0712
Image quality assessment and longitudinal quality monitoring of clinically-applied AI-based reconstructions in MRI of rectal cancer1MRI Unit, The Royal Marsden NHS Foundation Trust, London, United Kingdom, 2Division of Radiotherapy and Imaging, The Institute of Cancer Research, London, United Kingdom
Synopsis
Keywords: Cancer, Machine Learning/Artificial Intelligence, Image Quality; Quality Control / Quality Assurance; QA/QC; AI/ML image reconstruction
Motivation: With increasing AI adoption in MR-reconstructions, robust quality assessment becomes paramount. This study aims to ensure that AI-techniques meet clinical requirements at implementation and longitudinally.
Goal(s): 1) Compare image quality of AI-imaging with standard techniques in anorectal cancer. 2) Develop longitudinal quality control (QC) assessments capable of detecting changes in AI-reconstructions without resource-intensive evaluations.
Approach: A prospective study involving 40 patients utilised radiologist scoring and quantitative image-quality-metrics (IQMs). Retrospective reconstructions gauged sensitivity of IQMs to reconstruction pipeline changes.
Results: AI-reconstructions demonstrated >50% time savings with improved image quality. Feasibility of quantitative-IQMs for assessing AI-reconstructions is established, providing a practical solution for ongoing QC.
Impact: There is a need to develop QC assessments offering performance monitoring for AI-based reconstructions in diverse clinical settings. The study presents feasible ways to support integration of AI-imaging into clinical practice, including resource-efficient quantitative image quality assessments.
Introduction
AI-based MRI acceleration techniques can improve workflow efficiency and the patient experience by reducing acquisition time whilst maintaining image quality1-3.It is crucial for clinical institutions to ensure AI-based techniques provided by MRI manufacturers meet local clinical requirements4. Local assessments often employ one-off qualitative studies that compare image quality between AI-based and standard techniques. Although such studies provide initial insights into the technique’s performance, they are resource-intensive and consequently are not practical for subsequent monitoring of performance that may change over time, because of model drift or changes associated with measurement and software updates. Also, the sensitivity of AI-based reconstructions to hardware degradation is unknown.
