0736
Unsupervised PK Model-free BBB Leakage Detection in DCE-MRI using Generative Adversarial Networks1Department of Biomedical Sciences, Seoul National University College of Medicine, Jongno-gu, Korea, Republic of, 2Interdisciplinary Program in Cancer Biology, Seoul National University College of Medicine, Jongno-gu, Korea, Republic of, 3Department of Radiology, Seoul National University Hospital, Jongno-gu, Korea, Republic of, 4Artificial Intelligence Collaborative Network (AICON), Department of Radiology, Seoul National University Hospital, Jongno-gu, Korea, Republic of, 5Department of Radiology, Seoul National University College of Medicine, Jongno-gu, Korea, Republic of, 6Center for Nanoparticle Research, Institute for Basic Science (IBS), Gwanak-gu, Korea, Republic of, 7Department of Radiology, Seoul Metropolitan Goverment-Seoul National University Boramae Medical Center, Seoul, Korea, Republic of, 8Department of Medical Sciences, Seoul National University College of Medicine, Jongno-gu, Korea, Republic of
Synopsis
Keywords: Diagnosis/Prediction, Perfusion, DCE-MRI, Glioblastoma, Blood-brain barrier, Deep learning, Generative adversarial networks
Motivation: Arterial input function (AIF) in DCE-MRI is often degraded due to noise, motion, and partial volume. This may lower the overall reliability of the resulting pharmacokinetic (PK) parameters.
Goal(s): Our goal was to develop a robust, fast method for detecting blood-brain barrier (BBB) leakage signals without PK models.
Approach: We employed a fast anomaly detection using generative adversarial networks (f-AnoGAN) for unsupervised detection of the leakage signals.
Results: The results were highly correlated with the traditional Ktrans maps, and more robust against reduced temporal data points, which may be used for shorter scan time and/or higher spatial resolution.
Impact: Our proposed method may allow fast and robust detection of BBB leakage signals in the case where the scan time is highly limited, and consequently, the traditional approach with PK models may not be suitable.
Introduction
