0751
Pilot Tone Navigated Motion Correction in DCE-MRI1Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
Keywords: Motion Correction, DSC & DCE Perfusion, Motion Correction
Motivation: Addressing the challenge of respiratory motion in abdominal DCE-MRI, especially in pediatric patients, to improve image quality and enhance quantitative DCE-MRI analysis.
Goal(s): To develop a motion correction method using PilotTone navigators (PTnavs) to enhance DCE-MRI quality and reliability.
Approach: We extract PTnav, create a linear motion model using binning based reference motion parameters. We then apply the motion model to the PTnav for each spoke to estimate its motion and correct for it. We evaluate the method on non-contrast volunteer and pediatric DCE-MRI data.
Results: Successful elimination of motion artifacts and improved image quality, reduced image alignment and improved signal-time-intensity curves.
Impact: The proposed PT-based motion correction effectively overcomes the challenges of previous motion correction methods, eliminating respiratory motion artifacts and enhancing image quality and misalignment in high-temporal-resolution DCE-MRI. This advancement improves diagnostic accuracy, particularly in pediatric cases with unpredictable breathing patterns.
Introduction
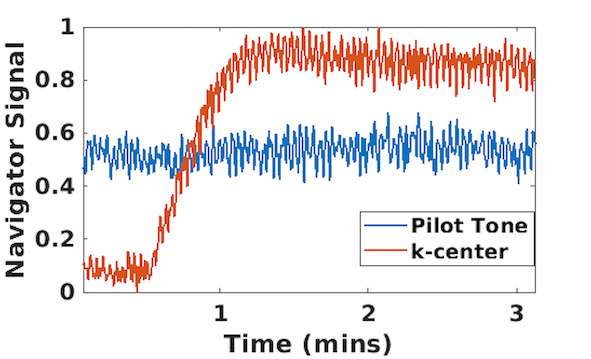
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) is a valuable tool for detailed analysis of abdominal anatomy with high resolution. However, it faces a significant challenge due to respiratory motion, especially in pediatric patients with unpredictable breathing patterns1. While radial imaging can help reduce motion artifacts to some extent, image quality can still suffer, particularly in such cases. As a result, the images often lack the necessary anatomical details for clinical evaluation. Internal navigators such as k-space-center or FID navigators2-5 are influenced by the injection of contrast material, making them unsuitable for measuring motion accurately. Recently, there has been promising progress in tracking physiological motion independently of MRI signal and contrast dynamics using a wireless RF transmitter that generates a reference signal called the Pilot-Tone (PT)6-8 (Figure 1). However, the PT signal alone does not directly provide motion parameters and requires calibration. In this context, we propose a retrospective motion correction method that relies on PT-based motion measurements. To convert the PT