0753
Free-breathing SMS-bSSFP myocardial perfusion imaging with prospective slice-tracking and AI-based reconstruction1School of Biomedical Engineering and Imaging Sciences, Faculty of Life Sciences and Medicine, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 3MR Physics, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, 4Cardiovascular predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 5MR Research Collaborations, Siemens Healthcare Limited, Melbourne, Australia
Synopsis
Keywords: Motion Correction, Perfusion, free breathing, myocardial perfusion, simultaneous multi-slice, prospective motion-correction, machine learning/artificial intelligence
Motivation: Simultaneous multi-slice-bSSFP shows promise for myocardial perfusion imaging with high spatial coverage/resolution. Free-breathing acquisitions are desirable but currently result in large through-plane motion.
Goal(s): To develop a free-breathing SMS-bSSFP myocardial perfusion technique with high spatial coverage/resolution and prospective through-plane motion correction.
Approach: Prospective slice-tracking using fastNAV was implemented into an SMS-bSSFP perfusion sequence. Image reconstruction used TGRAPPA combined with a deep learning-based complex-value image denoiser. This technique was evaluated in 10 patients undergoing two rest SMS perfusion scans with/without fastNAV.
Results: The proposed approach resulted in significant motion reduction, low noise-level reconstruction, and no degradation of myocardial sharpness.
Impact: This study demonstrates the feasibility of prospective slice tracking in an SMS perfusion sequence. Combined with the proposed deep learning-based reconstruction, it provides a myocardial perfusion protocol with increased spatial coverage, high spatial resolution, and feasible under free-breathing conditions.
Background