It is therefore essential to develop methods that can assess changes in the AI-reconstruction, to ensure consistent image quality over time5. The aims of this study were (1) to compare the image quality and acquisition time of AI-based accelerated 2D turbo spin echo (TSE) imaging with standard TSE imaging of the rectum, in particular rectal wall layer definition required for accurate tumour staging. The study seeks to establish whether AI-based techniques can significantly reduce acquisition time by over 50% without compromising image quality. (2) To develop quantitative quality control (QC) assessments to enable longitudinal evaluation of AI-based reconstruction techniques to detect changes in performance, without the need for repeated resource-intensive radiologist assessments.
Methods
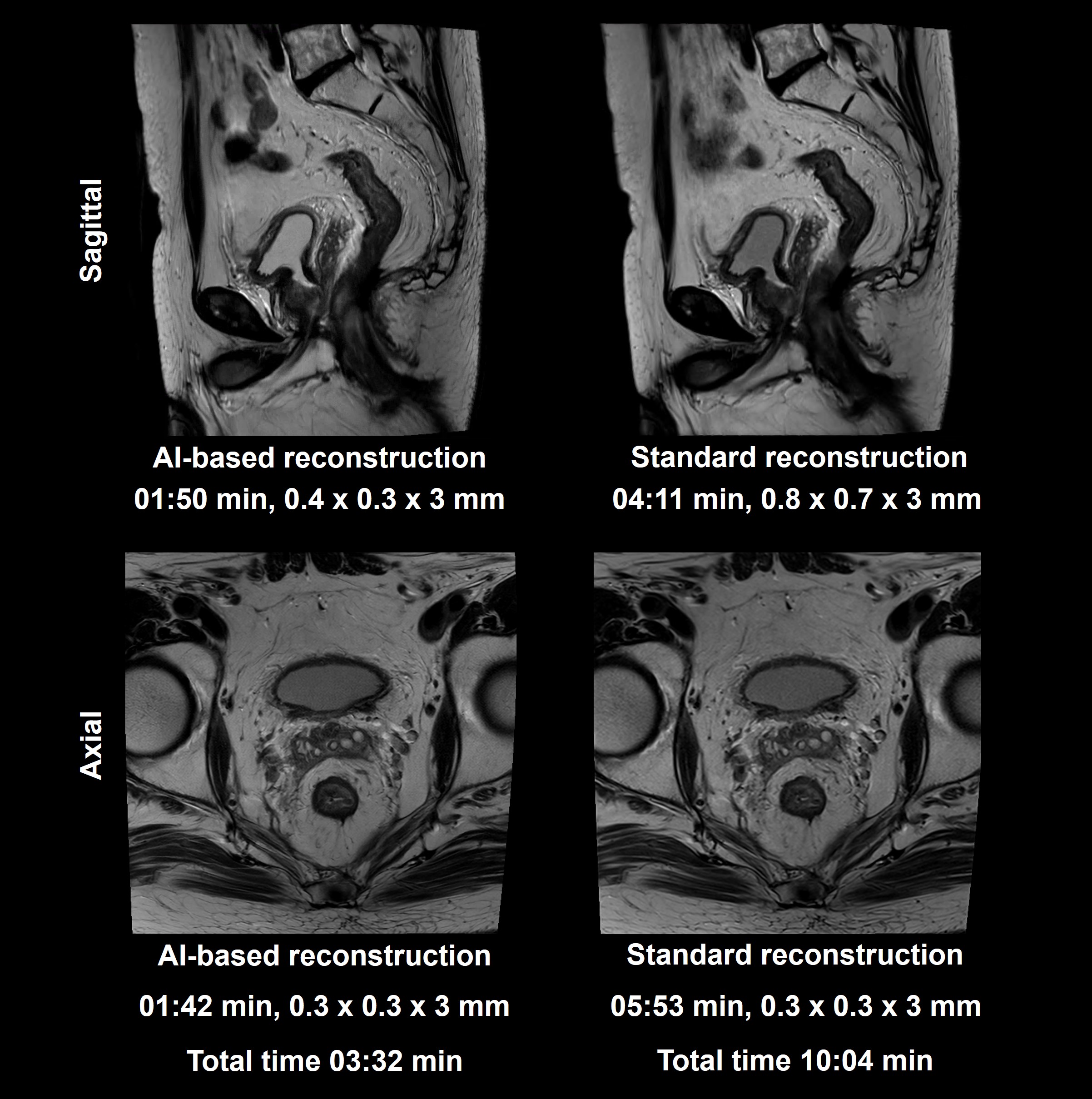
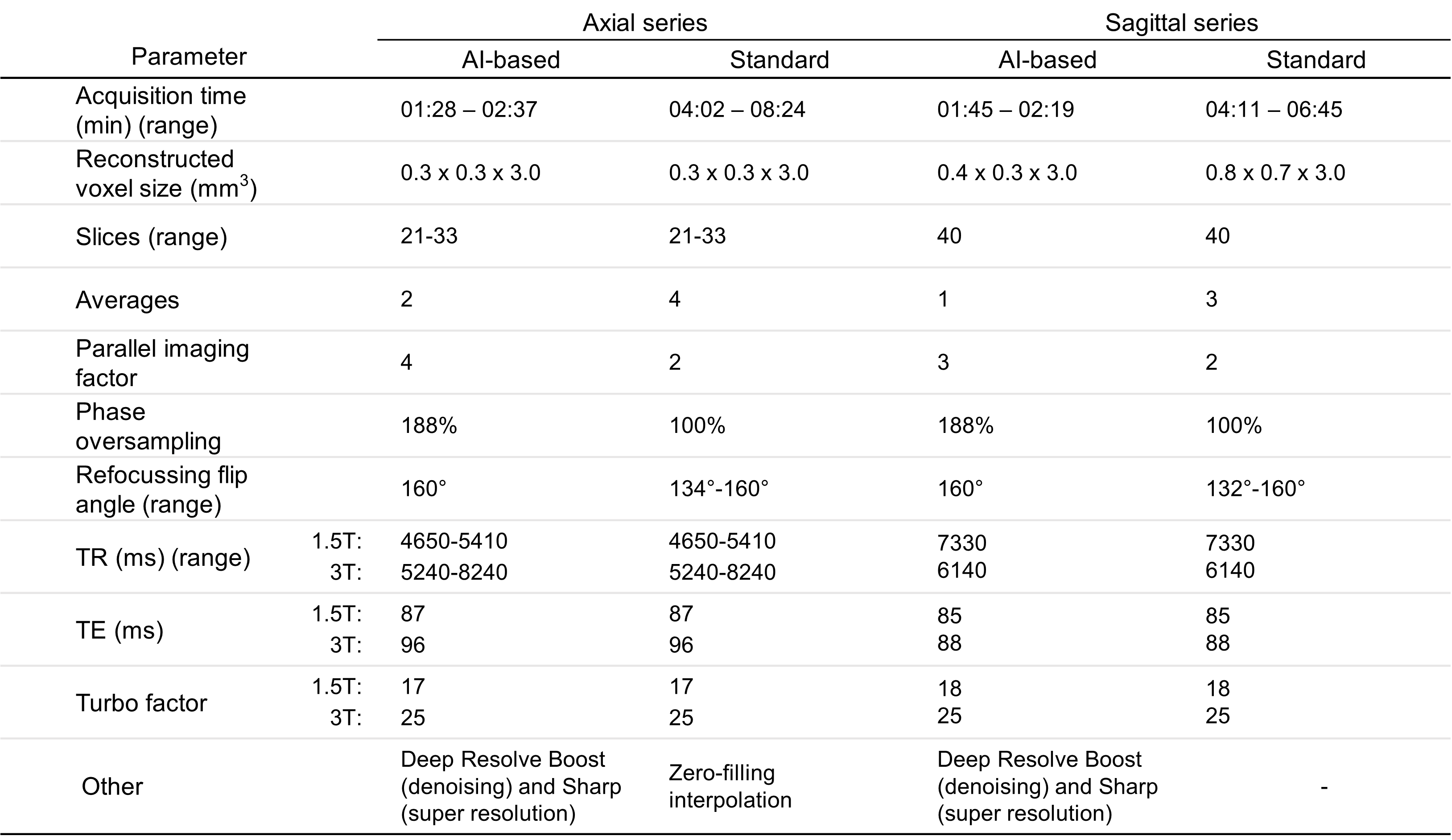
In this prospective study, informed consent was obtained from 40 patients with anorectal malignancy and with rectum in situ (i.e. not had surgical resection) (median age 63 years, range 37-85, 22M). AI-based reconstruction3,6 