0757
High resolution 3D isotropic non-rigid motion compensated T1 Dixon of Liver at a hybrid PET-MR scanner1Siemens Healthcare France, Courbevoie, France, 2INSERM U1148 Laboratory for vascular translational science, Paris, France, 3CHU de Nantes, Nantes, France, 4UMR_S 1307 Centre de Recherche en Cancérologie et Immunologie Intégrée Nantes Angers, Nantes, France, 5Hôpital Beaujon AP-HP, Clichy, France, 6INSERM U1149 Centre de Recherche sur l'Inflammation, Paris, France, 7School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 8MR Research Collaborations, Siemens Healthcare GmbH, Frimley, United Kingdom, 9Escuela de Ingeniería, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Motion Correction, Motion Correction, MRI, PET-MRI, liver, navigator, HCC, cancer, free-breathing MRI
Motivation: In current clinical practice, liver MRI scans often suffer from motion artifacts. This issue typically arises because patients struggle to maintain breath-holding.
Goal(s): Our goal is to produce a high-quality, isotropic 3D Dixon T1 scan without the need for breath-holding.
Approach: . Our method involves using a navigator to estimate liver motion, enabling us to calculate non-rigid motion fields for image reconstruction
Results: This approach yields high-quality free-breathing isotropic T1 3D Dixon liver data with a voxel size of 1.3mm³, surpassing the quality of the gold standard non-isotropic breath-hold Dixon T1 liver scan.
Impact: This work aims to deliver previously unseen high-quality free-breathing isotropic 3D Dixon liver data that can surpass the current clinical standard breath-hold non-isotropic T1 3D Dixon liver scans.
Introduction
Current clinical practice in liver magnetic resonance imaging (MRI) scans requires patients to hold their breath for approximately 15 to 20 seconds to acquire 3D T1 Dixon non-isotropic images. This breath-hold is necessary to maintain good image quality. However, breath-holding can be difficult for patients with underlying medical conditions, leading to image artifacts.The primary objective of this study is to evaluate