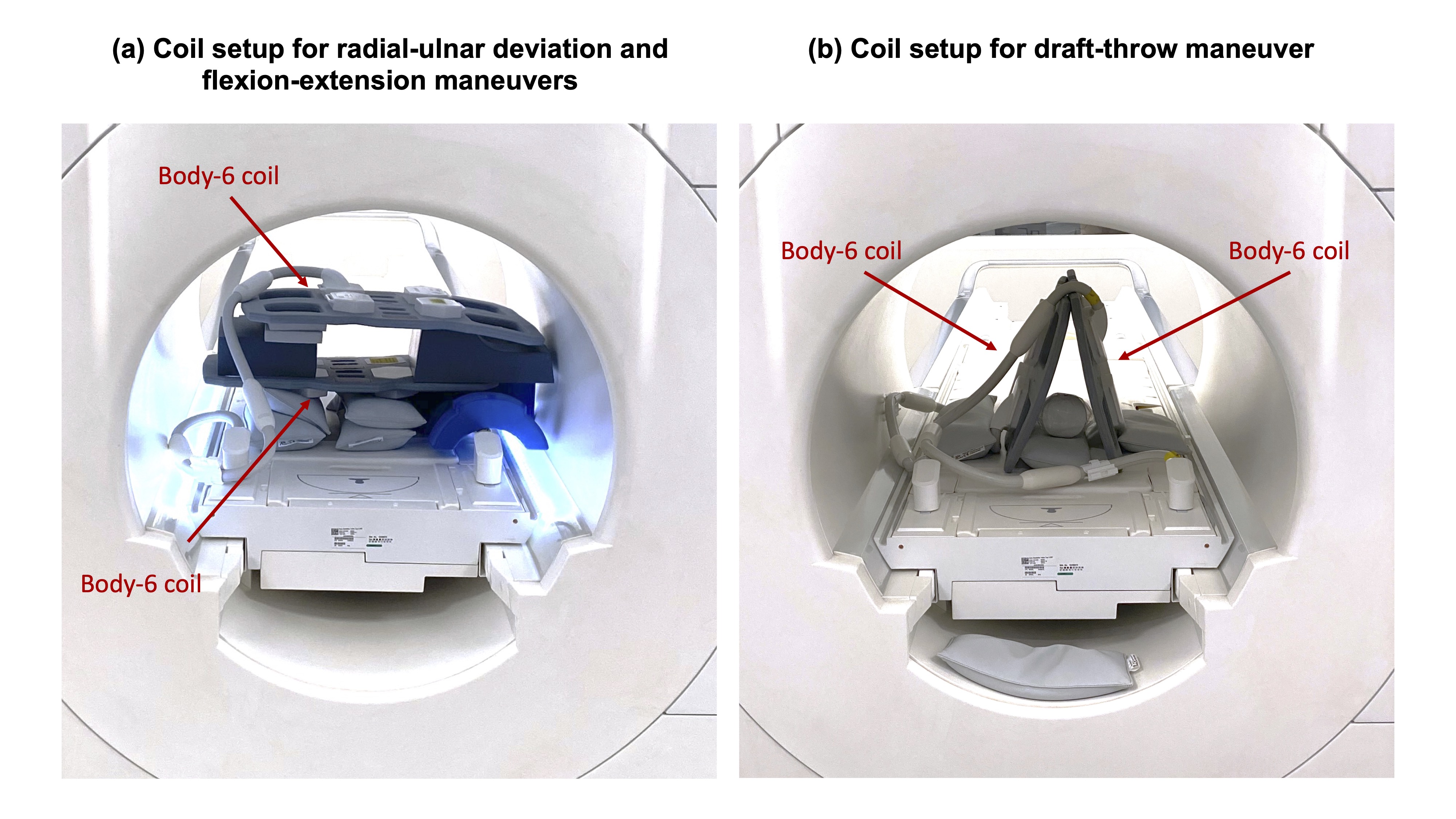
Two body-6 coils were used for data reception as illustrated in Figure 2. The volunteer was asked to kneel at the back of the scanner and extend his right arm to the scanner iso-center. Three different maneuvers were performed: RUD, FE, and DT, with each maneuver performed at a speed of 8-10 seconds per repetition for two repetitions. Scan parameters were TE/TR=0.46/8.42ms, Tread=6.48ms, flip angle=60o, FOV=22x22x8cm3, and voxel size=1.4x1.4x4mm3. Resonance frequency was tuned to imaging fat (-80Hz relative to water at 0.55T) to offer a positive contrast between bone marrow and ligament gaps. Real-time 3D images were reconstructed offline by spatiotemporally constrained reconstruction (STCR) (9), with the regularization parameters empirically chosen to balance the temporal blurring and residual aliasing.
