0730
Water exchange across blood-brain barrier in neuromyelitis optica spectrum disorder measured by vascular-water-exchange MRI1Key Laboratory of Biomedical Engineering of Education Ministry, College of Biomedical Engineering and Instrument Science, Zhejiang University, Hangzhou, China, 2Neurology Department, First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China, 3MR Collaboration, Siemens Healthcare, Shanghai, China, 4Interdisciplinary Institute of Neuroscience and Technology, Zhejiang University School of Medicine, Hangzhou, China
Synopsis
Keywords: Neuroinflammation, Neuroinflammation, blood-brain barrier, vascular-water-exchange imaging, neuromyelitis optica spectrum disorder
Motivation: Limited information exists regarding the spatial characteristics of blood-brain barrier (BBB) disruption at the whole-brain level for neuromyelitis optica spectrum disorder (NMOSD).
Goal(s): We explored spatial features of BBB changes in NMOSD using noninvasive, quantitative MRI technique.
Approach: Vascular-water-exchange MRI was applied for quantitative analysis.
Results: In the white matter, the apparent exchange rate across the BBB (AXRBBB) was significantly higher in acute-phase patients than in healthy controls, especially in some lesion-prone areas. In the gray matter, acute-phase patients had significantly higher AXRBBB values in the frontal and parietal lobes. AXRBBB was also significantly correlated with clinical-scale scores.
Impact: Exploring the spatial features of BBB disruption will enable better understanding the imaging features of NMOSD and may help clinicians in differentially diagnosing NMOSD from other brain diseases using noninvasive MRI.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a demyelinating inflammatory syndrome of the central nervous system that mainly affects the optic nerve and/or spinal cord. In most cases, NMOSD is characterized by the presence of serum aquaporin-4-immunoglobulin-G (AQP4-lgG)1 antibodies, which are major autoimmune antibodies implicated in the NMOSD pathogenesis2. BBB disruption has been reported in NMOSD3–5 and the BBB permeability could also serve as a biomarker for predicting NMOSD severity6. However, current evaluations of BBB permeability in NMOSD rely primarily on invasive techniques such as the albumin-index, which requires blood and cerebrospinal fluid samples from patients and cannot provide spatial characteristics of the BBB disruption. Vascular water exchange imaging (VEXI), a special version of filter exchange imaging (FEXI) adapted for the measurement of BBB permeability to water molecules, is a contrast-agent-free MRI method for BBB assessment7,8. In this study, we aim to explore the spatial characteristics of BBB permeability on a whole-brain scale for NMOSD by using VEXI.Methods
ParticipantsEleven acute-phase and 12 recovery-phase NMOSD patients and 12 healthy controls (HCs) were recruited.
MRI data acquisition and processing
VEXI is a specialized diffusion-based technique designed to assess the exchange of water across the BBB. More information on the acquisition and analysis of VEXI data can be found in references7,8. The quantitative parameter used to characterize BBB permeability to water molecules is referred to as the apparent exchange rate across BBB (AXRBBB).
Each participant was examined on a 3T MRI clinical scanner (MAGNETOM Prisma, Siemens Healthcare). VEXI with a 3.0×3.0×5.0 mm3 resolution was acquired with bf = 250 s/mm2 in the filter block and bd = 0 s/mm2 and 250 s/mm2 with 3 and 6 repetitions, respectively, in the detection block. The three mixing times were 25, 200, and 400 ms. VEXI was also acquired with bf = 0 s/mm2 at the shortest mixing time. VEXI data were preprocessed with TORTOISE9 for eddy current and head motion corrections. In-house programs developed in MATLAB 2018B were used to fit the VEXI data models and obtain the parameter maps (i.e., AXRBBB, apparent diffusion coefficient and σ).
Region-of-interest analysis
For the white matter (WM), we selected multiple lesion areas in NMOSD patients, including the corticospinal tract (CST), corpus callosum (CC), and superior occipitofrontal fascicle (SFOF) as experimental regions, acoustic radiation and uncinate fascicle as control regions. For the gray matter (GM), we selected the thalamus and the frontal, parietal, occipital, temporal and insular lobes. All regions-of-interest were bilateral, and the effect of the cerebrospinal fluid was removed.