navigator signal into motion parameters, we establish a linear motion model by analyzing reference motion measurements from each respiratory bin after applying binning (i.e., XD-GRASP9) and averaging the PT signal in each bin, using only a small portion of the data. We evaluated the effectiveness of our proposed method using two non-contrast volunteer exams and one pediatric patient undergoing DCE-MRI.Methods
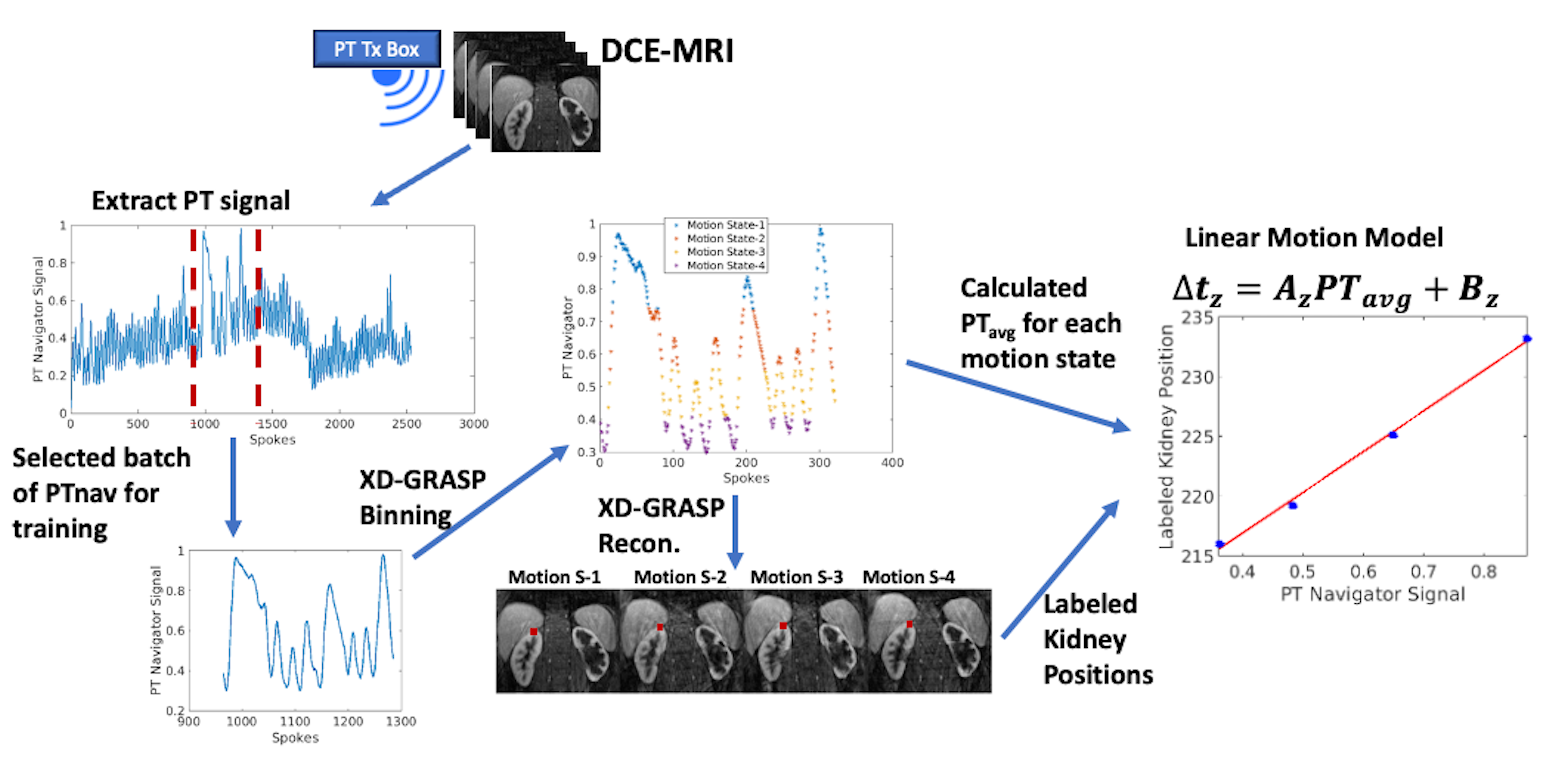
MR Experiments: To capture PT navigator signal, we placed the PT transmitter box by the subject's hip on the patient table. We scanned two volunteers (both 41 years old, one female and one male) using a 3T MRI scanner (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) with their written consent. We used spine and body matrix coils, and the volunteers breathed freely and irregularly for a 2.5 minutes scan. Imaging parameters included TE/TR/FA = 1.49ms/4ms/9˚, 32 coronal slices (Partial Fourier = 6/8), voxel size = 1.2x1.2x3mm3, and 1326 radial spokes. Additionally, we recorded PT navigator data during DCE-MRI exams of three pediatric patients (one female, two male, age range=2-17 years) at 3T MRI scanner MAGNETOM Prisma/Skyra, Siemens Healthineers, Erlangen, Germany) with informed consent. One of the patients was non-sedated, free-breathing and the other two were under sedation during the scan. In the DCE-MRI exam 2536 spokes were acquired and the other imaging parameters were the same.Motion Correction: The proposed motion correction (MoCo) method is outlined in Figure 2. We began by extracting the multi-channel PT navigator signal from raw data. To identify the most representative physiological motion signal, we applied principal component analysis and coil clustering. Within a window of approximately 300 spokes, we employed XD-GRASP to categorize the data into around 6-8 motion states or bins and calculated the average PT navigator value for each bin. We also marked the uppermost point of the right kidney for each bin. A linear motion model was then constructed based on the kidney's position in each bin and the average PT navigator signal for each bin. After calibrating this model, we applied the PT-based motion model to each k-space line in the whole scan, modifying its phase to correct for oblique z-translation motion in k-space. Subsequently, we reconstructed the motion-corrected k-space data and used GRASP reconstruction to generate a dynamic series of volumes for the patient data.