The estimation of the arterial input function (AIF)1 in DCE-MRI can be time-consuming and susceptible to noise, motion, and partial volume artifacts, potentially leading to errors in PK parameter estimation2-5. While recent studies have presented blood-brain barrier (BBB) leakage imaging using DCE-MRI, there are many challenges in obtaining precise PK parameters and in dealing with the wide diversity of abnormal contrast leakage signals6. In this study, we investigate the feasibility of employing f-AnoGAN7 for the unsupervised detection of unseen BBB leakage signals in DCE-MRI using deep learning without PK models.Method
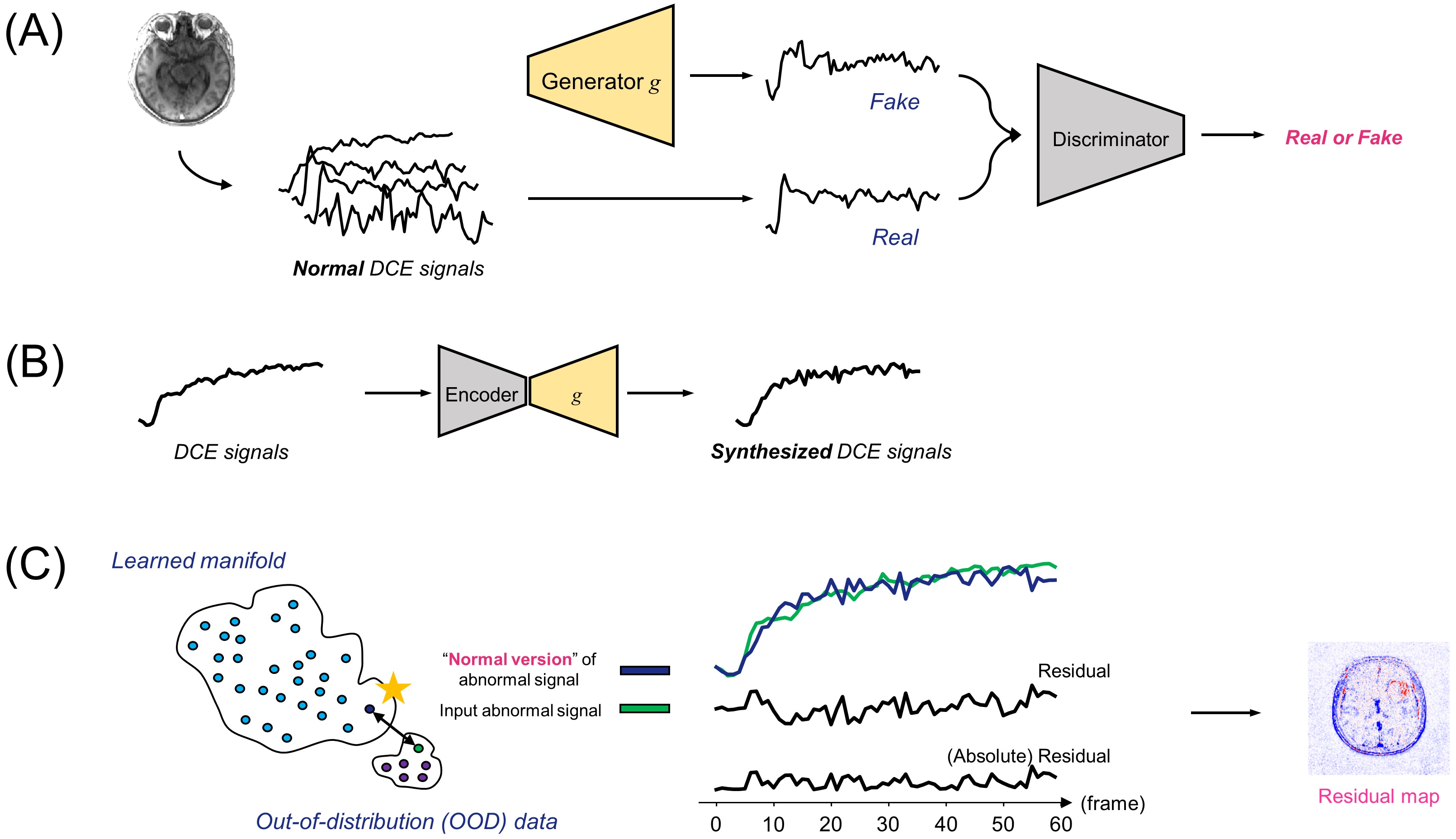
DCE-MRI data: In this study, we conducted DCE-MRI scans using a Siemens scanner on 30 adult-type diffuse glioma (glioblastoma, IDH-wt; astrocytoma, IDH-mutant; oligodendroglioma, IDH-mutant, and 1p/19q-codeleted, according to WHO CNS tumor classification 2021) patients with institutional review board approval and informed consent. The choice of glioma as our subject was motivated by its suitability for studying BBB breakdown and contrast leakage8, which result from glioma cell infiltration. Out of the 30 patients, data from 20 patients were allocated for a training set, and the remaining 10 were used for a test set.f-AnoGAN: We employed an AnoGAN9 to detect unseen abnormalities within the input data based on a reference data obtained from AnoGAN (Fig.1). The AnoGAN was trained solely on 543,740 normal DCE-MRI 1D time-series signals, with exclusion of axial slices containing tumors. For fast latent space mapping, we employed a f-AnoGAN7 approach, incorporating an autoencoder10, of which the decoder part is the generator of the pre-trained GAN.
Unsupervised leakage detection: If a given query signal is abnormal, then the network cannot produce abnormal data because it has never seen it during training. Instead, it aims to produce a normal DCE signal that closely resembles the input signal but without abnormality. The abnormality of the DCE signal can directly be visualized by the residual signal between the query and the AnoGAN-generated signal. The proposed leakage maps can be obtained by estimating the residual signals for all image pixels (Fig.1).
Network evaluation: Ktrans maps were obtained using nordicICE (NordicNeuroLab, Norway) using an extended Tofts model11-12 for comparison. We calculated the structural similarity index13 (SSIM) between our proposed maps and the Ktrans maps, as well as the Pearson’s correlation coefficient (r) between the residuals and Ktrans values for comparative analysis.