Results and Discussion
Firstly, we investigated the differences in BBB permeability between the entire WM and GM (Figure 1d). We found that both in the WM and GM, the AXRBBB values of acute-phase patients were significantly higher than recovery-phase patients (WM, p=0.0278; GM, p=0.0066) and HCs (WM, p=0.0022, GM, p=0.0007). These findings suggested the presence of BBB disruption of acute-phase NMOSD patients.For the detailed WM regions, AXRBBB values were significantly higher for the acute-phase patients than for the HCs (CST, p=0.0269; CC, p=0.0116; SFOF, p=0.0096; Figure 2). The two control regions did not significantly differ. Longitudinally extensive CC lesions and long CST lesions are the most specific lesions in NMOSD2,10,11. One study suggested that the SFOF may be involved in processing visuospatial information12 and that patients with NMOSD have impaired visuospatial processing ability.
For the detailed GM regions, only the frontal and parietal lobes showed significantly higher AXRBBB values in the HCs than in acute-phase patients (p=0.0114 vs. p=0.0285, respectively; Figure 3). This is consistent with previous findings that in bilateral cortical impairment in NMOSD patients, the frontal lobe was the most commonly affected area, followed by the parietal lobe13.
The AXRBBB in both the WM and GM was significantly correlated with Expanded Disability Status Scale scores (WM: r=0.43, p=0.039; GM: r=0.42, p=0.049), suggesting that deeper degrees of NMOSD and worsened motor function are associated with higher AXRBBB values (Figure 4). NMOSD progression is often accompanied by demyelination; thus, we also considered the neurofilament light chain, which is an important biomarker of axonal injury, and we found that it was significantly correlated with both the WM and GM (WM: r=0.55, p=0.049; GM: r=0.65, p=0.016; Figure 5). These results suggest the feasibility of AXRBBB as a useful imaging marker for monitoring NMOSD severity.
Conclusion
We used VEXI to investigate the BBB changes in patients with NMOSD and found the BBB alternations mainly happens in the acute phase of NMOSD and in specific brain regions. Such BBB alternations is correlated with the EDSS score and neurofilament light chain concentration in NMOSD.Acknowledgements
This work is supported in part by the National Natural Science Foundation of China (NSFC) (Grant Nos. 82111530201, 82222032, 82172050), the STI2030-Major Projects Q22 of China (Grant No. 2022ZD0206000).References
1. Borisow N, Mori M, Kuwabara S, et al. Diagnosis and treatment of NMO spectrum disorder and MOG-encephalomyelitis. Front. Neurol., 2018, 9(OCT): 1–15.
2. Wingerchuk D M, Banwell B, Bennett J L, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology, 2015, 85(2): 177–189.
3. Asgari N, Flanagan E P, Fujihara K, et al. Disruption of the leptomeningeal blood barrier in neuromyelitis optica spectrum disorder. Neurol. Neuroimmunol. NeuroInflammation, 2017, 4(4).
4. You X, Yan L, Li X, et al. Disruption of blood-brain barrier integrity associated with brain lesions in Chinese neuromyelitis optica spectrum disorder patients. Mult. Scler. Relat. Disord., 2019, 27(October 2018): 254–259.
5. Jasiak-Zatońska M, Pietrzak A, Wyciszkiewicz A, et al. Different blood-brain-barrier disruption profiles in multiple sclerosis, neuromyelitis optica spectrum disorders, and neuropsychiatric systemic lupus erythematosus. Neurol. Neurochir. Pol., 2022, 56(3): 246–255.
6. Wang Y, Zhu M, Liu C, et al. Blood brain barrier permeability could be a biomarker to predict severity of neuromyelitis optica spectrum disorders: A retrospective analysis. Front. Neurol., 2018, 9(AUG): 1–7.
7. Bai R, Li Z, Sun C, et al. Feasibility of filter-exchange imaging (FEXI) in measuring different exchange processes in human brain. Neuroimage, Elsevier Ltd, 2020, 219(February): 117039.
8. Zhang Y, Wang Y, Li Z, et al. Vascular-water-exchange MRI (VEXI) enables the detection of subtle AXR alterations in Alzheimer’s disease without MRI contrast agent, which may relate to BBB integrity. Neuroimage, Elsevier Inc., 2023, 270(February): 119951.