a 3D non-rigid motion correction framework for T1 Dixon liver MRI imaging at a hybrid PET-MR scanner. We have accomplished this by adapting a 3D non-rigid motion correction framework recently developed for cardiac PET-MR [1]. Performance is evaluated using a novel PET-MR phantom setup that allows to induce realistic deformations within a silicon-molded block, as well as in a healthy volunteer. MRI only evaluation is performed at this stage, with the aim of extending this evaluation to the PET data in the near future.
Methods
Phantom Design
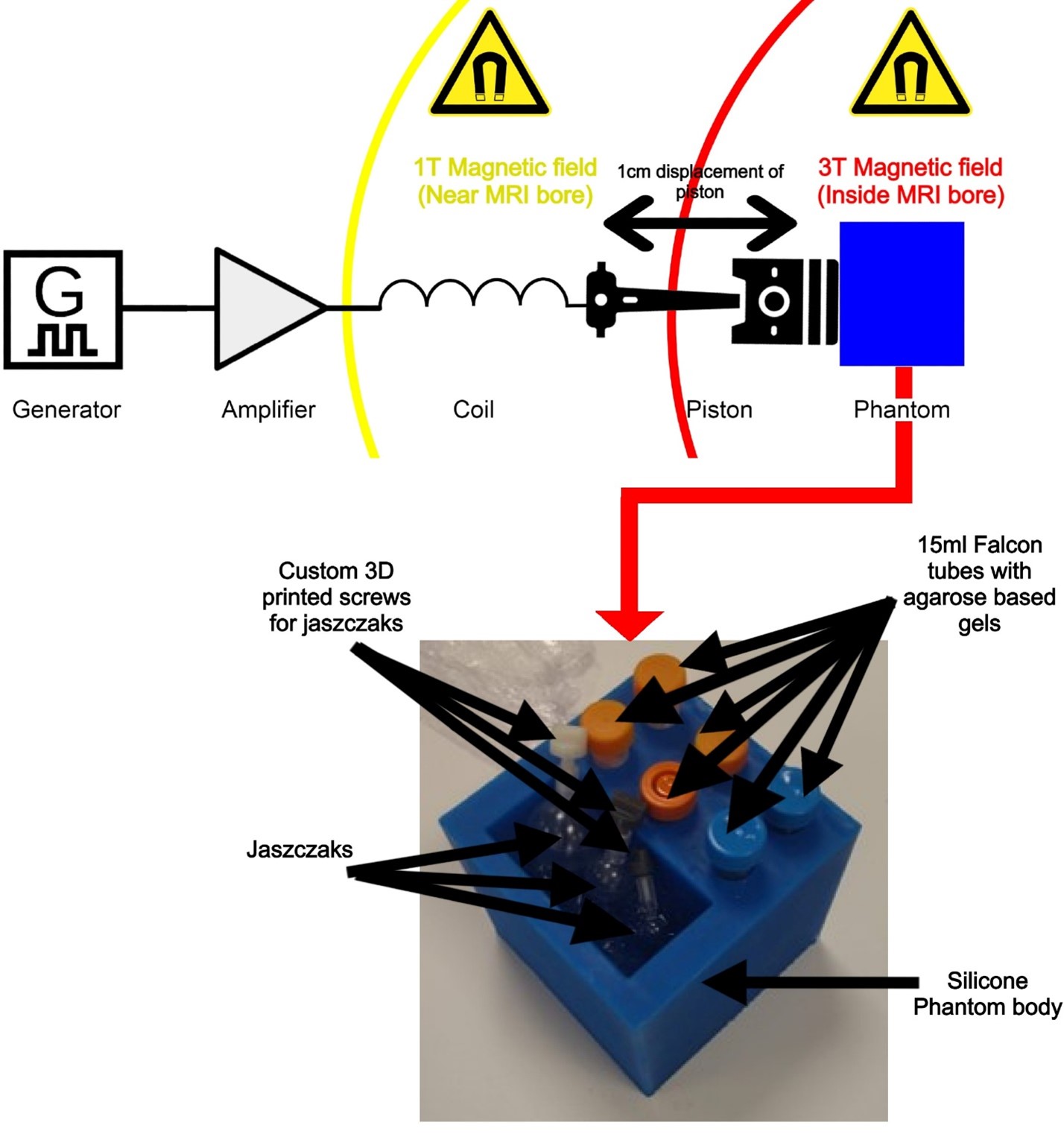
To evaluate a 3D motion-corrected T1 Dixon liver sequence, we created a unique phantom that mimics human physiology and breathing artifacts. The phantom uses a current-driven coil in the MRI’s magnetic field to induce realistic deformations in a silicon-molded block containing six 15ml Falcon tubes (Corning, USA). Four tubes contain agarose gels[2](UltraPure™ Agarose, Invitrogen Life Technologies, UK) doped with Nickel salt (Nickel(II) nitrate hexahydrate 98%, Thermoscientific, USA) to replicate liver tissue in T1 and T2, while two contain sucrose gels(Sigma Aldrich, UK) to simulate liver apparent diffusion coefficient values. An ultrasound gel compartment allows for object insertion (figure 1).
MR acquisition
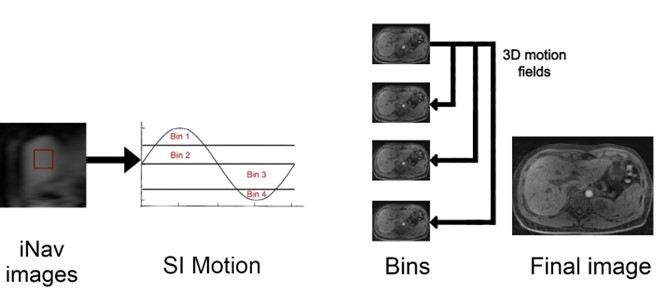
MR acquisition was performed on a 3T Biograph mMR (Software version V11P) PET-MR system (Siemens Healthcare, Erlangen Germany). Acquisition was performed with a free-breathing research framework with Dixon T1 encoding. The framework includes undersampled 3D Variable Density spiral-like Cartesian trajectory, 2D image navigator (iNAV) preceding the 3D acquisition to correct for food-head (FH) and right-left (RL) translation motion of the liver and to enable respiratory binning for subsequent non-rigid motion correction [3]. Acquisition parameters include Acquisition time: 2min20s, TR: 4.9ms, TE1: 1.34ms, TE2: 2.89ms, FA:9°, FOV:400mm, acquired voxel size: 1.3mm3, 3.3x undersampling factor, iNAV triggers every 250 milliseconds.