Analysis
From images of the RUD and DT maneuvers, the scapholunate (SL) interval were measured in 3D. Similarly, the distance between the proximal and distal poles of the scaphoid along the volar cortex during the FE maneuver was determined.
Results
Figure 3 shows the central slices of real-time movies of RUD. Figure 4 shows 3D rendering of RUD. Figure 5 shows 3D rendering of DT. The SL interval assessment appeared to be more consistent across the range-of-motion with the DT maneuver (6.05mm versus 6.00mm at the extremas) compared to the RUD maneuver (3.25mm versus 4.37mm at the extremas). The distance between the scaphoid proximal and distal poles was 11.91mm.Discussion
This work presents a 3D real-time method to capture wrist movements at a frame rate of 10 frames/second. The use of non-selective excitation pulses and a relatively large imaging FOV ensured complete wrist coverage during the full range-of-motion, resolved in three-dimensions. With comprehensive wrist coverage, collected data can be visualized and evaluated in 4D (x,y,z,t), without restriction on maneuvers or range of motion. Intra-articular morphometrics can be assessed from the proposed method. The use of image registration or segmentation could potentially improve the 4D visualization further and may enable motion compensated reconstruction to further allow even higher spatial and temporal resolution. Further study will also evaluate the method in patients with dynamic wrist instability.Conclusion
Real-Time 3D imaging of the moving wrist is feasible at 0.55T, without movement restriction, and achieving 1.4x1.4x4mm3 spatial and 100ms temporal resolution.Acknowledgements
We acknowledge research support from Siemens Healthineers, and grant support from the National Institutes of Health (R21 HL159533 and U01 HL167613) and National Science Foundation (Award 1828736).References
1. Chaudhari AJ, Lim Y, Cui SX, Bayne CO, Szabo RM, Boutin RD, Nayak KS. Real-Time MRI of the Moving Wrist at 0.55 Tesla. British Journal of Radiology; 2023 Nov;96(1151):20230298.
2. Shaw CB, Foster BH, Borgese M, Boutin RD, Bateni C, Boonsri P, et al. Real-time three-dimensional MRI for the assessment of dynamic carpal instability. PLoS One. 2019;14(9):e0222704.
3. Boutin RD, Buonocore MH, Immerman I, Ashwell Z, Sonico GJ, Szabo RM, et al. Real-time magnetic resonance imaging (MRI) during active wrist motion--initial observations. PLoS One. 2013;8(12):e84004.
4. Wilms LM, Radke KL, Abrar DB, Frahm J, Voit D, Thelen S, et al. Dynamic assessment of scapholunate ligament status by real-time magnetic resonance imaging: an exploratory clinical study. Skeletal Radiol. 2023.
5. Leng S, Zhao K, Qu M, An KN, Berger R, McCollough CH. Dynamic CT technique for assessment of wrist joint instabilities. Med Phys. 2011;38 Suppl 1(Suppl 1):S50.
6. Moritomo H, Apergis EP, Herzberg G, Werner FW, Wolfe SW, Garcia-Elias M. 2007 IFSSH committee report of wrist biomechanics committee: biomechanics of the so-called dart-throwing motion of the wrist. J Hand Surg Am. 2007;32(9):1447-53.
7. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-93.
8. Guenthner C, Peereboom SM, Dillinger H, McGrath C, Albannay MM, Vishnevskiy V, et al. Ramping down a clinical 3 T scanner: a journey into MRI and MRS at 0.75 T. MAGMA. 2023.
9. Adluru G, McGann C, Speier P, Kholmovski EG, Shaaban A, Dibella EV. Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging. J Magn Reson Imaging. 2009;29(2):466-73.
Figures