9. Pierpaoli, C., Walker, L., Irfanoglu, M.O., et al. TORTOISE: an integrated software package for processing of diffusion MRI data, ISMRM 18th Annual Meeting. Vol. 1597. Stockholm, 2010.
10. Weinshenker B G. Clinical spectrum of neuromyelitis optica 2013. Neurol. Clin. Neurosci., 2014, 2(2): 23–27.
11. Huda S, Whittam D, Bhojak M, et al. Neuromyelitis optica spectrum disorders. Clin. Med. J. R. Coll. Physicians London, 2019, 19(2): 169–176.
12. Makris N, Papadimitriou G M, Sorg S, et al. The occipitofrontal fascicle in humans: A quantitative, in vivo, DT-MRI study. Neuroimage, 2007, 37(4): 1100–1111.
13. Jiang W, Sun X, Huang H, et al. Bilateral parafalcine cortical and leptomeningeal impairment in MOG antibody disease and AQP4 neuromyelitis optica. J. Neuroimmunol., Elsevier B.V., 2022, 369(December 2021): 577898.
Figures
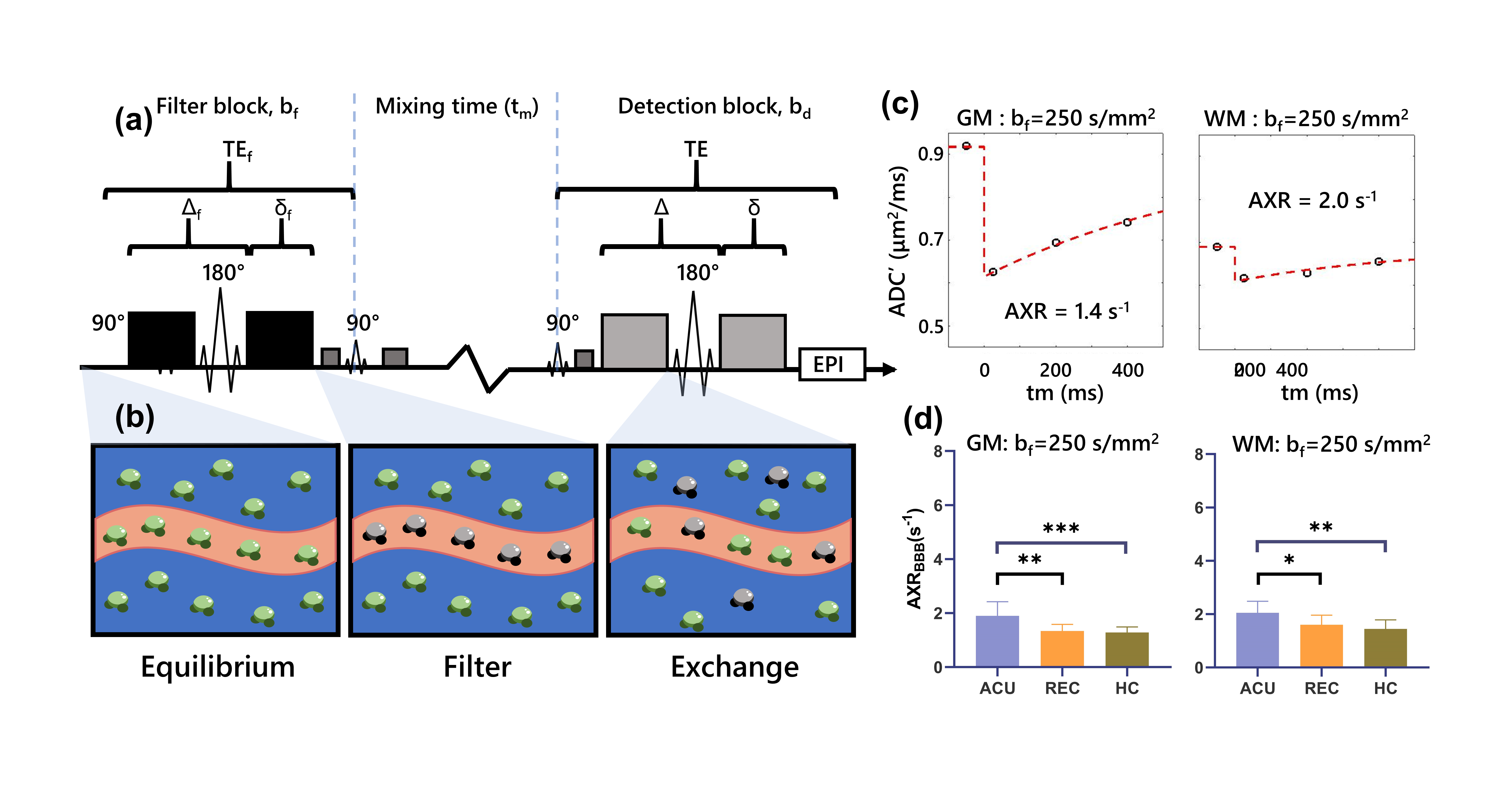
Figure 1. Illustration of the VEXI implemented in this study. (a) Description of VEXI pulse sequence (b) MRI signal evaluation of intravascular and extracellular water molecules during VEXI acquisition. (c) Examples of fitting results. (d) Statistical comparison of AXRBBB values in the whole WM and GM in the acute-phase patients (ACU, n=11), recovery-phase patients (REC, n=12) and healthy controls (HC, n=12). p, significance by one-way analysis of variance.