Simultaneous multi-slice (SMS) bSSFP imaging is an acceleration technique which shows promise for myocardial perfusion imaging by providing increased spatial coverage and high spatial resolution(1,2). SMS images can be reconstructed using iterative reconstruction techniques which often incorporate temporal regulation that can introduce bias in the signal temporal profile (1,2). Deep learning-based reconstruction using TGRAPPA and a magnitude-based image denoising (NoiseMapNet) was recently demonstrated as a successful alternative to preserve temporal consistency of the signal (3). Furthermore, free-breathing acquisitions are desirable as breath holding is not feasible in all patients. However, the resulting through-plane respiratory motion remains mostly uncorrected, as prospective slice tracking is challenging due to failing respiratory signal in the presence of prior saturation pulses. In this study, we have developed a free-breathing SMS-bSSFP acquisition with prospective slice tracking for through-plane motion compensation and a novel deep-learning (AI) based reconstruction.Methods
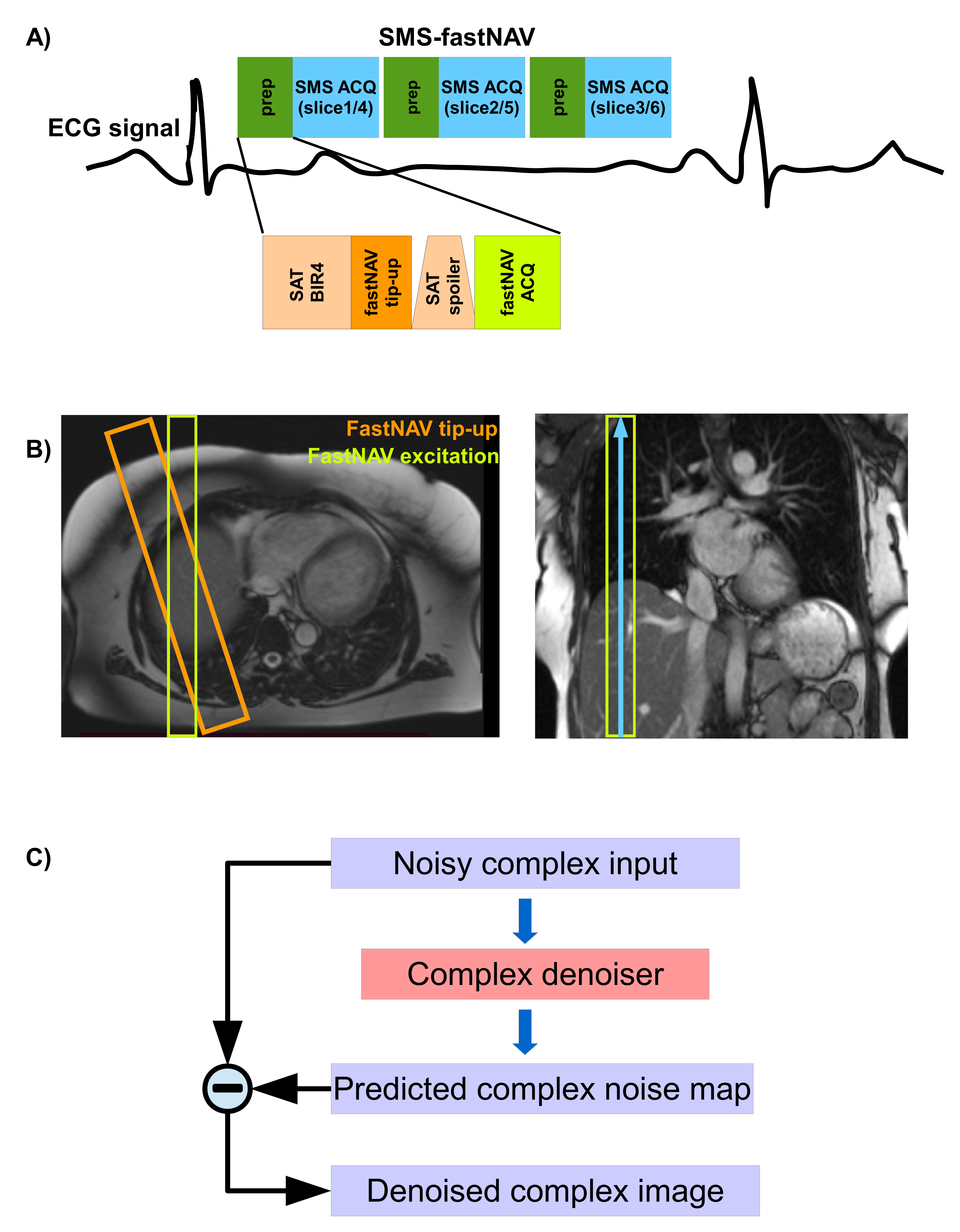
Pulse sequenceImages were acquired using a free-breathing saturation recovery SMS-bSSFP sequence with CAIPIRINHA encoding, GC-LOLA and a “lean” implementation for slice separation (4). Prospective slice tracking was implemented in foot-head direction using a fast diaphragmatic respiratory navigator (fastNAV) (5) acquired prior to each SMS readout. FastNAV consists of introducing a 90° slice selective tip-up pulse (20mm) to restore longitudinal magnetisation between the excitation (non-selective BIR-4) and spoiler of the saturation pulse. The fastNAV signal is then acquired from another slice-selective excitation pulse (FA=15°) intersecting the tip-up slice, as seen in Figure 1A,1B.
Image reconstruction
Image reconstruction consisted of TGRAPPA followed by a new complex-value 2D image denoising network (C-NoiseMapNET), shown in Figure 1C. This network was trained on real and imaginary noisy images to output their respective estimated noise maps. The denoising is then performed by subtracting the noise maps from the noisy images. A patch-based training was done on 764 complex high SNR CINE images with different orientations (SHAX, 2CH, 3CH, 4CH) and simulated Gaussian noise in the complex-value images. Network parameters include the mean squared error for the cost function, dropout, Adam optimiser and weight decay.
