0750
TR-resolved Real-Time Low-Field CMR using Hermitian Motion Corrected Reconstructions1Radiology, University of Michigan, Ann Arbor, MI, United States, 2Biomedical Engineering, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Motion Correction, Low-Field MRI, Real-time
Motivation: Real-time cardiac MR could provide new insights into function of the myocardium while avoiding artefacts arising from cardiac and/or respiratory motion.
Goal(s): High temporal resolution real-time cardiac MR is particularly challenging at low field (0.55T) due reduced SNR and coil elements available on commercial systems.
Approach: Here, we leverage motion compensated reconstructions and Hermitian symmetry to enable the highly undersampled reconstructions required for real-time cardiac MR at low field.
Results: Experiments at 0.55T show that the proposed approach enables imaging with a temporal resolution of 6 ms (R~48x) with minimal aliasing, outperforming conventional compressed sensing (considerable aliasing) and parallel imaging (aliasing dominated).
Impact: TR-resolved (6ms temporal resolution) real-time cardiac is demonstrated at 0.55T where SNR is limited. Such highly accelerated imaging may reveal finer details in myocardial function. Additionally, the high acceleration factors achieved here could also be leveraged for 3D real-time imaging.
INTRODUCTION:
MR cardiac cine is the gold-standard to evaluate ejection fraction, a key evaluation of cardiac function, and a predictor/assessor of heart failure. Conventional cine images are acquired during a breath-hold to avoid respiratory motion artefacts, but residual artefacts may arise from respiratory drift, arrhythmia or bulk motion. Real-time imaging is an approach in which images are collected with a high temporal resolution such that these limitations can be bypassed. However, high acceleration factors are required for real-time imaging, potentially resulting in aliasing and noise amplification. While parallel imaging1,2,3 and compressed