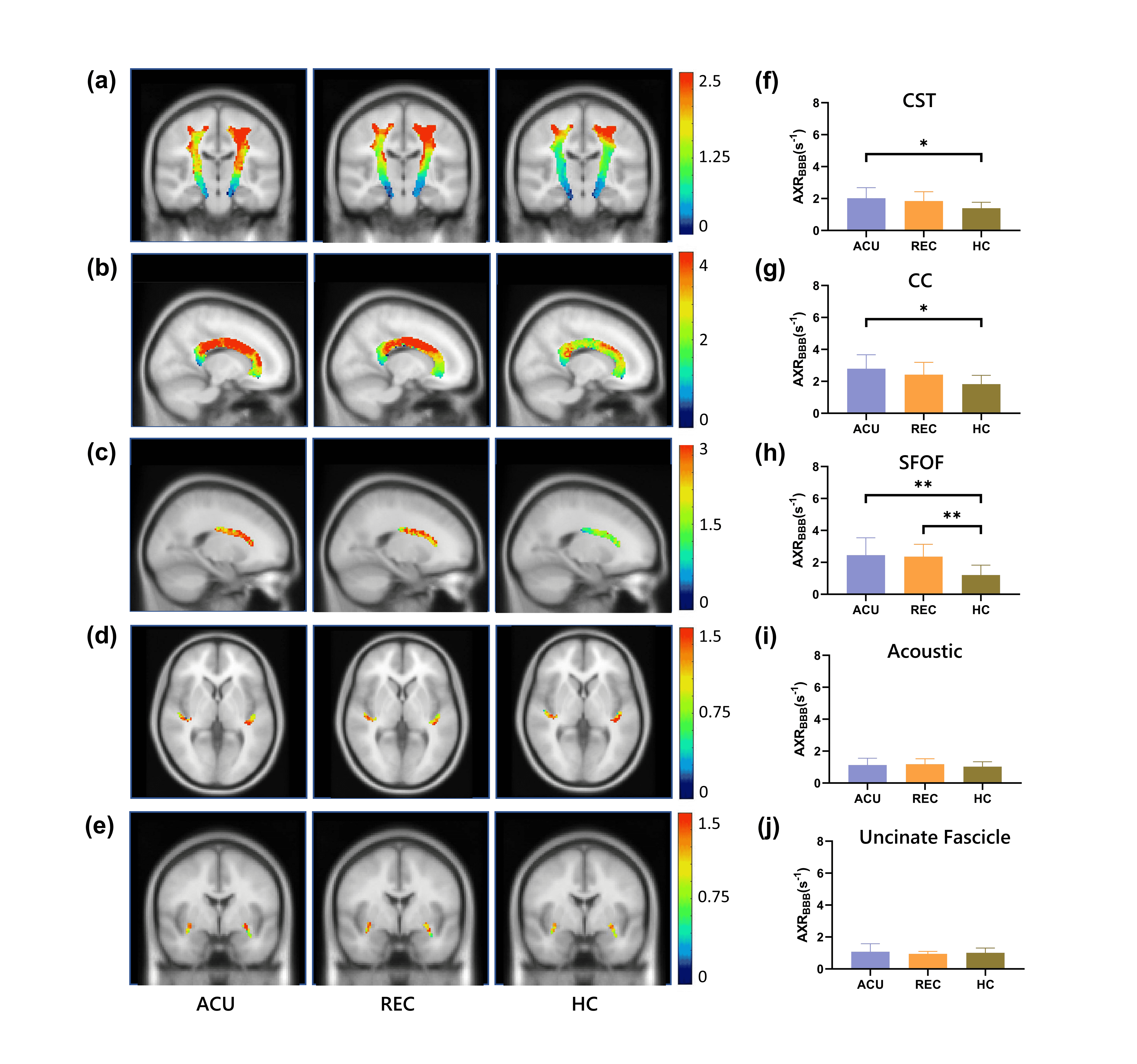
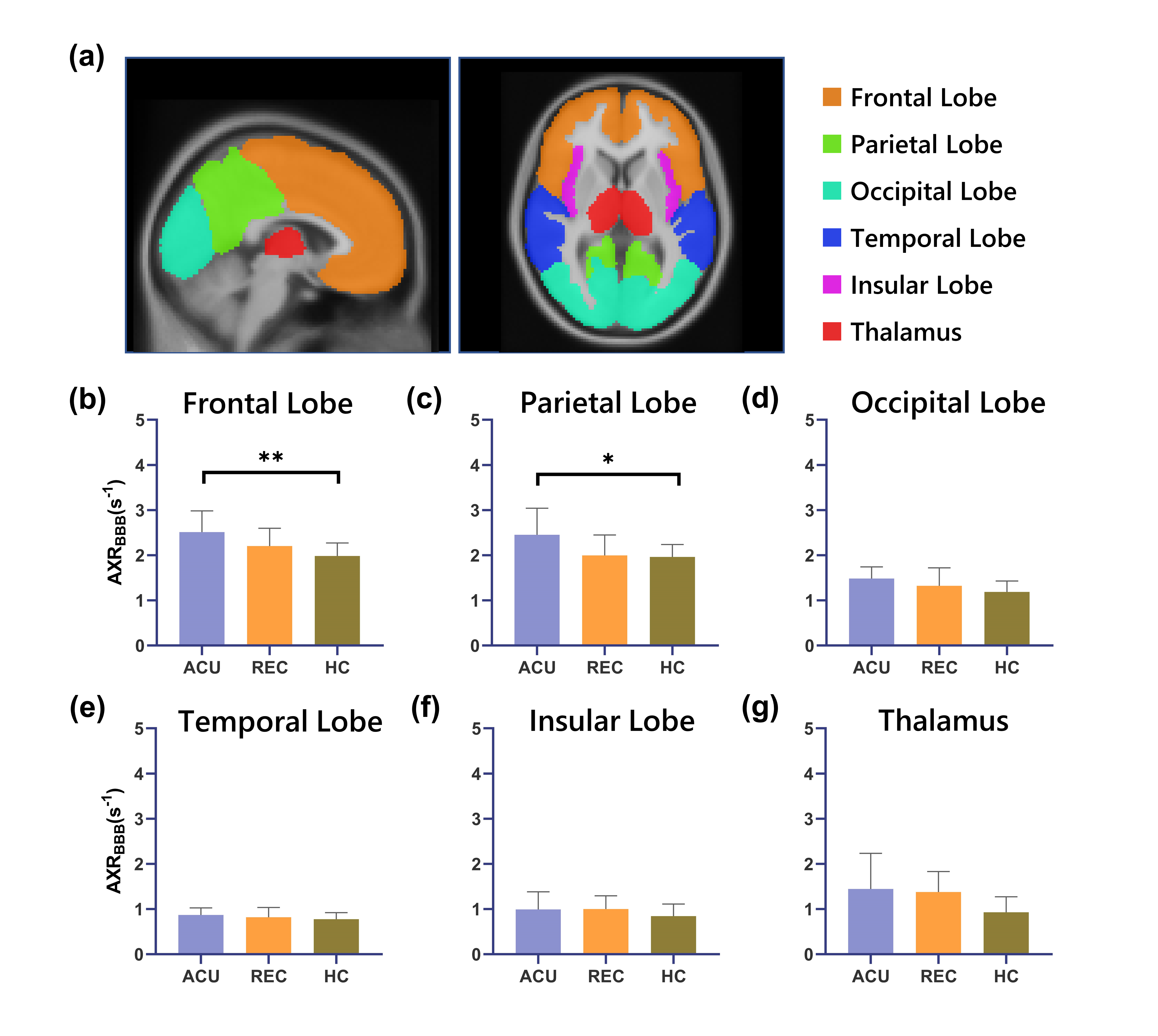
Figure 3. VEXI showing the gradual increase in the AXRBBB from HCs to recovery-phase patients to acute-phase patients in the GM regions. (a) ROI presentation of the GM in the MNI152 space. (b–g) Statistical comparison of AXRBBB values in the frontal lobe (b), parietal lobe (c), occipital lobe (d), temporal lobe (e), insular lobe (f) and thalamus (g) among acute-phase patients (ACU, n=11), recovery-phase patients (REC, n=12) and healthy controls (HC, n=12). p, significance by one-way analysis of variance.
