0744
Unfolding evolving pathology in experimental cerebral malaria model treated with artesunate with in vivo MRI1Radiology, Albert Einstein College of Medicine, Bronx, NY, United States, 2Microbiology & Immunology and Infections Diseases, Albert Einstein College of Medicine, Bronx, NY, United States
Synopsis
Keywords: Infectious Disease, Infectious disease, cerebral malaria
Motivation: Artesunate is the first-line treatment of P. falciparum malaria. However, despite artesunate therapy, there is a 15% fatality rate in severe malaria and survivors can suffer long-term neurocognitive deficits.
Goal(s): Describe the evolving pathology in experimental cerebral malaria (ECM) model treated with artesunate, to develop a model for testing adjunctive therapy in cerebral malaria.
Approach: In vivo MRI was applied on ECM mice prior to and post artesunate treatment.
Results: Despite rapid clearance of the parasite by artesunate, significantly reduced CBF and subsequent reperfusion/reoxygenation injury is detected by MRI, and may ultimately cause neurocognitive deficits in CM survivors.
Impact: It is critical to understand the evolving pathology after antimalarial cure with artesunate in cerebral malaria in order to design effective adjunctive therapy, to reduce mortality and neurocognitive impairment. Reduced CBF and its rapid recovery may contribute to CM neuropathology.
Introduction
Cerebral malaria (CM) is characterized by brain microvasculature sequestration of P. falciparum parasites, inflammatory cytokine production and vascular leakage. Antimalaria drug Artesunate (ART) is the first-line treatment of severe P. falciparum malaria. However mortality rate is high and survivors can suffer long-term neurocognitive deficits1 despite its potent antimalaria effect. Thus, defining the possible mechanisms of long-term neurocognitive impairment in CM treated with artesunate is critical to developing adjunctive neuroprotective therapies. Here experimental cerebral malaria (ECM) mouse model was used to monitor the effect of infection and recovery post artesunate. We hypothesized that reduction in cerebral blood flow (CBF) due to the obstruction of vessels by infected and uninfected RBCs, and subsequent reperfusion/reoxygenation may contribute to the neurological complication in survivors of CM.Methods
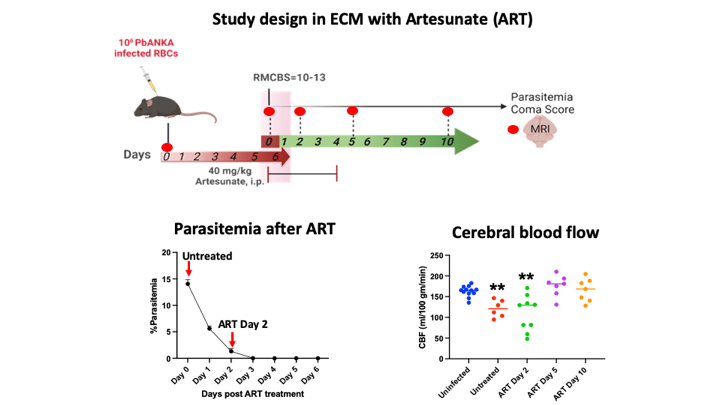