In-vivo evaluation
All imaging was done using a 1.5T scanner (Magnetom Aera Siemens Healthcare, Erlangen, Germany). Ten patients (7/3 males/females, average age 59±10 years) referred for clinical CMR were recruited for this study. For each patient, two perfusion protocols (0.075 mmol/kg gadobutrol bolus injection for each) were performed in a randomised order with a 10 mins gap: SMS-bSSFP with no fastNAV (SMS) and SMS-bSSFP with fastNAV (SMS-fastNAV). Both sequences used the same SMS bSSFP imaging parameters: slice number: 6, spatial resolution 1.9x19mm2, slice thickness: 10mm, TE/TR/FA: 1.24ms/2.9ms/50°, in-plane TGRAPPA acceleration factor: 3.5, and multiband factor: 2. All scans were reconstructed using TGRAPPA-only and the proposed reconstruction.
Quantitative analysis
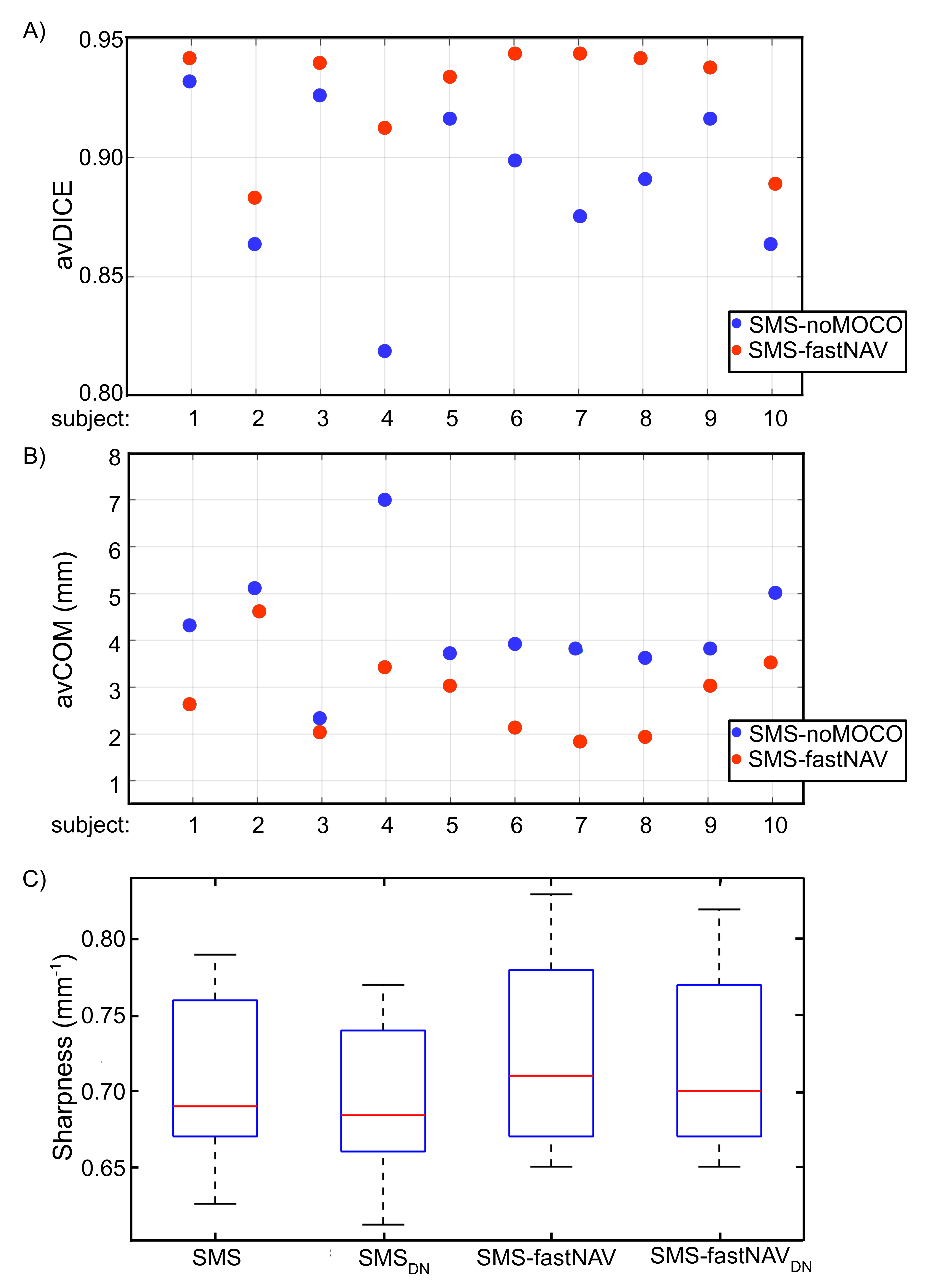
For each patient, quantification of the temporal alignment of the LV across all dynamics where the LV is visible (i.e. from contrast arrival) was done by obtaining the average DICE coefficient of the LV (avDICE) and average displacement of the LV centre of mass location (avCOM) (6). Myocardial sharpness was compared between the TGRAPPA-only and proposed reconstructions (6,7).
Results
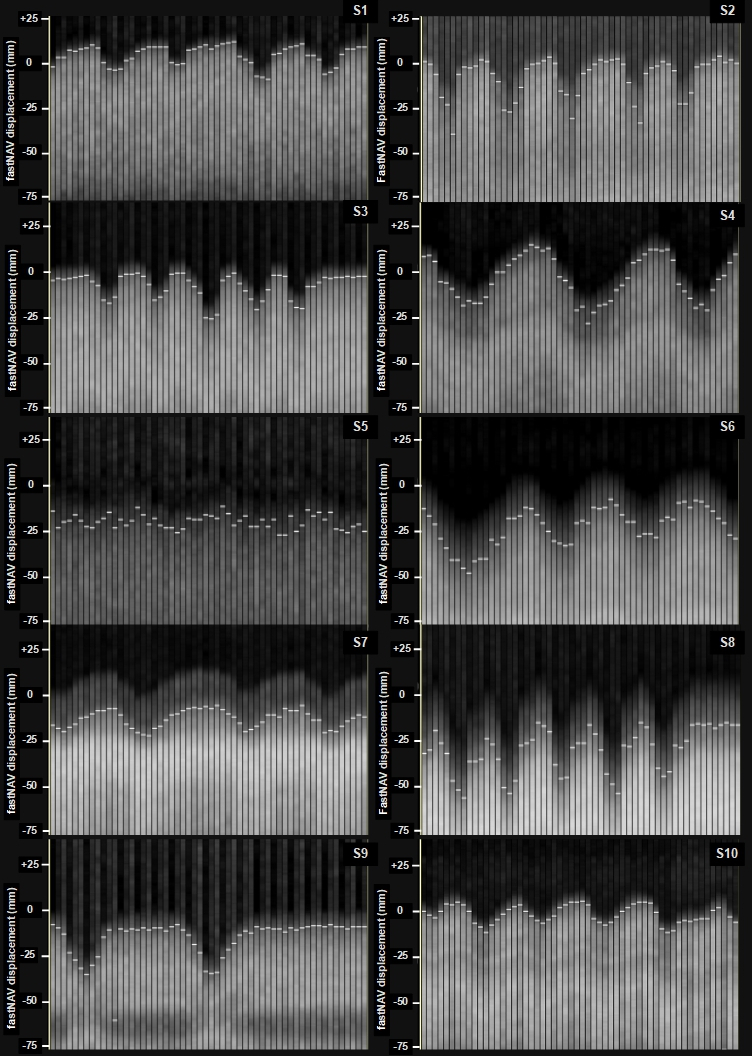