sensing4,5,6,7 have been successfully deployed for this application at 1.5T and above, these methods may be insufficient at lower fields due to reduced SNR and reduced/sub-optimal number of coils available. Here, we develop a novel Hermitian Motion Corrected (MCH) reconstruction that incorporates knowledge of real-time motion and Hermitian symmetry into the forward model, allowing the MCH approach to tackle high acceleration factors in low SNR applications. We deploy MCH for 2D real-time cardiac MR at 0.55T, demonstrating its ability to achieve a temporal resolution of 6 ms (same as the TR) with a spatial resolution of 2.2x2.2 mm2. The proposed approach was evaluated in five healthy subjects and compared with iterative SENSE and Total Variation (TV) reconstructions.METHODS:
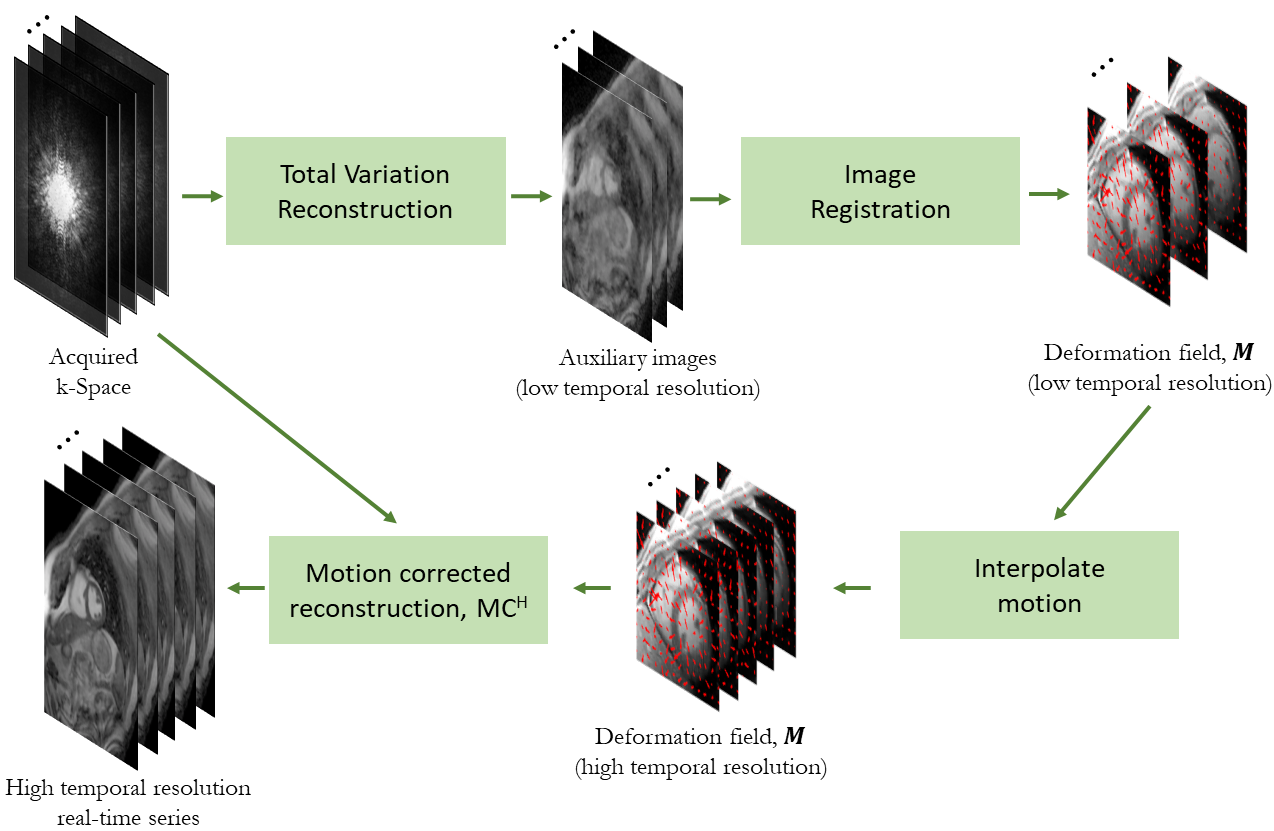
The proposed MCH incorporates motion into the reconstruction8,9 in combination with the Virtual Coil Concept (VCC)10, further leveraging Hermitian symmetry. MCH employs the following optimization:$$\widehat{x}=argmin_{x}\left\|SF\binom{P}{P^{*}}\binom{C}{C^{*}}Mx-\binom{s}{s'}\right\|_{2}^{2}$$
where x is the real-time image series; S is the sampling trajectory; F is the Fourier transform; P is the image phase; C are coil sensitivities; s are the acquired k-space data; $$$s'(k)=s^{*}(-k)$$$ (where k denotes the k-space coordinate); and M are the deformation fields capturing the real-time motion. A single phase map is estimated from a reconstruction of the complete acquired data. Preliminary spatial and temporal TV (as employed by XD-GRASP11) reconstruction is performed using data over 10 TRs (60 ms temporal resolution). Elastic motion is estimated via local cross-correlation based image registration12,13 of this preliminary image series. The estimated motion fields (assumed to be smooth over time) are interpolated to a 6 ms (single-TR) temporal resolution. Finally, the 6 ms temporal resolution motion fields are incorporated into the proposed MCH reconstruction (Fig.1).