Results
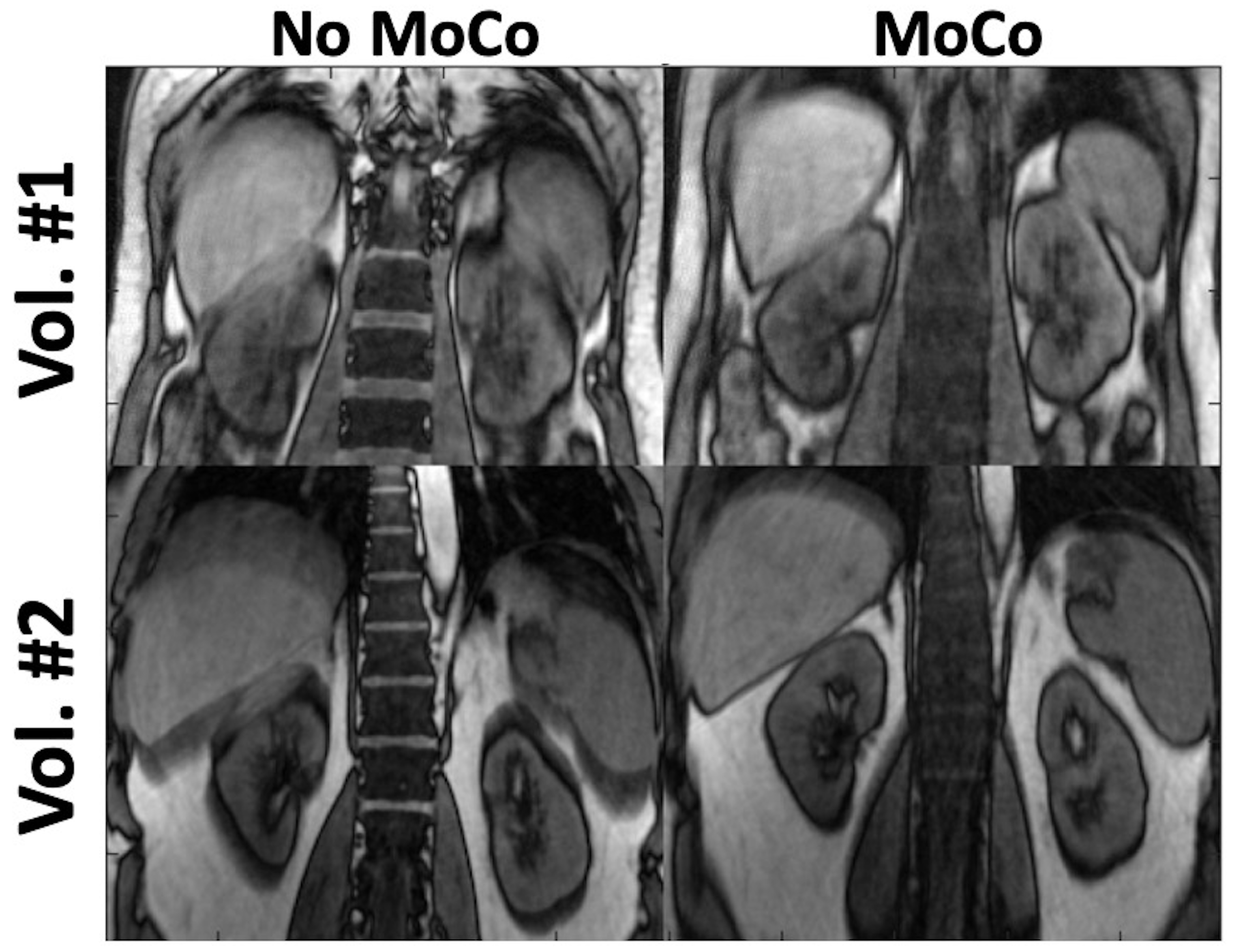
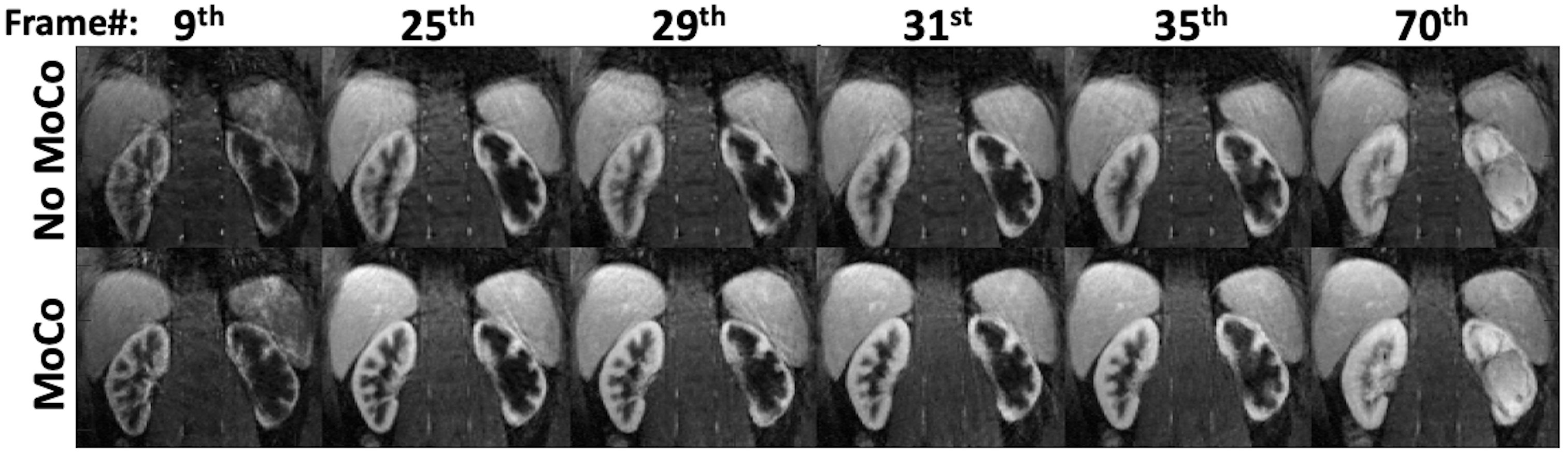
With and without MoCo, single volumes (i.e. using 1326 spokes) generated from non-contrast volunteer exams are compared in Figure 3. Figure 4 demonstrates a dynamic image series each reconstructed from 34 spokes for MoCo and noMoCo for one patient. The other two patients, who were under sedation, did not have heavy breathing during the acquisition. In Figure 5, extracted contrast signal curves are compared for with and without MoCo along with animated GIF of dynamic series.Discussion and Conclusion
Current motion correction techniques, such as binning and XD-GRASP reconstruction, are unsuitable for high-temporal-resolution DCE-MRI data because reconstructing each volume in at high temporal resolution (<3s), as needed for accurate functional information, would result in too few radial lines per bin, diminishing their efficacy. Alternative navigators like k-space center and FIDnav are ineffective in early phases after contrast injection because their signal is influenced by both motion and contrast changes. In contrast, our PT-based motion correction is suitable for DCE-MRI and could effectively eliminate motion artifacts in non-contrast volunteer data (Figure 3) and DCE-MRI patient data (Figure 4), improving image quality.Acknowledgements
This work was supported partially by the National Institute of Diabetic and Digestive and Kidney Diseases (NIDDK), National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Institute of Neurological Disorders and Stroke (NINDS) and National Library of Medicine (NLM) of the National Institutes of Health under award numbers R01DK125561, R21DK123569, R21EB029627, R01NS121657, R01LM013608, S10OD0250111. We thank the Center for Advanced Imaging Innovation and Research (CAI2R) at NYU for supplying the 3T Pilot Tone device used in this work.References