For comparison purposes, we acquired a clinical breath-hold VIBE Dixon T1. Acquisition parameters include acquisition time: 18s, TR: 4ms, TE1: 1.29ms, TE2: 2.52ms, FA: 15°, FOV: 400mm, interpolated voxel size: 1.2x1.2x3mm3, acquired voxel size: 1.6x1.2x6mm3, number of slices:72, Grappa:3.
Motion compensated reconstruction
2D FH and RL translation motion correction is performed in k-space with the motion estimated by the iNAVs. FH motion is used to bin the data in 4 respiratory bins. Each bin is reconstructed with iterative SENSE [4] and intra-bin image registration is performed to estimate the motion fields to end expiration [5]. Non-rigid motion compensated reconstruction is performed using iterative SENSE and the General Matrix Description (GMD) [6] of the non-rigid motion. Motion reconstruction is performed in-line in the scanner system.
Results
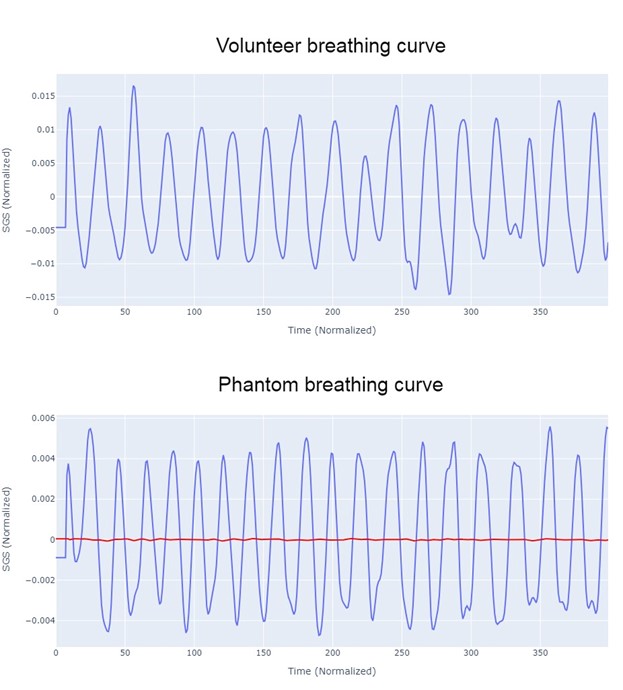
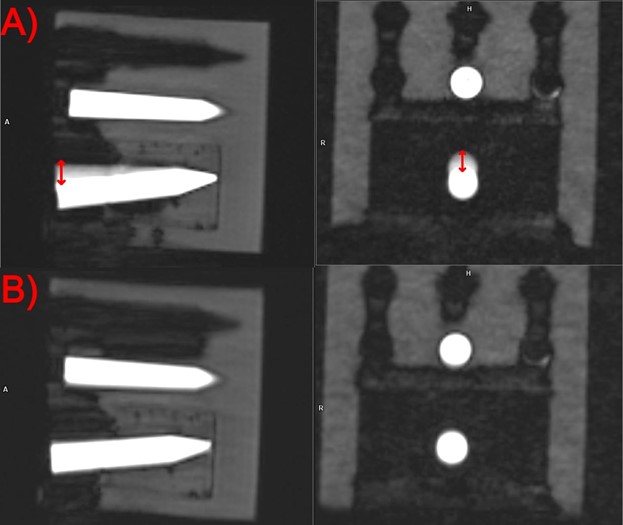
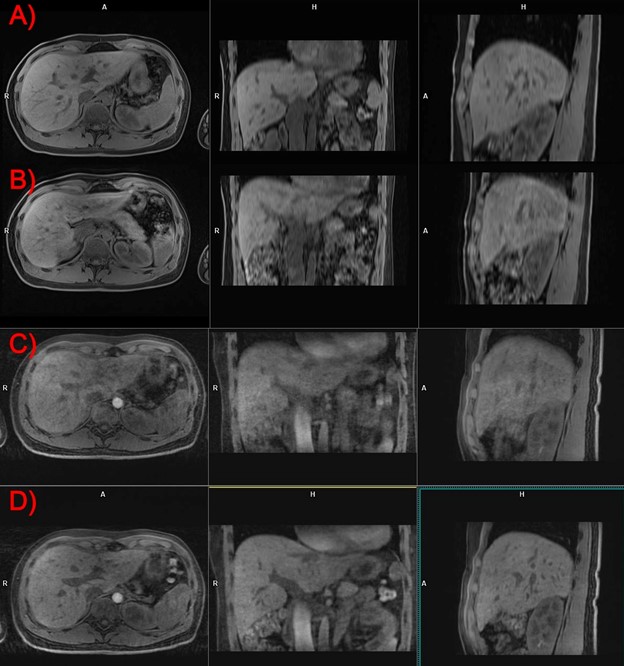
In figure 3 we observe the high similarity between the respiratory curves of the volunteer and the phantom in terms of amplitude and frequency.Figure 4.A shows the effect of motion in the 3D T1 Dixon water image (axial and coronal MPR reconstruction) when no navigator is not used. Figure 4.B highlights the outstanding motion corrected 3D T1 Dixon water image with iNAV-based non-rigid respiratory motion-corrected. The movement observed in figure 4.A was about 1cm which was in agreement with the in-vivo head-feet displacement of the liver measured in our MR volunteer scans.
We can appreciate the high-resolution 3D isotropic Dixon water images on the sagittal and coronal MPR reconstructions with sharper blood vessels and liver edges when compared to the current gold standard (5.A and 5.B).
Discussion