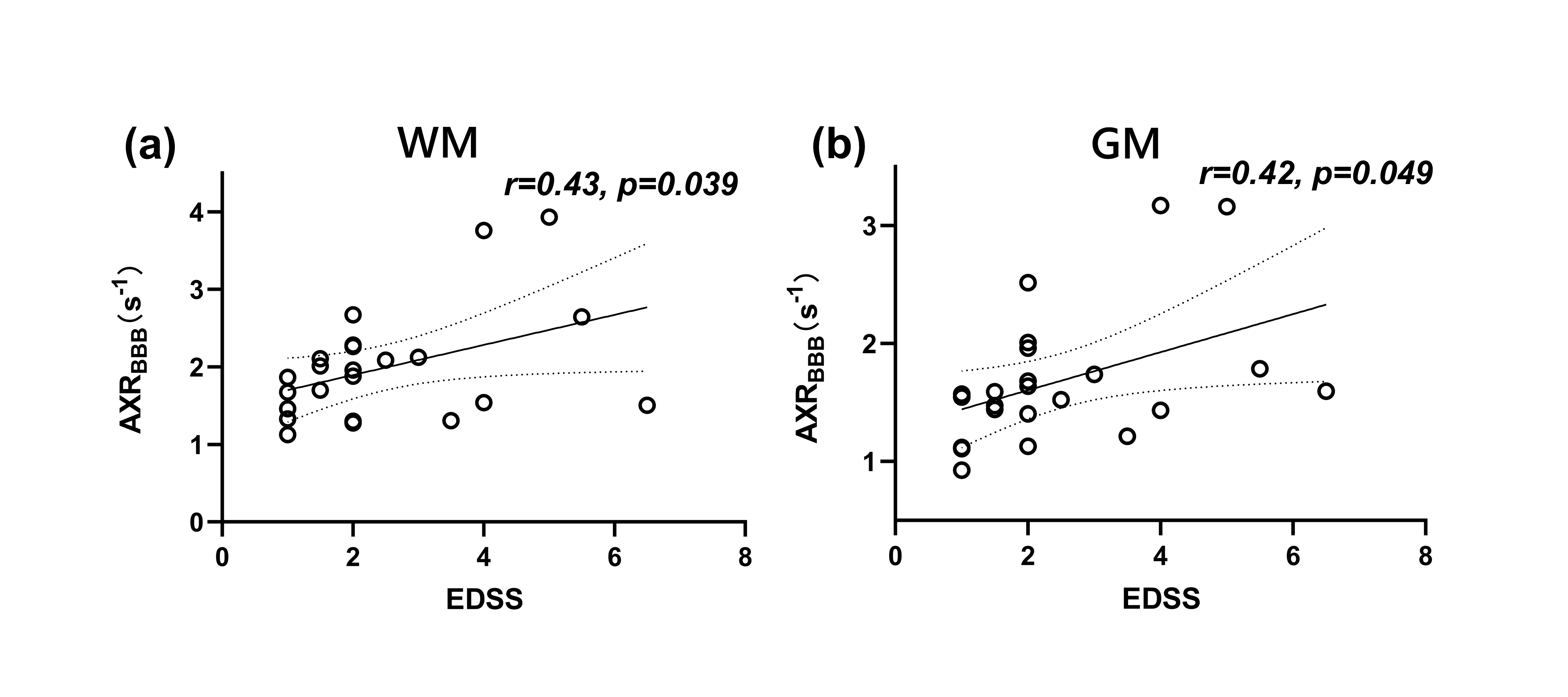
Figure 4. AXRBBB was positively correlated with EDSS scores in both the whole-brain WM (a) and GM (b), all patients (n=23) completed the EDSS scale. Patients with deeper degrees of NMOSD (or worsened motor functions) were associated with higher AXRBBB values. EDSS, Expanded Disability Status Scale.
