0754
Frequency Modulated Continuous Wave Radar-based respiratory motion correction for cardiac MRI: Initial Results1ShanghaiTech University, Shanghai, China, 2United Imaging Healthcare, Shanghai, China, 3UIH America, Inc., Houston, TX, United States, 4Shanghai Clinical Research and Trial Center, Shanghai, China
Synopsis
Keywords: Motion Correction, Motion Correction
Motivation: Cardiac MRI is susceptible to motion-induced artifacts because of the sequential data acquisition process.
Goal(s): Evaluate the feasibility of utilizing a Frequency Modulated Continuous Wave (FMCW) Radar as a quantitative respiratory motion correction signal for free-breathing cardiac MRI.
Approach: A short calibration scan was performed to establish a motion model relating the FMCW Radar signal to the respiratory-induced heart motion. The established model was then applied during the imaging scan to perform retrospective motion correction for each k-space readout line.
Results: The FMCW radar showed good correlation to the respiratory-induced heart motion, and the proposed method effectively improved the image quality.
Impact: This study demonstrated the feasibility of utilizing FMCW radar as a surrogate to accomplish motion correction in free-breathing cardiac MRI.
Introduction
Cardiac MRI is susceptible to motion-induced artifacts because of the sequential data acquisition process. These artifacts can result in poor image quality, repeated scans, and remain an impediment to clinical application.1,2 Recent years, the Frequency Modulated Continuous Wave (FMCW) radar 3,4 been developed to measure respiratory motion, but its potential application for respiratory motion correction remains unexplored. In this paper, we propose a novel technique using FMCW radar signals and a patient-specific motion model5-7 to correct respiratory motion during cine MRI.Method
Figure 1 illustrates the pipeline of this technique. In calibration scan, 2D images of the heart were acquired at end-diastole in both coronal and sagittal views to extract the heart's motion in the head-foot (HF), left-right (LR) and anterior-posterior (AP) directions, respectively. The displacement of the heart in the three directions was calculated for each individual imaging frame using a template matching method. The ROI of heart from a reference image was manually cropped as template, and retrospective 2D cross-correlation amongst the acquired images was used to extract spatially resolved translational motion information in the head-foot ($$$\Delta HF_{ext}$$$), anterior-posterior ($$$\Delta{AP}_{ext}$$$) and left-right ($$$\Delta{LR}_{ext}$$$) directions. Fractional polynomial regression was applied according to Eqs. (1,2,3) for modeling the relationship between respiratory-induced heart motion and FMCW radar signals to account for potential nonlinearity and improve model fitting.$$\begin{aligned}\Delta HF_{ext}&=a_{HF}+b_{HF}\times Radar+c_{HF}\times\sqrt{Radar},&(1)\\\\\Delta AP_{ext}&=a_{AP}+b_{AP}\times Radar+c_{AP}\times\sqrt{Radar},&(2)\\\\\Delta LR_{ext}&=a_{LR}+b_{LR}\times Radar+c_{LR}\times\sqrt{Radar},&(3)\end{aligned}$$
In Eqs. (1,2,3), $$$Radar$$$ represents the FMCW radar signal; and $$$a, b$$$ and $$$c$$$ represent model coefficients. To accommodate for hysteresis as previously observed,8 the calibration data was separated into inhalation and exhalation phases. During the imaging scan, our method utilized model coefficients and the FMCW radar signal acquired during the imaging scan to calculate the respiratory motion of heart ($$$\Delta HF_{cal},\ \Delta AP_{cal},\ \Delta LR_{cal}$$$) for each k-space readout line. The respiratory motion was retrospectively corrected via phase modulation of the k-space data prior to image reconstruction. In this study, we focused on assessing the correlation between respiratory-induced heart motion and FMCW radar signals by specifically analyzing in-plane motion from sagittal view.
Experiments
1. Calibration ScanCalibration scan involved acquiring dynamic cardiac data in sagittal and coronal views over 80 cardiac cycles. Each dynamic image was acquired during end-diastole with a 275 ms acquisition window.
2. ‘Realtime’ Cine Scan
Real-time cine scan was conducted in the sagittal view with free-breathing acquisition. Imaging parameters included FOV of 320 × 300 mm², TE/TR= 1/3.1 ms and flip angle=70°. The acquisition time per image was deliberately prolonged to 496 ms, hence enhances the distinction between the corrected and uncorrected image for comparison purposes.