[1] Chavhan, Govind B., Paul S. Babyn, and Shreyas S. Vasanawala. "Abdominal MR imaging in children: motion compensation, sequence optimization, and protocol organization." Radiographics 33.3 (2013): 703-719.
[2] Ariyurek C, Wallace TE, Kober T, Kurugol S, Afacan O. Prospective motion correction in kidney MRI using FID navigators. Magn Reson Med. 2023;89:276-285.
[3] Brau ACS, Brittain JH. Generalized self-navigated motion detection technique: Preliminary investigation in abdominal imaging. Magn Reson Med. 2006;55(2):263-270.
[4] Kober T, Marques JP, Gruetter R, Krueger G. Head motion detection using FID navigators. Magn Reson Med. 2011;66(1):135-143.
[5] Wallace TE, Afacan O, Waszak M, Kober T, Warfield SK. Head motion measurement and correction using FID navigators. Magnetic Resonance in Medicine. 2019;81(1):258-274.
[6] Ludwig, Juliane, et al. "Pilot tone–based motion correction for prospective respiratory compensated cardiac cine MRI." Magnetic Resonance in Medicine 85.5 (2021): 2403-2416.
[7] Falcão, M. B. L. et al. Pilot tone navigation for respiratory and cardiac motion-resolved free-running 5D flow MRI. Magn Reson Med 87, 718–732 (2022).
[8] Solomon, Eddy, et al. "Free-breathing radial imaging using a pilot-tone radiofrequency transmitter for detection of respiratory motion." Magnetic resonance in medicine 85.5 (2021): 2672-2685.
[9] Feng, Li, et al. "XD-GRASP: golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing." Magnetic resonance in medicine 75.2 (2016): 775-788.
Figures