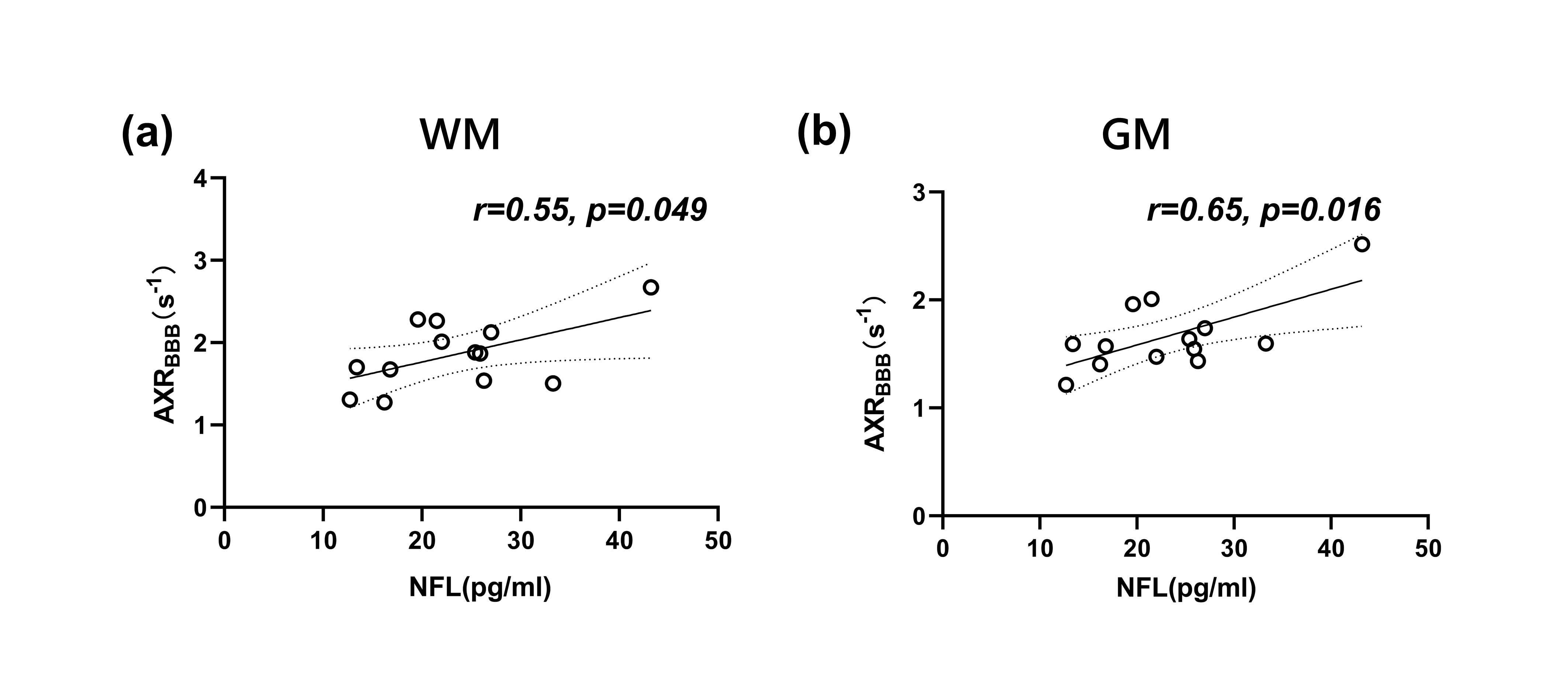
Figure 5. AXRBBB was positively correlated with inflammatory factors in both the whole-brain WM (a) and GM (b), thirteen of the 23 patients had NFL test results. Patients with stronger inflammatory responses had higher AXRBBB values. NFL, neurofilament light chain.