3. Segmented Cine Scan
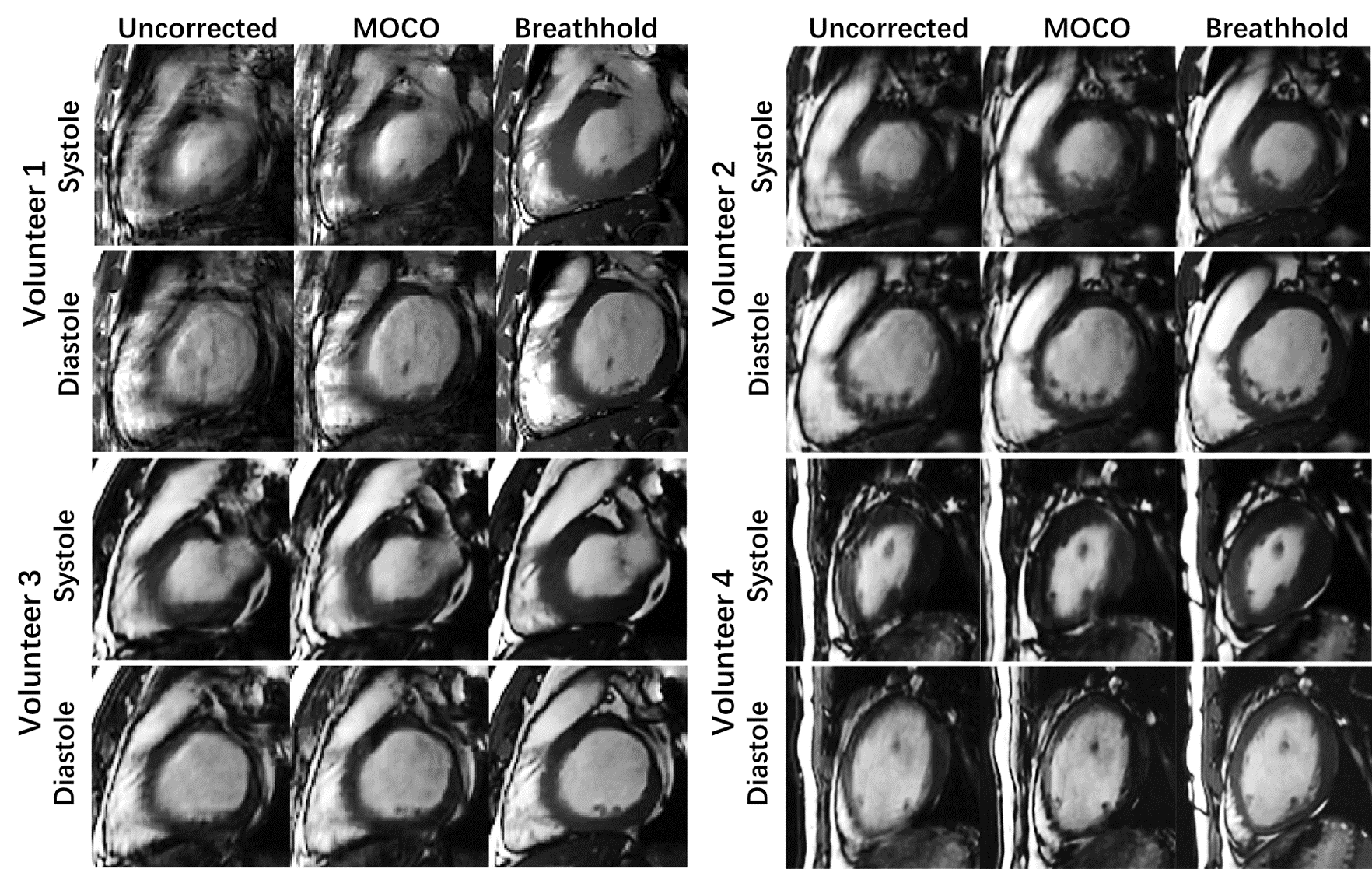
Segmented cine data were obtained during free-breathing, using the same parameters as for the realtime cine scan. The image quality with and without motion correction was compared. Additionally, we captured breath-holding segmented cine as reference images.