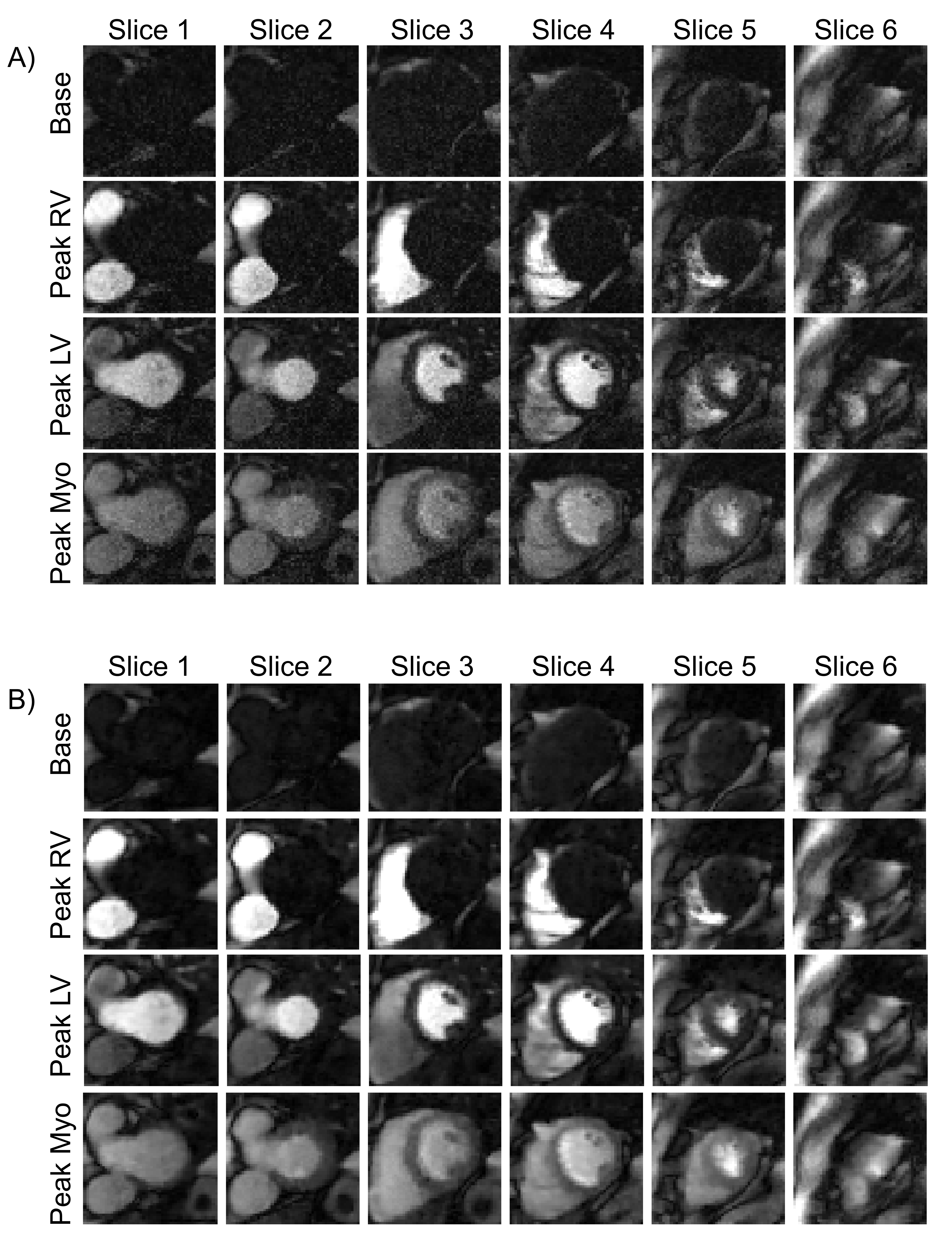
Figure 2 shows the navigator tracking signal and position acquired from the different subjects. Figure 3 shows an example case of images acquired using SMS and SMS-fastNAV, where SMS-fastNAV resulted in substantially decreased apparent motion. Figure 4 shows the impact of the proposed reconstruction on a SMS-fastNAV acquisition in another patient. Over all subjects (see Figure 5), SMS-fastNAV led to higher avDICE score (0.93 ± 0.02 vs. 0.89 ±0.04 for SMS, p<0.0013) and decreased avCOM (2.82 ±0.89mm vs. 4.23 ±1.29mm for SMS, p=0.0051). There were no statistically significant differences in myocardial sharpness between the TGRAPPA-only and proposed reconstructions for both SMS data (0.69 ±0.09mm-1 vs. 0.68±0.1mm-1, p=0.73) and SMS-fastNAV data (0.72 ±0.1mm-1 vs. 0.71 ±0.08mm-1, p=0.75).Discussion
SMS-fastNAV successfully reduced through-plane motion as reflected by reduced apparent motion in the images, and shows promise for free breathing CMR perfusion. The proposed C-NoiseMapNet provides efficient noise suppression from the initial TGRAPPA reconstruction while preserving image sharpness, thus enabling high acceleration factor necessary for high spatial resolution. This approach can easily be combined with further in-plane motion reduction, which will be explored in future work.Conclusion