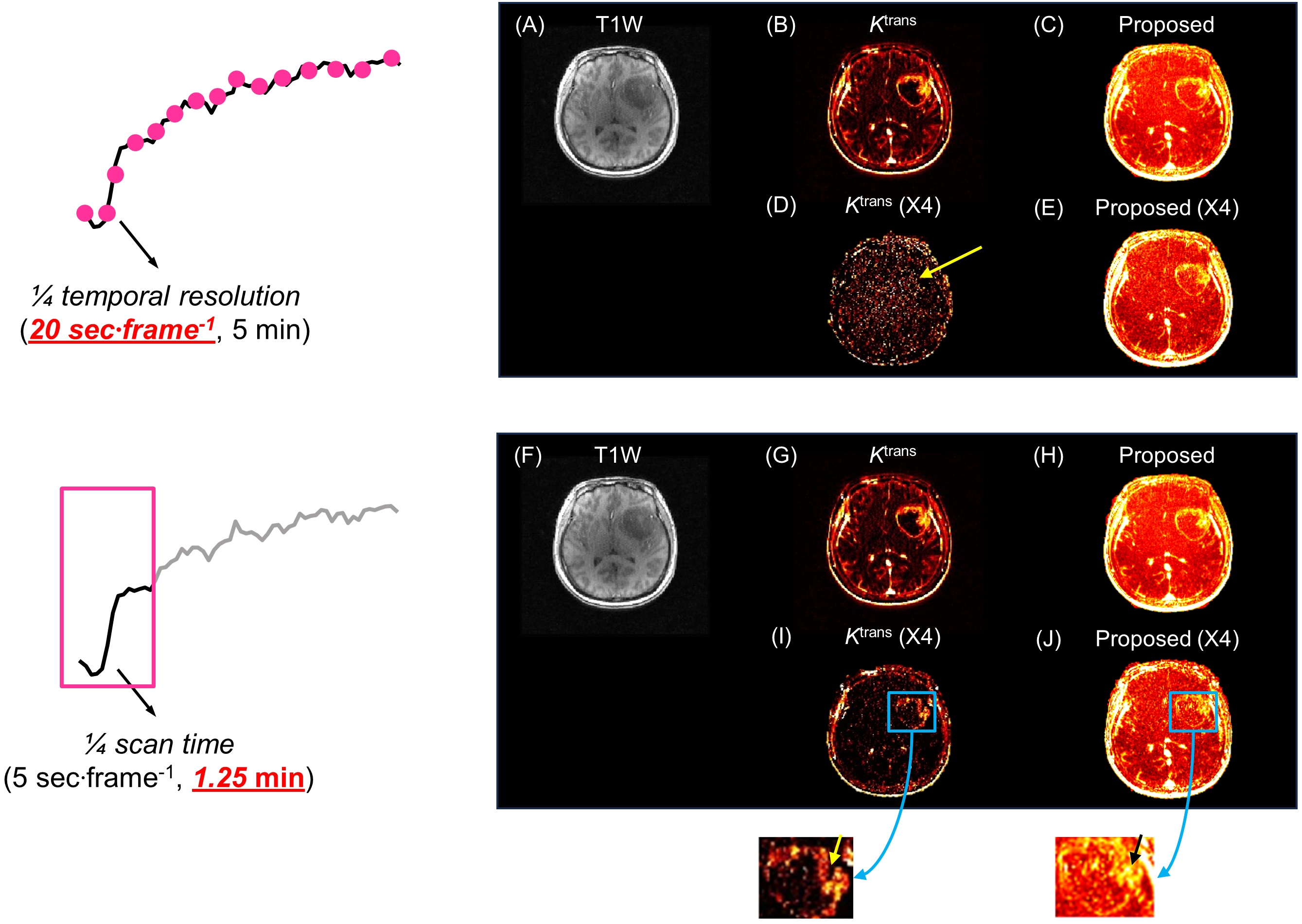
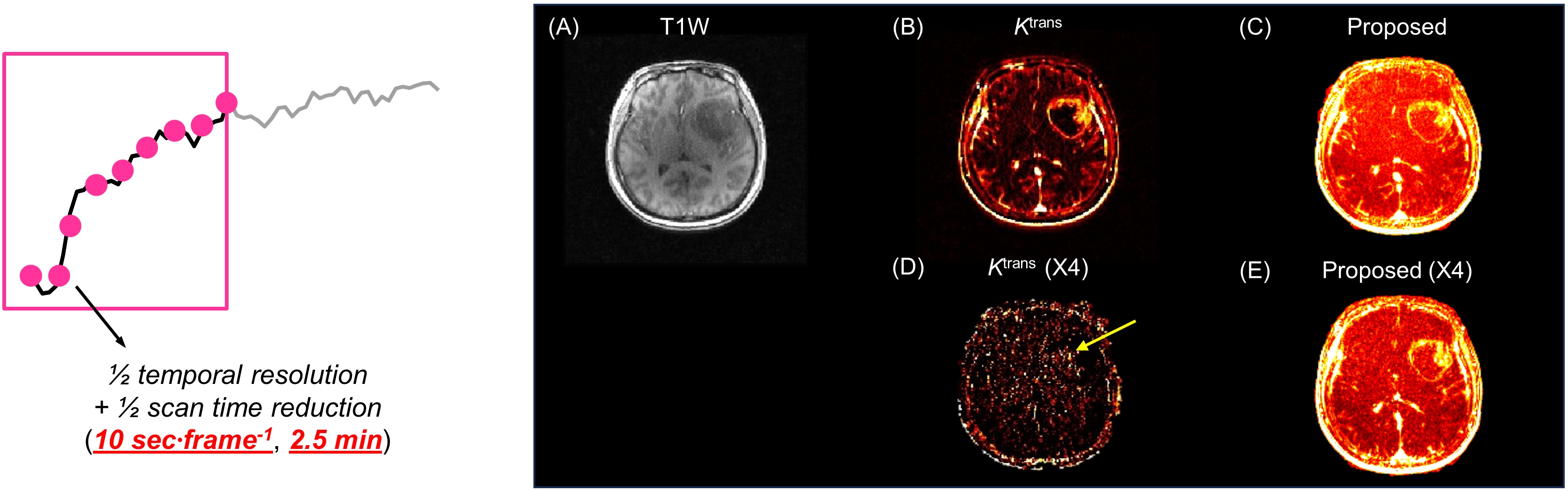
Ablation experiments: Additionally, we explored the feasibility of our proposed network by comparing it to a traditional model-fitting approach using additional retrospective datasets. For each unique retrospective training dataset, a dedicated f-AnoGAN model was independently trained and subsequently evaluated on the corresponding modified test dataset. First, DCE-MRI of which the temporal resolution was reduced by 4x, were tested, which can improve spatial resolution. Second, data with reduced scan time by a factor of 4 were used. Finally, we utilized hybrid data, where the temporal resolution was reduced by 2x, and scan time was also reduced by 2x.