EXPERIMENTS:
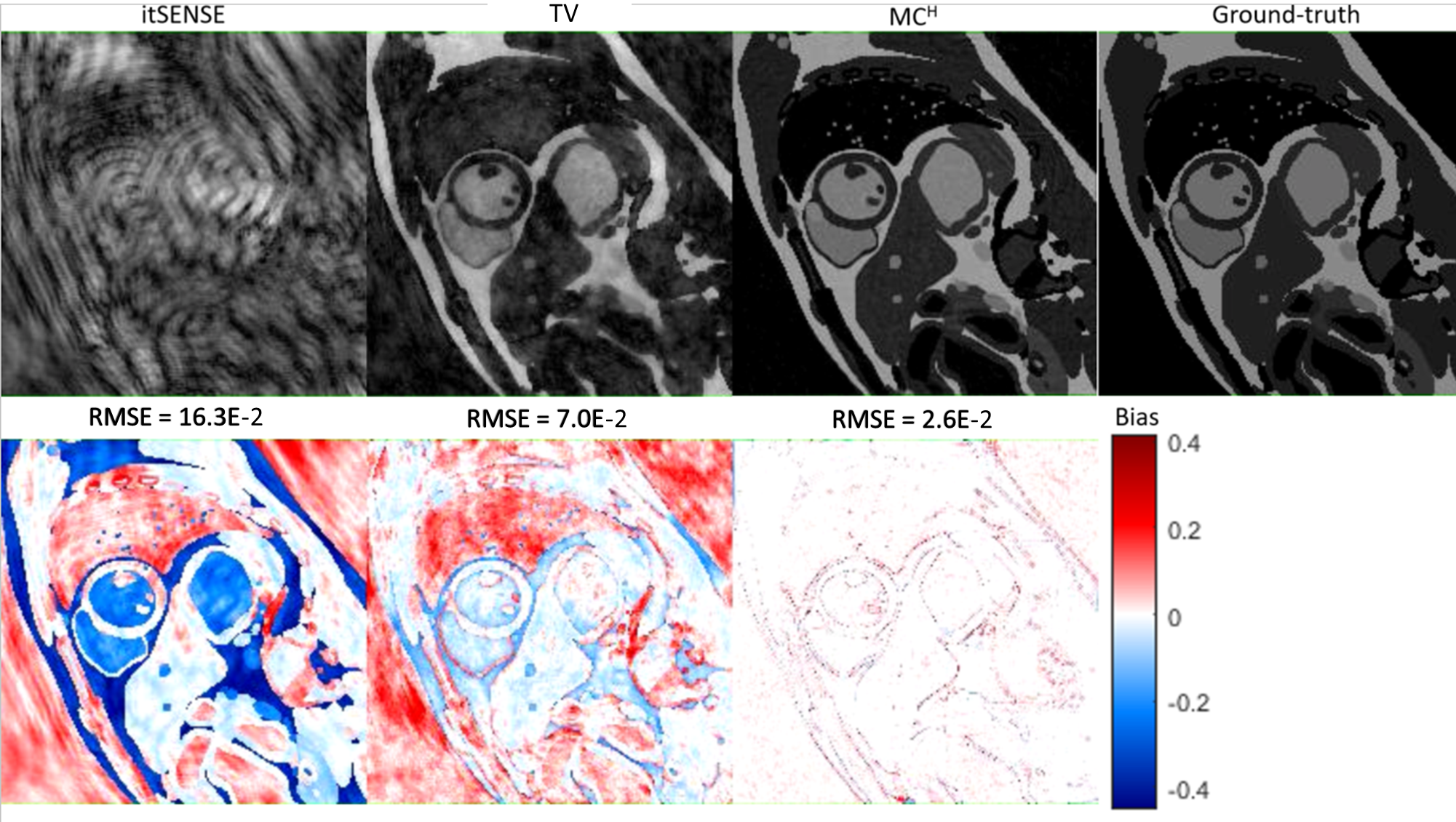
Numerical simulations based on MRXCAT14 were performed, with realistic (respiratory and cardiac) motion, noise, spiral undersampling, phase inhomogeneities and coil sensitivities. Five subjects were imaged at 0.55T with FOV=280x280mm2; 8mm slice thickness; resolution=2.2x2.2mm2; TE/TR=1.8/6.3 ms; flip angle=105º; bSSFP readout; golden angle spiral trajectory (48 arms for full sampling). Data were reconstructed with iterative SENSE, TV and the proposed MCH with an acceleration factor of R~48 (6 ms temporal resolution). Iterative SENSE and MCH were solved with (linear) conjugate gradient; TV was solved with the non-linear conjugate gradient.RESULTS:
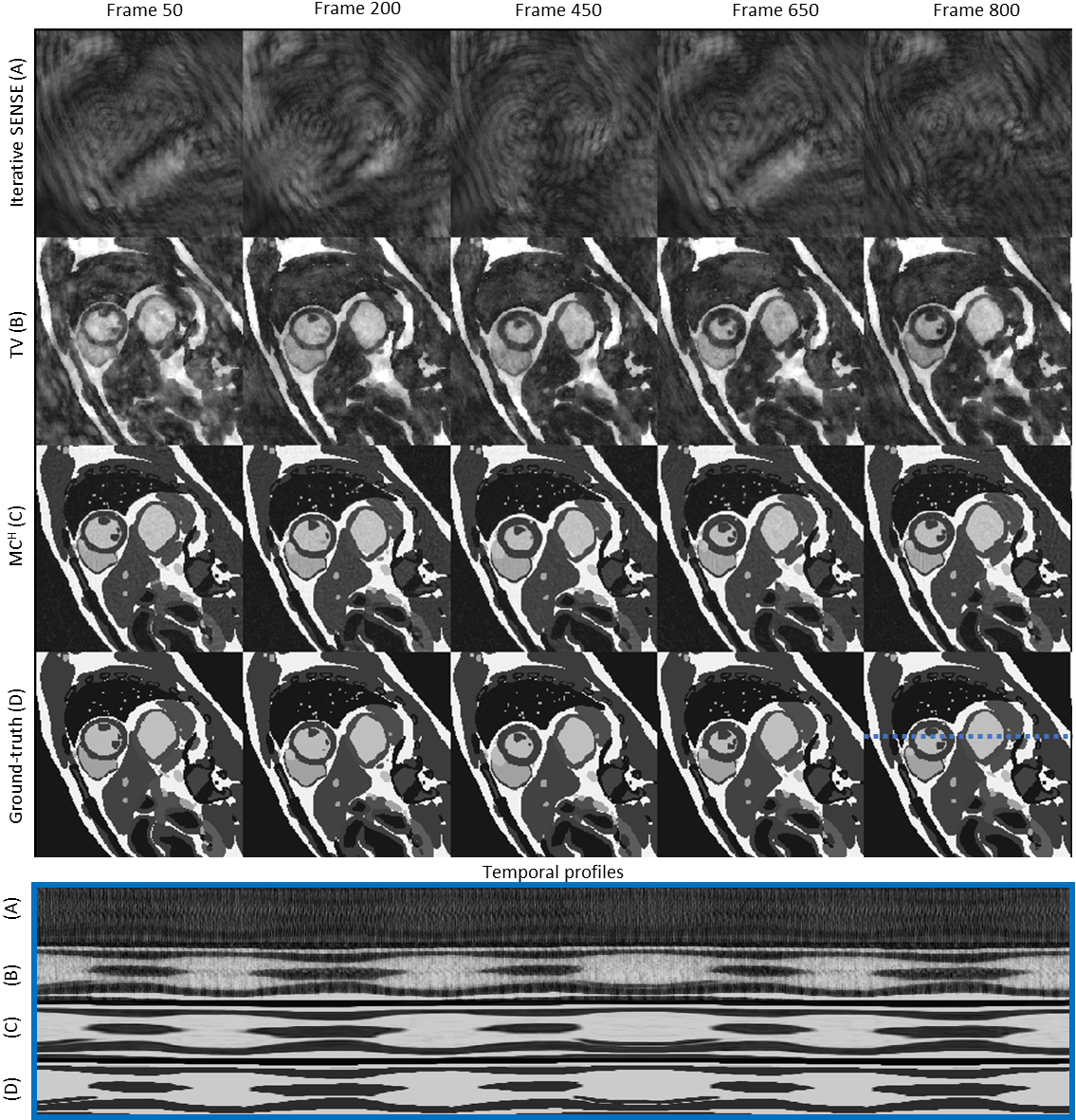
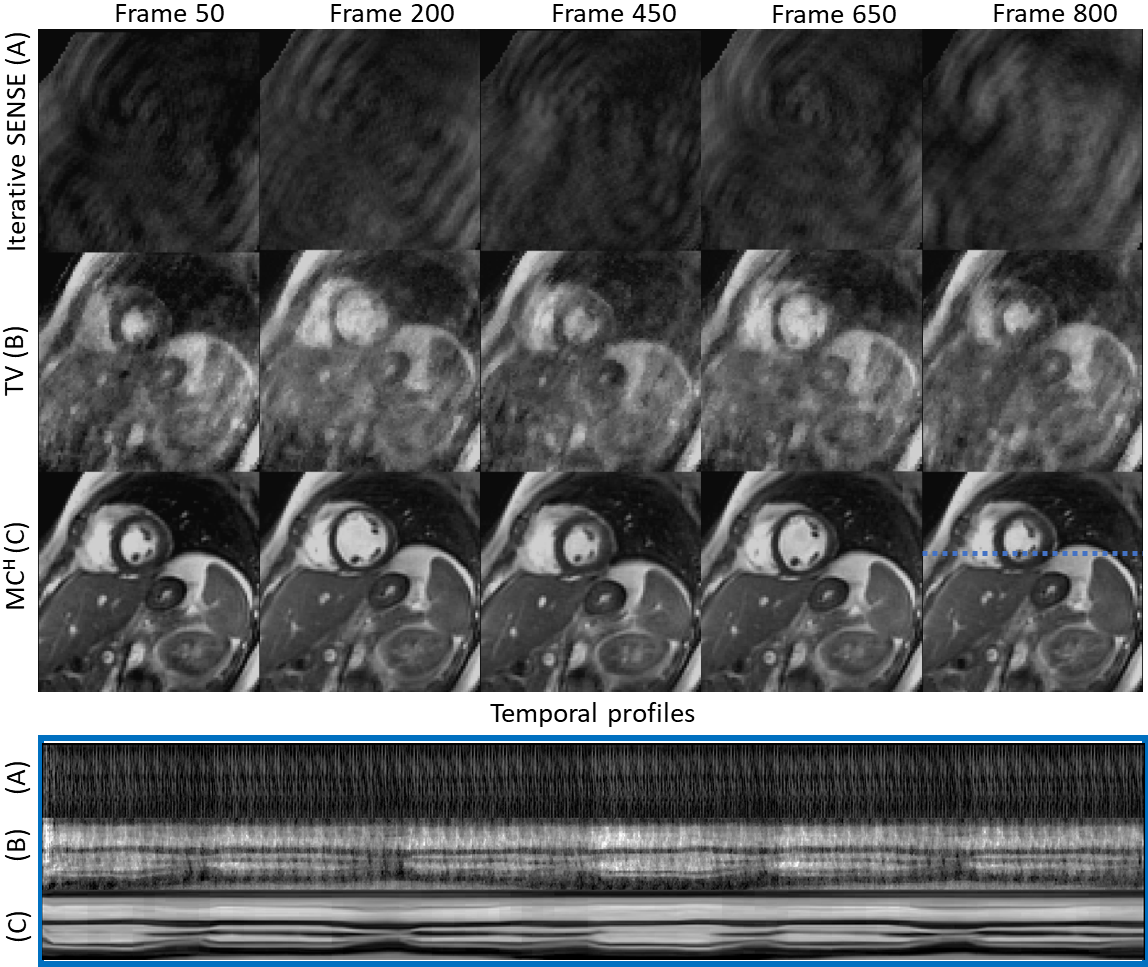
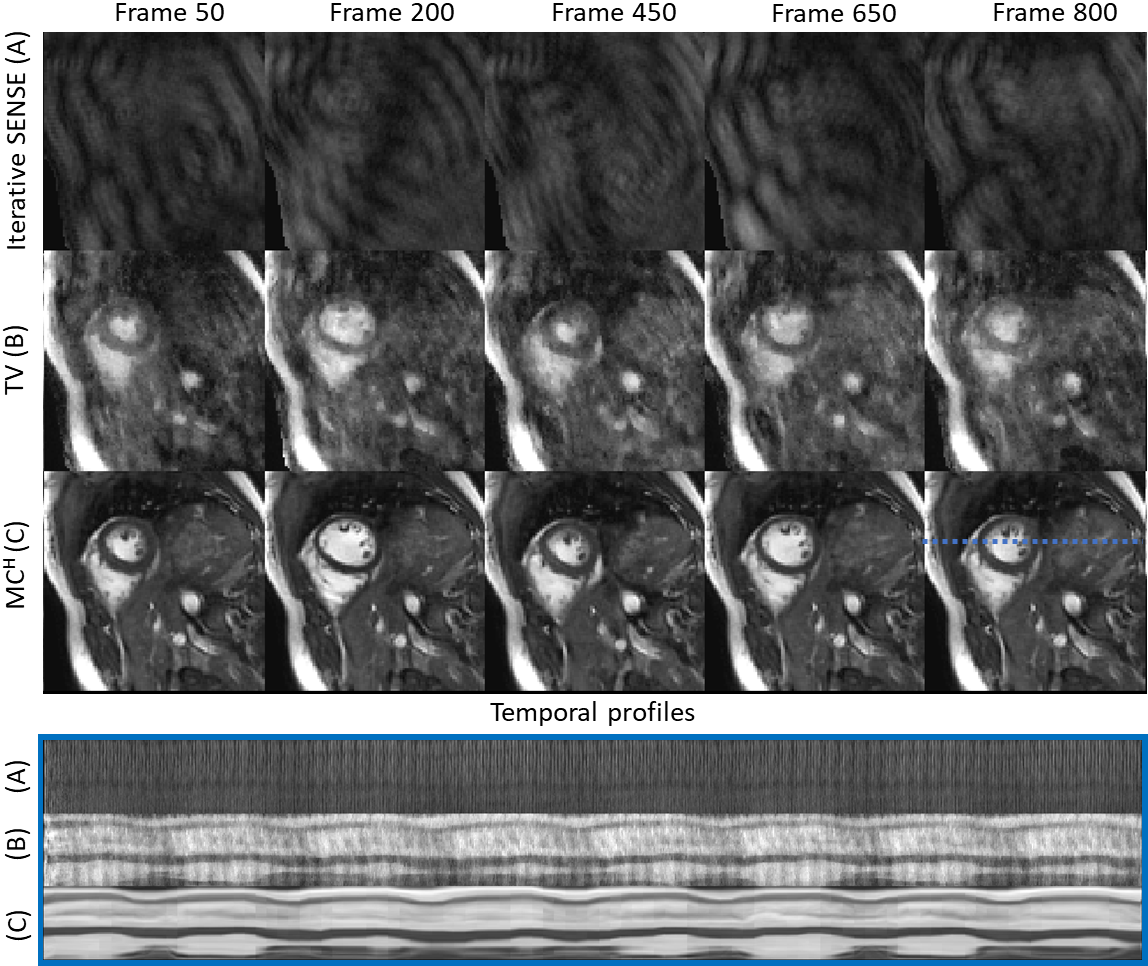
In simulations, aliasing artefacts dominate the SENSE reconstruction (RMSE=16.3E-2); considerable aliasing remains in TV (RMSE=7.0E-2); and only minor residual aliasing remains in MCH (RMSE=2.6E-2) (Fig.2). Different simulated respiratory and cardiac motion states are correctly resolved using both MCH and TV, albeit with more artefacts in the latter; significant aliasing is present with iterative SENSE (Fig.3). Corresponding performance is observed in vivo, with major, considerable and minor residual aliasing observed for SENSE, TV and MCH, respectively (Fig.4). Similar performance can be observed in a second in-vivo case in Fig.5. In both in-vivo cases, 1D temporal profiles indicate that MCH captures real-time motion at high temporal resolution with only minimal aliasing, unlike TV and iterative SENSE.CONCLUSION:
A novel approach combining Hermitian symmetry (via VCC) with motion corrected reconstructions is proposed to enable TR-resolved real-time cardiac MR at 0.55T, outperforming conventional compressed sensing. The high temporal resolution achieved could reveal finer details of cardiac motion in challenging applications such as valve imaging or exercise stress imaging, and may be particularly useful for higher coverage applications (e.g. 3D cine). Continued work will evaluate the performance of MCH in a larger cohort and evaluate beat-to-beat ejection fractions to complement existing functional analysis.Acknowledgements
This work was supported by the NIH (R01 HL153034, R01HL163991, R01HL163030) and Siemens Healthcare.References
1. Pruessmann KP, Weiger M, Börnert P, Boesiger P. Advances in sensitivity encoding with arbitrary k‐space trajectories. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2001 Oct;46(4):638-51.