SMS-fastNAV combined with advanced image reconstruction enables free-breathing CMR perfusion with increased spatial coverage, high spatial resolution, reduced through-plane and in-plane motion, low noise-level reconstruction, and no degradation of myocardial sharpness.Acknowledgements
This work was supported by the Innovate UK grant (68539), the Engineering and Physical Sciences Research Council (EPSRC) grant (EP/R010935/1), the British Heart Foundation (BHF) grants (PG/19/11/34243 and PG/21/10539), the Wellcome EPSRC Centre for Medical Engineering at Kings College London (WT 203148/Z/16/Z), the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, and Government of Botswana. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Nazir MS, Neji R, Speier P, et al. Simultaneous multi slice (SMS) balanced steady state free precession first-pass myocardial perfusion cardiovascular magnetic resonance with iterative reconstruction at 1.5 T. Journal of Cardiovascular Magnetic Resonance 2018;20(1).
2. Nazir Muhummad S, Milidonis X, McElroy S, et al. Quantitative Myocardial Perfusion With Simultaneous-Multislice Stress CMR for Detection of Significant Coronary Artery Disease. JACC: Cardiovascular Imaging 2022;15(9):1672-1674.
3. Adam N, Kowalik T, Tyler A, et al. Fast reconstruction of SMS bSSFP myocardial perfusion images using a combination of parallel imaging and AI-based denoising. Proceedings of the Joint Annual Meeting ISMRM-ESMRMB (31st Annual Meeting & Exhibition), International Society for Magnetic Resonance in Medicine, Ed; 2023. (abstract 4298).
4. Stäb D, Speier P. Gradient-controlled local Larmor adjustment (GC-LOLA) for simultaneous multislice bSSFP imaging with improved banding behavior. Magnetic Resonance in Medicine 2019;81(1):129-139.
5. Mooiweer R, Neji R, Mcelroy S, et al. A fast navigator (fastNAV) for prospective respiratory motion correction in first‐pass myocardial perfusion imaging. Magnetic Resonance in Medicine 2021;85(5):2661-2671.
6. Roujol S, Foppa M, Basha TA, et al. Accelerated free breathing ECG triggered contrast enhanced pulmonary vein magnetic resonance angiography using compressed sensing. Journal of Cardiovascular Magnetic Resonance 2014;16:1-9.
7. McElroy S, Ferrazzi G, Nazir MS, et al. Combined simultaneous multislice bSSFP and compressed sensing for first-pass myocardial perfusion at 1.5 T with high spatial resolution and coverage. Magn Reson Med 2020;84(6):3103-3116.
Figures