4. Test scan
A test scan used identical parameters to the calibration scan and included 8 subjects over 80 RR cycles. Heart motion was calculated and compared to motion extracted from dynamic images. To provide a measure of the error between the calculated motion and extracted motion over the duration of the test scan, the mean absolute error (MAE) and error range was calculated:
$$\begin{gathered}
\mathrm{MAE}=\frac{1}{80}\sum_{k=1}^{80}\bigl|\triangle HF_{\mathrm{cal}}(\mathrm{k})-\triangle HF_{ext}(\mathrm{k})\bigr|, \text{(4)} \\
\mathrm{range}=\max(|\triangle HF_{\mathrm{cal}}(\mathrm{k})-\triangle HF_{ext}(\mathrm{k})|), \text{(5)}
\end{gathered}$$
where $$$\Delta HF_{cal}(k)$$$ represents the average of the calculated motion of the central six readout lines in the $$$k$$$th frame. The same approach was also used with $$$|\Delta AP_{cal}-\Delta AP_{ext}|$$$ and $$$|\Delta LR_{cal}-\Delta LR_{ext}|$$$.
Results
Our method accurately calculated AP and LR cardiac motion with a precision of 1 mm during regular respiration, as illustrated in Figure 2. A summary of calculation error analysis is displayed in Figure 3. The mean absolute errors along HF, AP and LR directions were mm, mm and mm, respectively. Figure 4 shows 5 representative real-time cine images, our proposed method accurately corrects these respiratory-induced motion displacements. Figure 5 illustrates the end-systole and end-diastole phases of 4 volunteers captured during free-breathing, with and without retrospective motion correction. Note the substantial improvement of anatomical details in the motion-corrected images, whereas the uncorrected images suffered from noticeable blurring artifacts. Due to the lack of ground truth, only visual assessment was performed on image quality.Discussion
The proposed technique effectively reduces motion artifacts and improves image quality in free-breathing cine MRI. A limitation of this study is its narrow scope, which solely addresses the correction of in-plane motion while neglecting through-plane motion. To further advance this field, future investigations should explore the potential of the technique for real-time tracking of through-plane motion.Acknowledgements
No acknowledgement found.References
1. Zaitsev M, Maclaren J, Herbst M. Motion artifacts in MRI: A complex problem with many partial solutions. J Magn Reson Imaging. 2015;42(4):887-901.
2. Shechter G, Ozturk C, Resar JR, Mcveigh ER. Respiratory Motion of the Heart From Free Breathing Coronary Angiograms. IEEE Transactions on Medical Imaging. 2004;23(8):1046-1056.
3. Wang H, Li Y, Xia X, Hu L, Zhao J, Chen Q. Non-contact respiratory triggering for clinical MRI using frequency modulated continuous wave radar. Paper presented at: Medical Imaging 2021: Physics of Medical Imaging; 2021-02-15, 2021.
4. He M, Nian YJ, Gong YS. Novel signal processing method for vital sign monitoring using FMCW radar. Biomed Signal Proces. 2017;33:335-345.
5. Mcclelland JR, Hawkes DJ, Schaeffter T, King AP. Respiratory motion models: A review. Medical Image Analysis. 2013;17(1):19-42.
6. Bush MA, Ahmad R, Jin N, Liu Y, Simonetti OP. Patient specific prospective respiratory motion correction for efficient, free-breathing cardiovascular MRI. Magnetic Resonance in Medicine. 2019;81(6):3662-3674.
7. Ludwig J, Speier P, Seifert F, Schaeffter T, Kolbitsch C. Pilot tone–based motion correction for prospective respiratory compensated cardiac cine MRI. Magnetic Resonance in Medicine. 2021;85(5):2403-2416.
8. Burger I, Meintjes EM. Elliptical subject-specific model of respiratory motion for cardiac MRI. Magnetic Resonance in Medicine. 2013;70(3):722-731.