2. Seiberlich N, Ehses P, Duerk J, Gilkeson R, Griswold M. Improved radial GRAPPA calibration for real‐time free‐breathing cardiac imaging. Magnetic resonance in medicine. 2011 Feb;65(2):492-505.
3. Zhang S, Uecker M, Voit D, Merboldt KD, Frahm J. Real-time cardiovascular magnetic resonance at high temporal resolution: radial FLASH with nonlinear inverse reconstruction. Journal of Cardiovascular Magnetic Resonance. 2010 Dec;12(1):1-7.
4. Pedersen H, Kozerke S, Ringgaard S, Nehrke K, Kim WY. k‐t PCA: temporally constrained k‐t BLAST reconstruction using principal component analysis. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2009 Sep;62(3):706-16.
5. Feng L, Srichai MB, Lim RP, Harrison A, King W, Adluru G, Dibella EV, Sodickson DK, Otazo R, Kim D. Highly accelerated real‐time cardiac cine MRI using k–t SPARSE‐SENSE. Magnetic resonance in medicine. 2013 Jul;70(1):64-74.
6. Zhao B, Haldar JP, Christodoulou AG, Liang ZP. Image reconstruction from highly undersampled (k, t)-space data with joint partial separability and sparsity constraints. IEEE transactions on medical imaging. 2012 Jun 8;31(9):1809-20.
7. Otazo R, Candes E, Sodickson DK. Low‐rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magnetic resonance in medicine. 2015 Mar;73(3):1125-36.
8. Batchelor PG, Atkinson D, Irarrazaval P, Hill DL, Hajnal J, Larkman D. Matrix description of general motion correction applied to multishot images. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2005 Nov;54(5):1273-80.
9. Cruz G, Hammernik K, Kuestner T, Velasco C, Hua A, Ismail TF, Rueckert D, Botnar RM, Prieto C. Single‐heartbeat cardiac cine imaging via jointly regularized nonrigid motion‐corrected reconstruction. NMR in Biomedicine. 2023:e4942.
10. Blaimer M, Gutberlet M, Kellman P, Breuer FA, Köstler H, Griswold MA. Virtual coil concept for improved parallel MRI employing conjugate symmetric signals. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2009 Jan;61(1):93-102.
11. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD‐GRASP: golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. Magnetic resonance in medicine. 2016 Feb;75(2):775-88.
12. Rueckert D, Sonoda LI, Hayes C, Hill DL, Leach MO, Hawkes DJ. Nonrigid registration using free-form deformations: application to breast MR images. IEEE transactions on medical imaging. 1999 Aug;18(8):712-21.
13. Modat M, Ridgway GR, Taylor ZA, Lehmann M, Barnes J, Hawkes DJ, Fox NC, Ourselin S. Fast free-form deformation using graphics processing units. Computer methods and programs in biomedicine. 2010 Jun 1;98(3):278-84.
14. Wissmann L, Santelli C, Segars WP, Kozerke S. MRXCAT: Realistic numerical phantoms for cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance. 2014 Dec;16(1):1-1.
Figures