for de-noising (DR-Boost) and super-resolution (DR-Sharp) (Deep Resolve, Siemens Healthcare, Erlangen, Germany) was applied in accelerated sagittal T2w-TSE and small-field-of-view axial T2w-TSE sequences. AI-sequences were acquired in addition to standard-of-care T2w-TSE imaging at matched slice positions. Patients were imaged on 1.5T MAGNETOM Sola (19/40) or 3T MAGNETOM Vida scanners (Siemens Healthcare).Likert scoring assessment
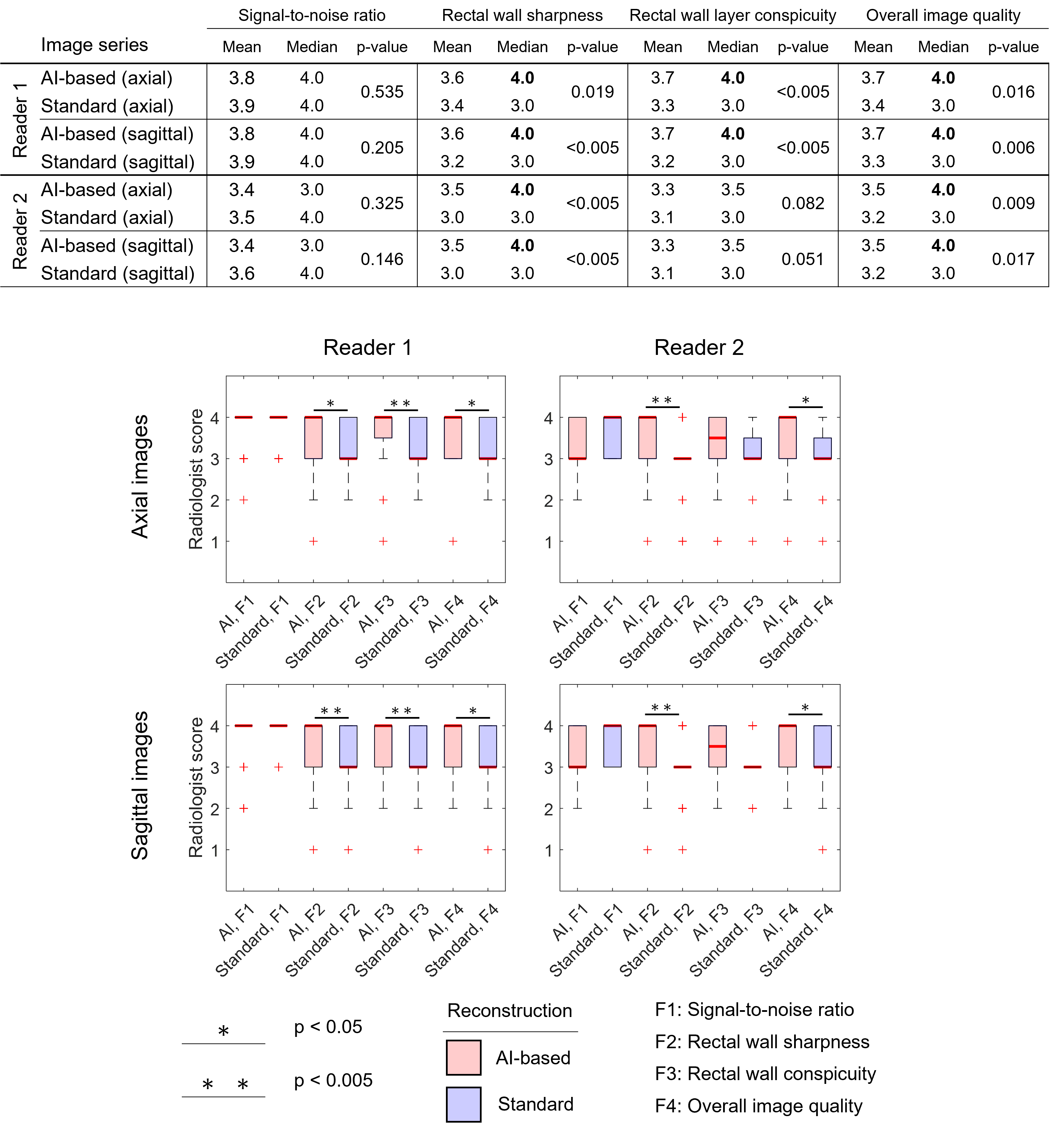
Two radiologists conducted a blinded qualitative analysis using a four-point Likert scale to score four features on each dataset: signal-to-noise ratio (SNR), rectal wall sharpness, rectal wall layer conspicuity, and overall image quality. Differences between median scores for the AI- and standard-series were evaluated using a Wilcoxon-test with a significance level of p<0.05.
Quantitative image quality metrics (IQMs)
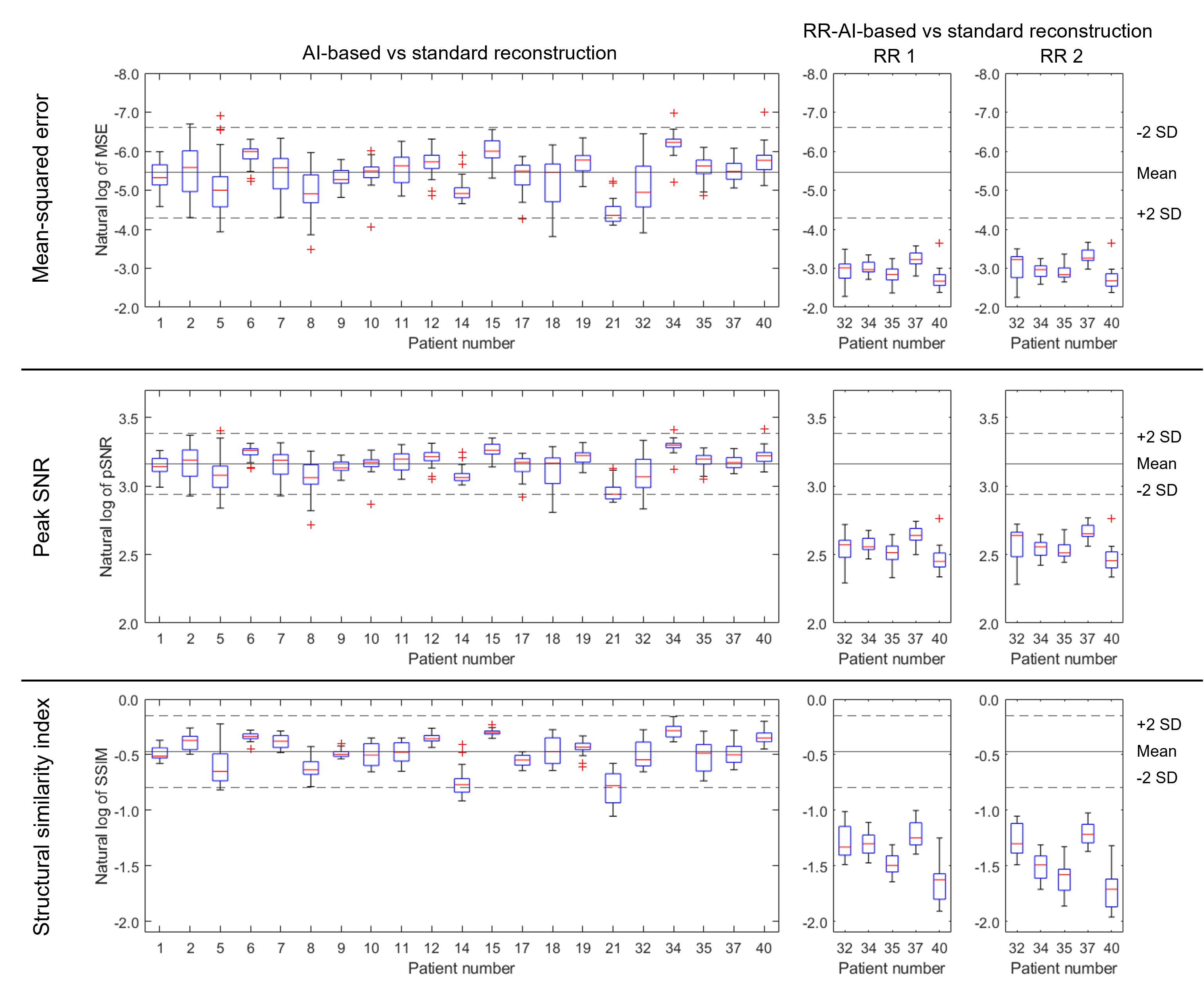
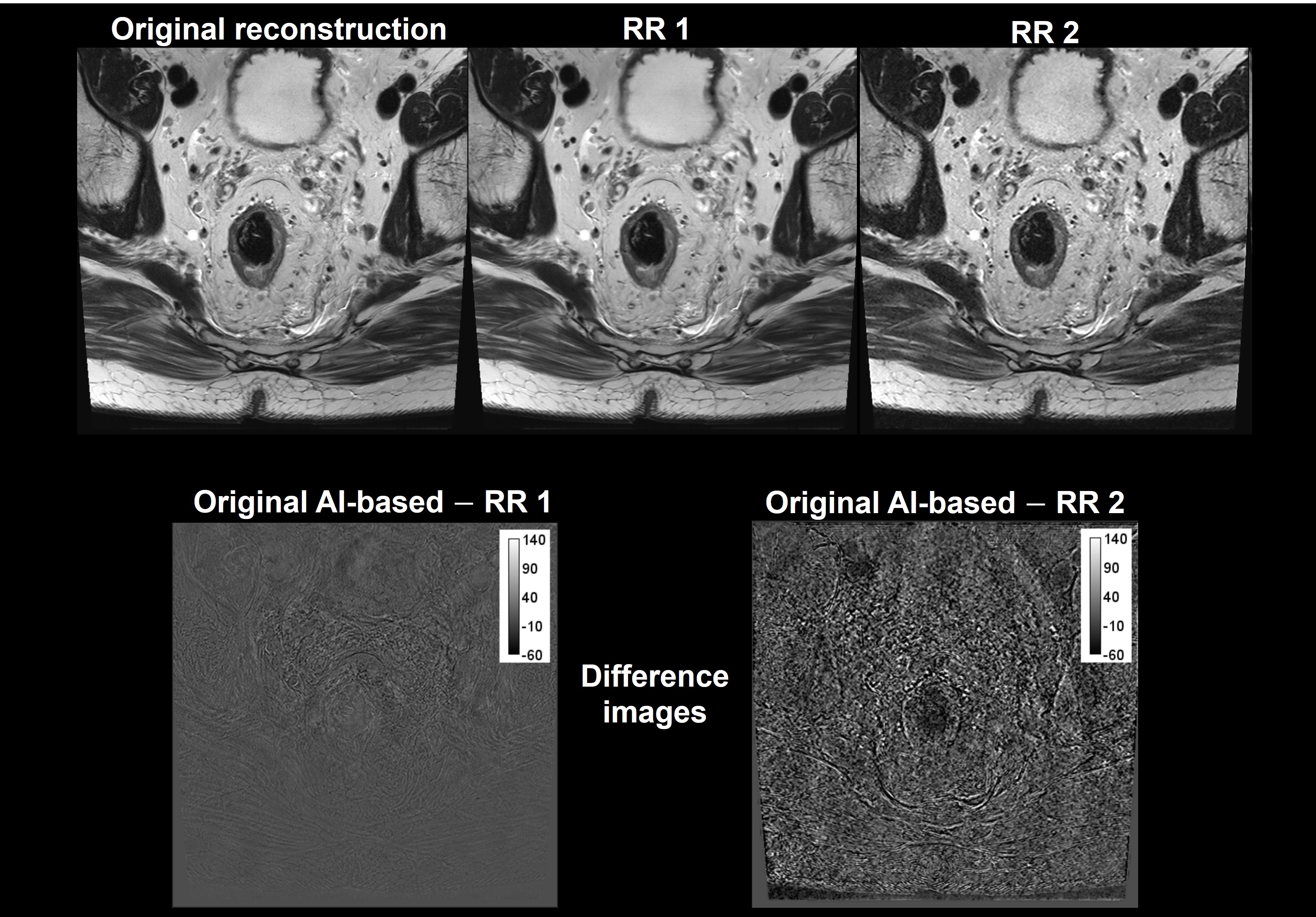
IQMs were measured in MATLAB (R2020b, MathWorks, Natick, MA)7,8 to assess differences between the AI and standard axial images. Mean-squared error (MSE), peak signal-to-noise ratio (pSNR), structural similarity