Results
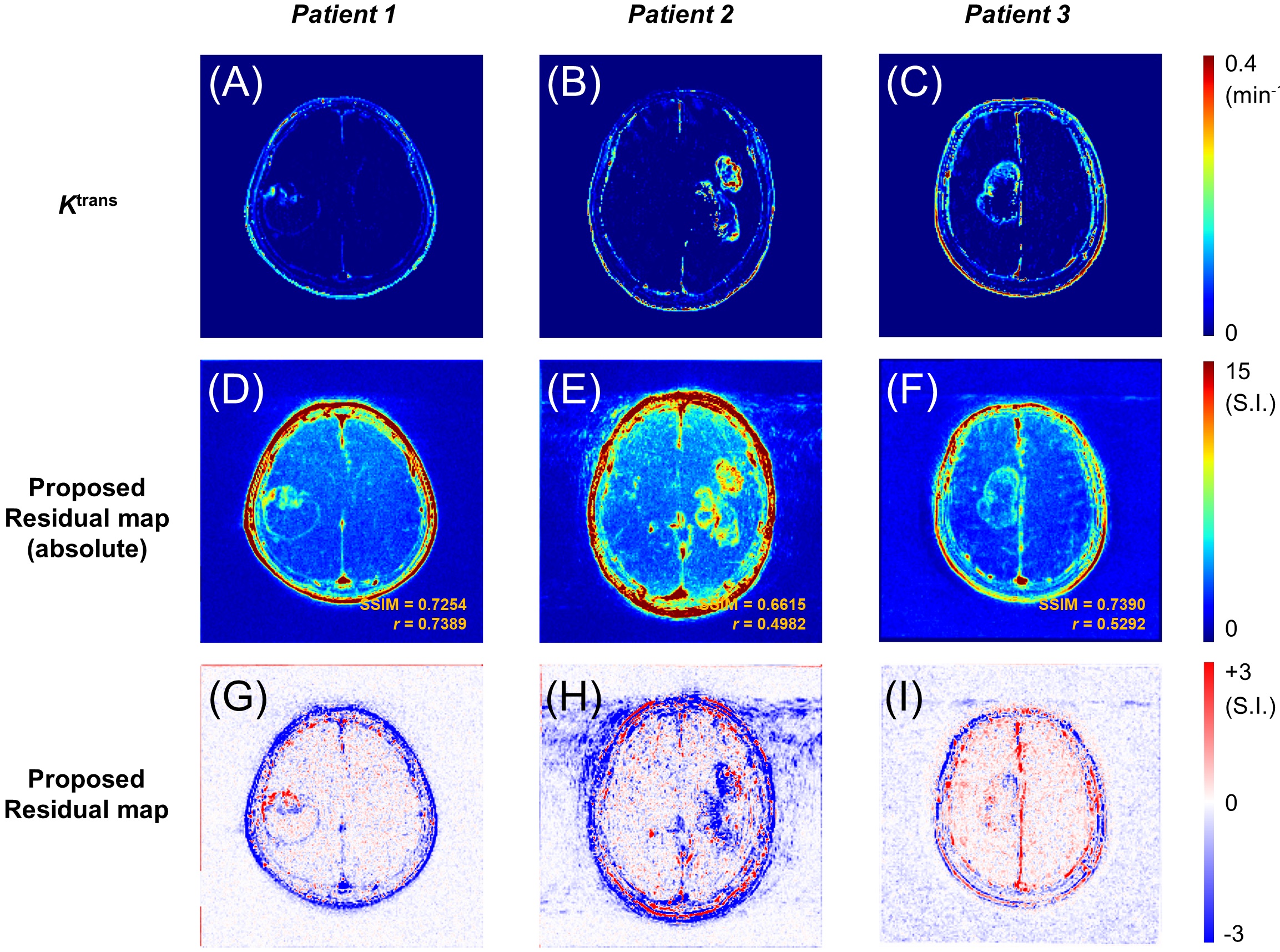
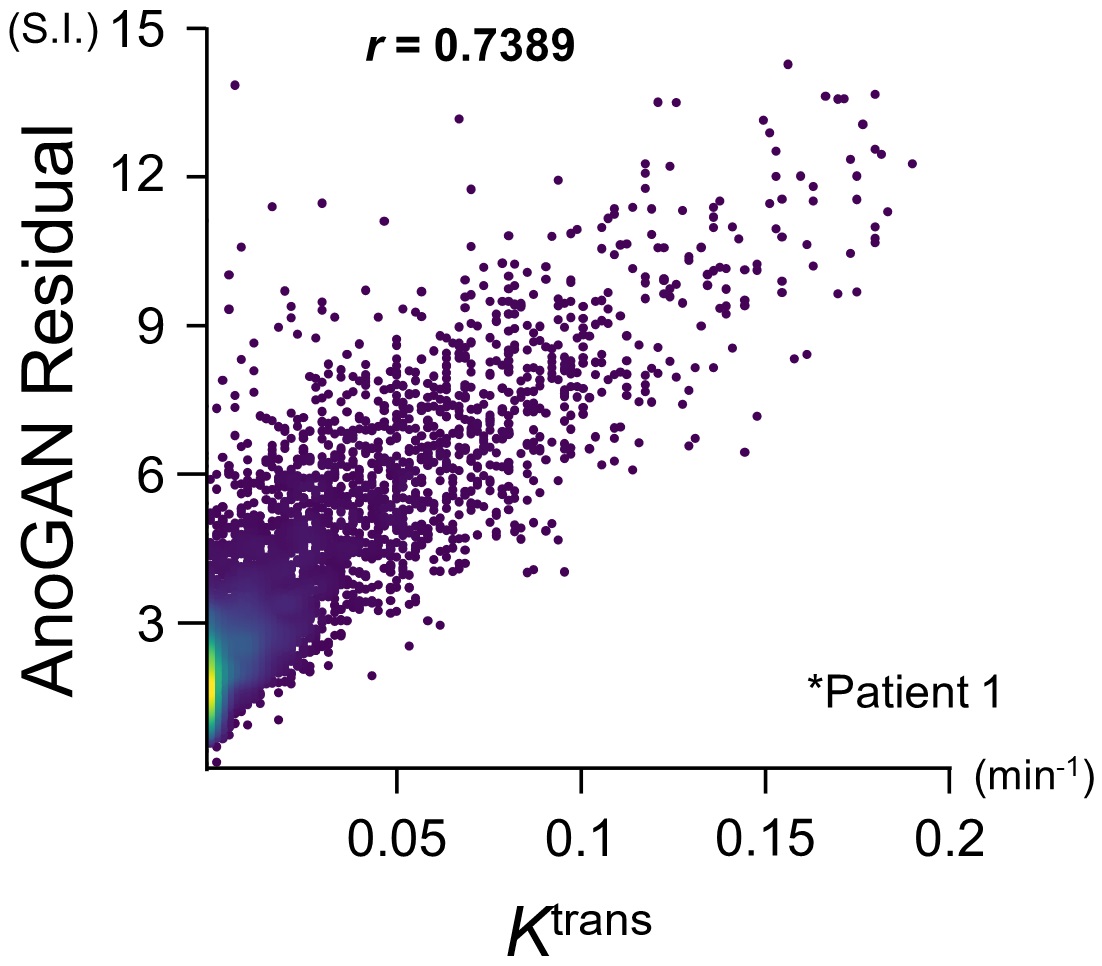
Leakage detection: Fig.2A-C show Ktrans maps of representative patient data. The corresponding residual maps in absolute mode (Fig.2D-F) and original residual maps (Fig.2G-I) obtained by the proposed method appear to be comparable with Ktrans maps. Fig.3 shows the representative scatter plot, in which the AnoGAN residuals are highly correlated with Ktrans values. The mean SSIM was 0.7285±0.0539 and the mean r was 0.6265±0.0826. Each slice was processed in 0.1 millisecond with a single GPU.Ablation experiments: The anatomical image, Ktrans and proposed leakage map from the original data are shown (Fig.4A-C, Fig.4F-H, Fig.5A-C). Fig.4D-E show the results of each method with the reduced temporal resolution. Fig.4I-J show the results for the data with the reduced scan time. The results of the hybrid data with the reduced temporal resolution and scan time are also shown in Fig.5D-E. Overall, the Ktrans maps tend to be degraded, but the proposed residual maps remain relatively robust.
Discussion
The proposed method shows high SSIM and, specifically, high r with Ktrans (Fig.3), which implies that it is capable of detecting unseen BBB breakdown without PK models. Moreover, the proposed method may be more robust than Ktrans to the limited amount of data. Thus, the proposed method may have potential in DCE-MRI. However, more training data are needed for more accurate manifold learning, and the latent space mapping needs to be further improved for more accurate synthesized data. Importantly, we need to validate the method on a more amount of patient data.Conclusion
Deep learning-based leakage detection without PK models and ground truth data may be feasible. Additionally, the proposed method has potential for higher spatial resolution and/or reduced scan time in DCE-MRI.Acknowledgements
This research was supported by grant No. 0420212190 from the SNUH Research Fund, and supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (No. 2021M3E5D2A01022493)(I.H). Phase III (Postdoctoral fellowship) grant of the SPST (SNU-SNUH Physician Scientist Training) Program (K.S.C), the National Research Foundation of Korea (NRF) grant fundedby the Korea government (MSIT) (No. RS-2023-00251022) (K.S.C); the SNUH Research Fund (No. 04-2022-0520) (K.S.C.); the Technology Innovation Program (20011878, Development of Diagnostic Medical Devices with Artificial Intelligence Based Image Analysis Technology) funded by the Ministry of Trade, Industry & Energy (MOTIE, Korea) (J.W.C).