C57BL/6 mice were infected with PbANKA infected RBCs and treated with artesunate after onset of neurological decline in ECM (untreated ECM), as shown in Figure 1. Neuropathology was assessed using volumetrics, CBF, T1, T2* (3D-MGRE), and tissue inflammation (DTI mean diffusivity, MD) at 9.4 Tesla2. ANTs3 was used to register Dorr mouse brain atlas4 to T2-wt images for atlas-based volumetric analysis and extraction of T2* and diffusivity. CBF and T1 were manually analyzed.Results
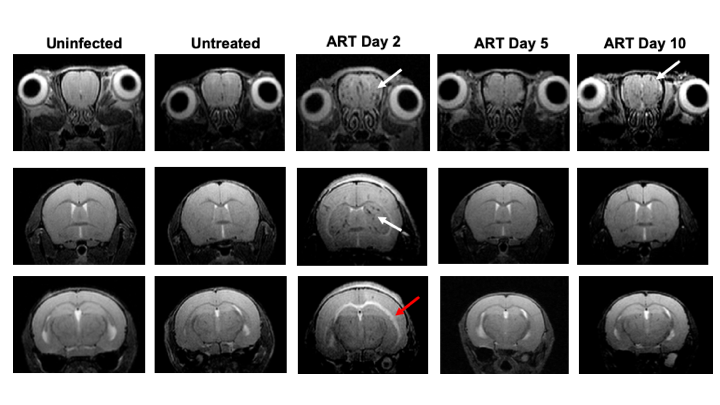
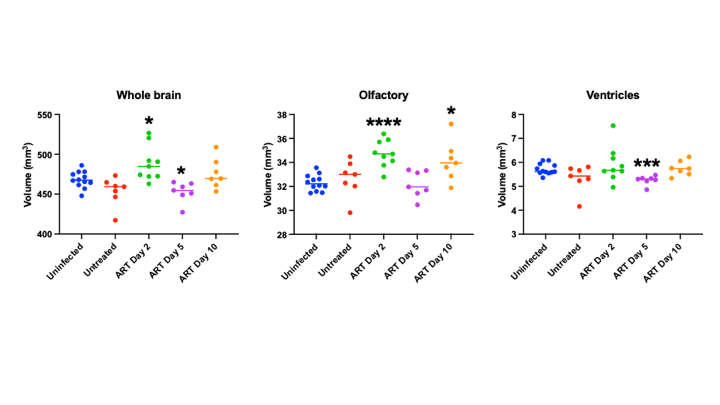
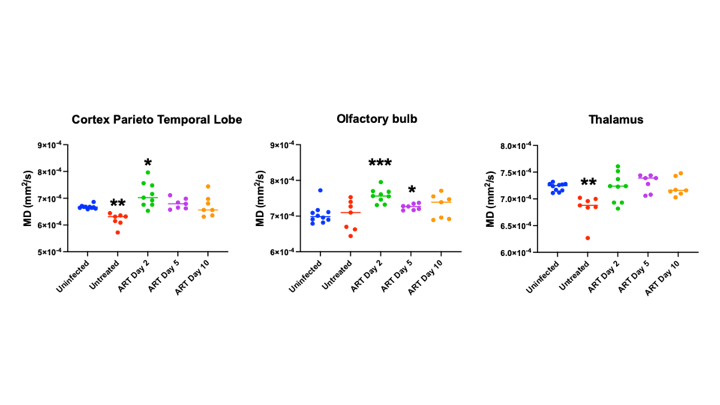
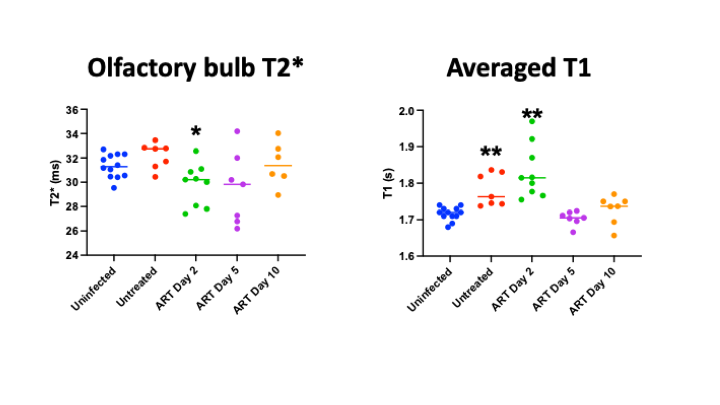
As expected, parasitemia (Figure 1) decreased from 14.1% in untreated mice to 1.3% in ART treated Day 2 mice, and no parasites were detected by day 4 of ART. CBF (Figure 1) decreased significantly from the uninfected control of 163±13 to untreated ECM 110±43 ml/100 gm/min and remained decreased at Day 2 ART with 121±21 ml/100 gm/min. CBF in both Day 5 and Day 10 ART mice recovered to normal level. As demonstrated in Figure 2, no obvious pathology was detected in brain of untreated ECM mice. However, in Day 2 ART mice, microhemorrhages was observed in olfactory, cortex, and thalamus. White matter hyperintensity was also observed. In Day 5 ART mice, microhemorrhages was less severe compared to ART Day 2 mice. Furthermore, microhemorrhages persist in Day 5 and Day 10 ART mice even when parasitemia is undetectable. Volumetric analysis (Figure 3) demonstrates enlarged brain only in Day 2 ART mice, that was reflected in both grey and white matter, but not in ventricles. Brain volume in Day 5 ART mice was slightly smaller when compared to uninfected mice. MD (Figure 4) decreased in untreated ECM mice, but increased in Day 2 ART mice compared to uninfected mice. MD eventually recovered to uninfected level in most brain regions. T2* decreased in olfactory of Day 2 ART mice, as shown in Figure 5. Averaged T1 (Figure 5) increased in both Untreated and Day 2 ART mice. Increased T1, T2*, and MD in ART Day 2 mice indicate an increase in extracellular fluid, which accumulates during vasogenic edema formation.Discussion
Our study provides a temporal analysis post cure of malaria in the ECM model and demonstrates that neuropathology is maximal after the start of artesunate treatment, and highlights the role of abnormal CBF. Parasitized erythrocytes obstruct brain vessels leading to significantly reduced CBF in infected mice where no obvious pathology was detected by neuroimaging. Reduced CBF