Our phantom, exhibiting a remarkable resemblance to human head-feet movement (Figure 3), demonstrates a strong similarity in amplitude and frequency with the predefined parameters on our function generator, signifying that our PET-MRI system reproduces images in a manner akin to those acquired from our human subject.When it comes to displacement analysis, our results reveal outstanding motion correction in the phantom image. Furthermore, human images exhibit a vivid visualization of larger and medium-sized liver vessels, characterized by clear edges. It's important to note that our motion-corrected images may have some limitations in capturing some smaller vessels effectively (Figure 5). Nevertheless, these first findings offer great promise, especially in challenging scenarios like breath-hold imaging, where it could significantly benefit non-cooperative patients.
Conclusion
Our novel MRI sequence enhances liver 3D T1 Dixon image quality, setting the stage for MR-guided motion correction in PET imaging. This holds promise for streamlined patient care and earlier treatment assessments.Acknowledgements
Siemens Healthcare, Courbevoie, France for financing my PhD projectReferences
1. Munoz, C., et al., Motion-corrected simultaneous cardiac positron emission tomography and coronary MR angiography with high acquisition efficiency. Magn Reson Med, 2018. 79(1): p. 339-350.
2. Lavdas, I., et al., A phantom for diffusion-weighted MRI (DW-MRI). J Magn Reson Imaging, 2013. 38(1): p. 173-9.
3. Zeilinger, M.G., et al., Non-rigid motion-corrected free-breathing 3D myocardial Dixon LGE imaging in a clinical setting. Eur Radiol, 2022. 32(7): p. 4340-4351.
4. Johnson, K.M., et al., Improved least squares MR image reconstruction using estimates of k-space data consistency. Magn Reson Med, 2012. 67(6): p. 1600-8.
5. Modat, M., et al., Fast free-form deformation using graphics processing units. Comput Methods Programs Biomed, 2010. 98(3): p. 278-84.
6. Batchelor, P.G., et al., Matrix description of general motion correction applied to multishot images. Magn Reson Med, 2005. 54(5): p. 1273-80.
Figures