We would like to thank Hyeryeon Son, Hye Mi Bang, and Minsu Kim for their invaluable assistance with data collection and analysis.
References
1. Sourbron SP, Buckley DL. On the scope and interpretation of the Tofts models for DCE-MRI. Magn Reson Med. 2011;66(3):735-745. doi:10.1002/mrm.22861
2. Heye T, Davenport MS, Horvath JJ, et al. Reproducibility of Dynamic Contrast-enhanced MR Imaging. Part I. Perfusion Characteristics in the Female Pelvis by Using Multiple Computer-aided Diagnosis Perfusion Analysis Solutions. Radiology. 2013;266(3):801-811. doi:10.1148/radiol.12120278
3. Rata M, Collins DJ, Darcy J, et al. Assessment of repeatability and treatment response in early phase clinical trials using DCE-MRI: comparison of parametric analysis using MR- and CT-derived arterial input functions. Eur Radiol. 2016;26(7):1991-1998. doi:10.1007/s00330-015-4012-9
4. Port RE, Knopp MV, Brix G. Dynamic contrast-enhanced MRI using Gd-DTPA: Interindividual variability of the arterial input function and consequences for the assessment of kinetics in tumors. Magn Reson Med. 2001;45(6):1030-1038. doi:10.1002/mrm.1137
5. Sourbron S. Technical aspects of MR perfusion. Eur J Radiol. 2010;76(3):304-313. doi:10.1016/j.ejrad.2010.02.017
6. Montagne A, Barnes SR, Nation DA, Kisler K, Toga AW, Zlokovic BV. Imaging subtle leaks in the blood–brain barrier in the aging human brain: potential pitfalls, challenges, and possible solutions. Geroscience. 2022;44(3):1339-1351. doi:10.1007/s11357-022-00571-x
7. Schlegl T, Seeböck P, Waldstein SM, Langs G, Schmidt-Erfurth U. f-AnoGAN: Fast unsupervised anomaly detection with generative adversarial networks. Méd Image Anal. 2019;54:30-44. doi:10.1016/j.media.2019.01.010
8. Heye AK, Culling RD, Hernández M del CV, Thrippleton MJ, Wardlaw JM. Assessment of blood–brain barrier disruption using dynamic contrast-enhanced MRI. A systematic review. NeuroImage: Clin. 2014;6:262-274. doi:10.1016/j.nicl.2014.09.002
9. Schlegl T, Seeböck P, Waldstein SM, Schmidt-Erfurth U, Langs G. Unsupervised Anomaly Detection with Generative Adversarial Networks to Guide Marker Discovery. arXiv. 2017. doi:10.48550/arxiv.1703.05921
10. Hinton GE, Salakhutdinov RR. Reducing the Dimensionality of Data with Neural Networks. Science. 2006;313(5786):504-507. doi:10.1126/science.1127647
11. Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced t1-weighted MRI of a diffusable tracer: Standardized quantities and symbols. J Magn Reson Imaging. 1999;10(3):223-232. doi:10.1002/(sici)1522-2586(199909)10:3<223::aid-jmri2>3.0.co;2-s
12. Tofts PS. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J Magn Reson Imaging. 1997;7(1):91-101. doi:10.1002/jmri.1880070113
13. Wang Z, Bovik AC, Sheikh HR, Simoncelli EP. Image Quality Assessment: From Error Visibility to Structural Similarity. IEEE Trans Image Process. 2004;13(4):600-612. doi:10.1109/tip.2003.819861
Figures