persists in Day 2 ART mice when parasitemia was significantly reduced by artenusate, along with worsening pathology. In untreated ECM and Day 2 ART mice, ~30% drop of CBF causes a critical reduction in the supply of oxygen and glucose to the brain, which may contribute to severe pathology including microhemorrhages and white matter hyperintensities that develop over time. Increased MD and T1 suggests that vasogenic edema contributes to brain swelling in Day 2 ART mice. Despite normalization of CBF and edema reversal at day 5 ART, the rapid reperfusion and reoxygenation may lead to ongoing microhemorrhages, which is also reported in survivors of CM5. This implies that the impediment of parasite induced vascular damage during acute disease, may contribute to long-term neurocognitive impairment despite ART’s robust antiparasitic effect. Altogether, our study provides evidence that microvascular alterations occur after resolution of blood flow and edema abnormalities in ECM treated with ART despite its potent action in eliminating circulating parasites. This indicates that adjunct treatment targeting reducing reperfusion injury and protecting vascular integrity may improve the outcomes of specific neuro- and vasculo-protective effects.Conclusion
Delayed occurrence of microhemorrhages and neurocognitive deficit reported in survivors of CM treated with ART makes it critically important to understand the evolving pathology during the early stages of recover post ART treatment. Our data indicate that significantly reduced blood flow and subsequently recovery might have long-term damaging effect on cerebral vascular integrity.Acknowledgements
No acknowledgement found.References
1. Idro R, Jenkins NE, Newton CR. Pathogenesis, clinical features, and neurological outcome of cerebral malaria. Lancet Neurol. 2005;4(12):827-840.
2.Cui MH, Billett HH, Suzuka SM, et al. Corrected cerebral blood flow and reduced cerebral inflammation in berk sickle mice with higher fetal hemoglobin. Transl Res. 2022;244:75-87.
3. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. 2011;54(3):2033-2044.
4. Dorr AE, Lerch JP, Spring S, Kabani N, Henkelman RM. High resolution three-dimensional brain atlas using an average magnetic resonance image of 40 adult C57Bl/6J mice. Neuroimage. 2008;42(1):60-69.
5.Nickerson JP, Tong KA, Raghavan R. Imaging cerebral malaria with a susceptibility-weighted MR sequence. AJNR Am J Neuroradiol. 2009;30(6):e85-86.
Figures