Figures
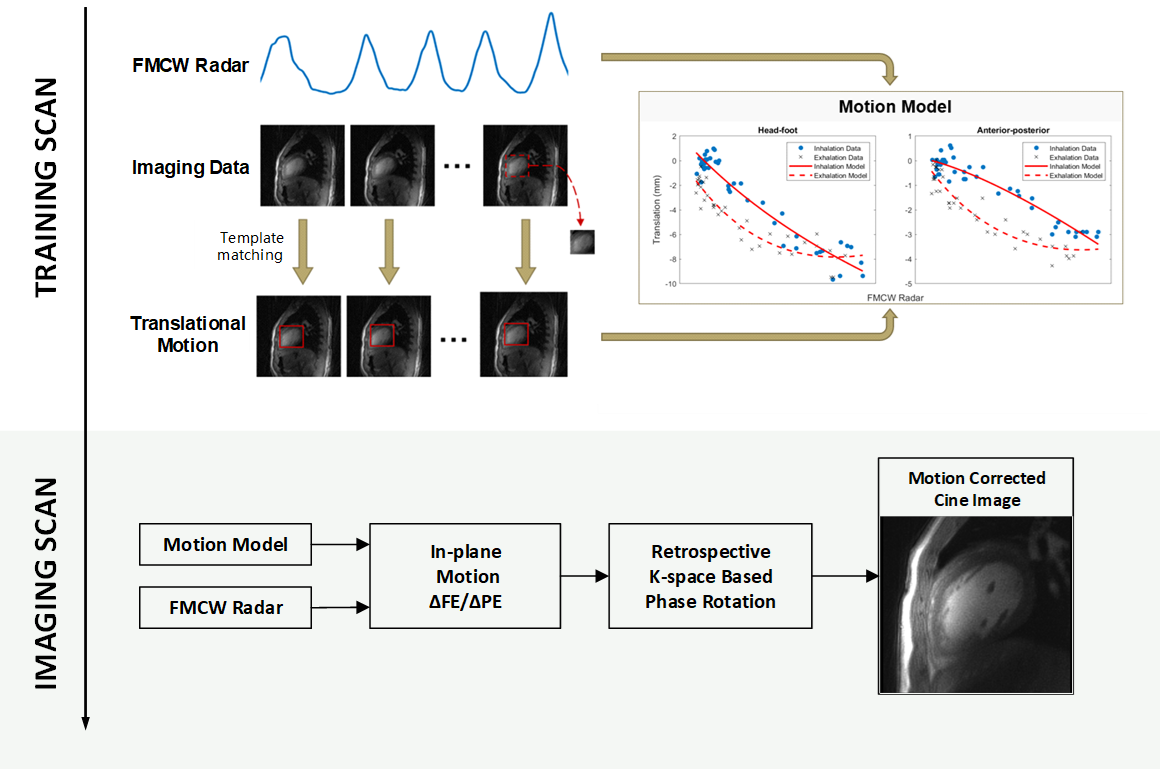
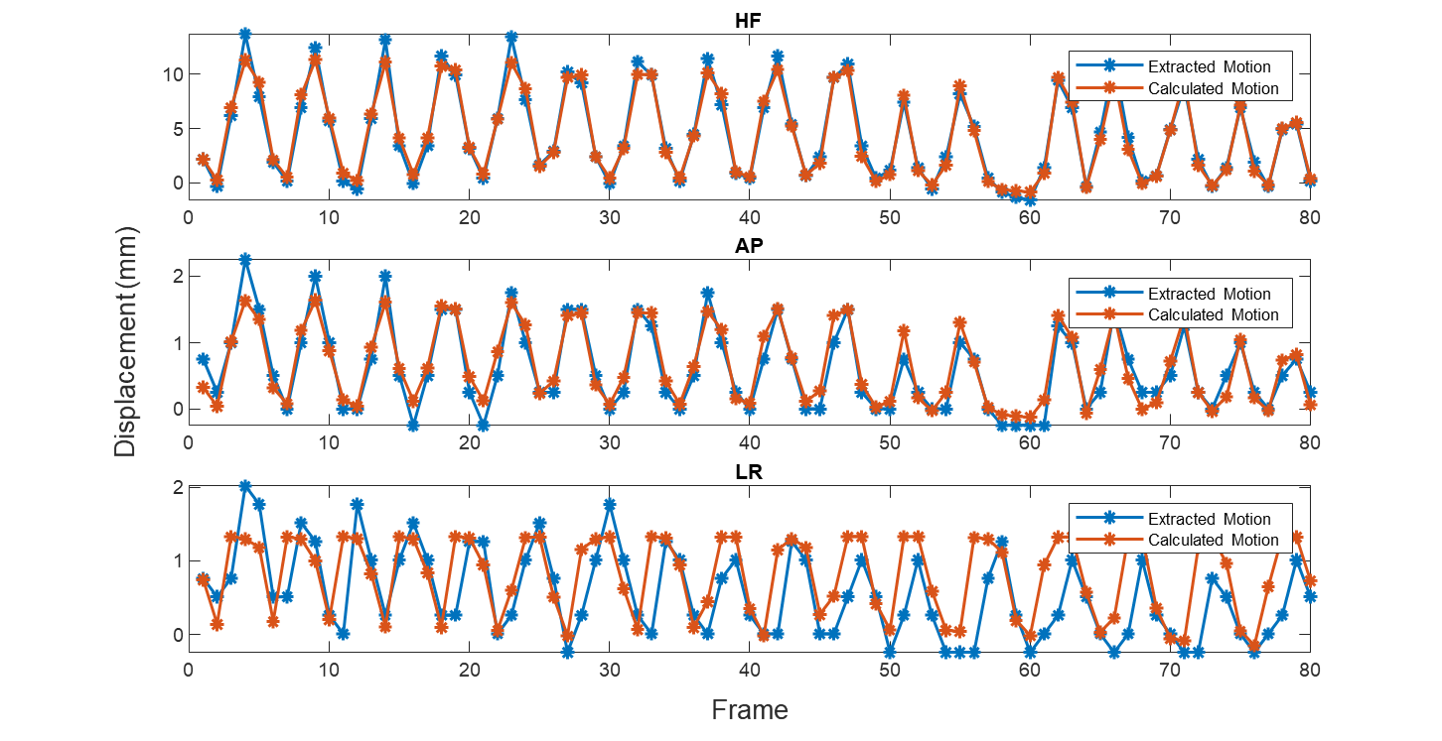
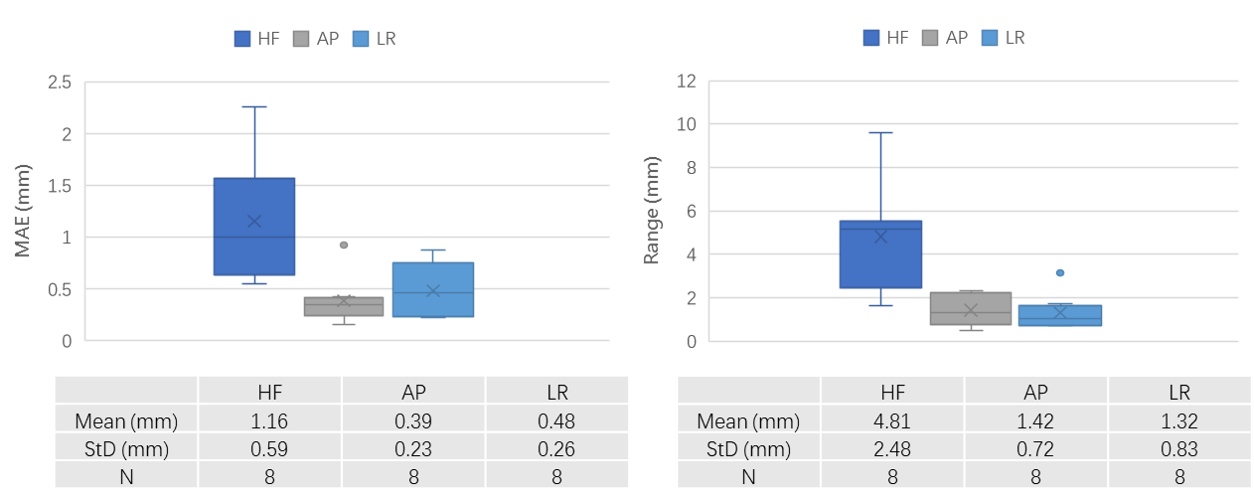
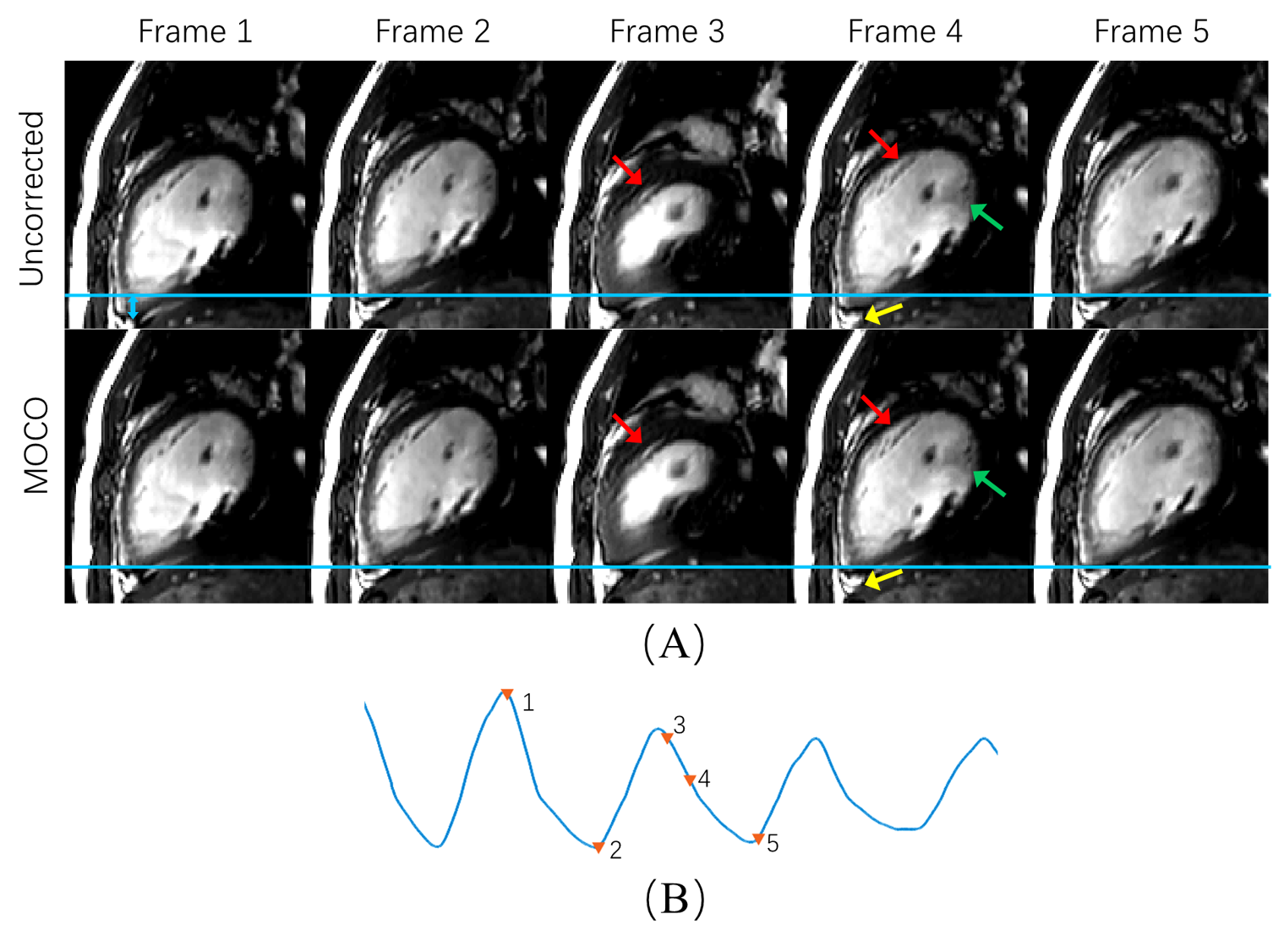
Figure 4 A, Comparison of free-breathing, 2D real-time scans with 50 repetitions, without and with FMCW radar-based in-plane motion correction (MOCO). B, Heart displacement calculated from synchronized recorded FMCW radar signal. Five representative frames with red triangle annotations indicating positions have been selected for presentation and were referenced with a horizontal blue line. This method effectively minimizes respiratory-induced heart motion across various cardiac phases in real-time scans (blue arrow).