index (SSIM), textural features (entropy), and wavelet decompositions were calculated for a central 200x200-pixel ROI for every slice in the series. Sensitivity of the IQMs to changes in the reconstruction process was evaluated using five patient datasets retrospectively reconstructed (RR) with deliberate modifications (changes to AI-reconstruction mode denoising strength, and additional image smoothing filter). IQMs were compared using a Shewhart chart to establish a control limit9.
Results
AI-based reconstructions allowed for median time savings of 56% (2:21 min) and 69% (4:01 min) for the sagittal and axial series, respectively, without a measurable impact on image quality.Qualitative scores show that the AI-series exhibited better image quality than the standard series (figure 3). There was no significant difference in the median cohort scores for SNR, or in the median scores of the 1.5T and 3T datasets for any feature.
Figure 4 contains Shewhart plots of MSE, pSNR, and SSIM, comparing AI-based and standard reconstructions for all patients acquired at 3T, and RR-datasets. The IQMs for the RR-datasets fell outside the control limit, showing that they are sensitive to changes in the reconstruction pipeline. Other IQMs did not show any difference between the original and RR-datasets.
Discussion
This study shows that AI-based reconstructions allowed for significant (50-70%) time savings to be achieved in a clinical setting in high-resolution T2-weighted rectal cancer imaging, with an overall improvement in image quality. Furthermore, it is possible to use quantitative IQMs (MSE, pSNR, SSIM) to detect changes in the reconstruction pipeline of AI-based techniques without resource intensive image scoring.Other IQMs were insensitive to changes in the reconstruction, however an exhaustive assessment of textural features and wavelet transforms were not performed. Further work will explore additional IQMs as potential QC metrics for an on-going longitudinal evaluation of these imaging protocols in clinical practice and investigate correlations between IQMs and radiologist scores to determine clinical significance.
Conclusion
In conclusion, the study indicates that AI-based reconstruction techniques demonstrate similar or improved rectal wall layer definition and overall image quality, with a 50-70% reduction in acquisition times. Quantitative IQMs (MSE, pSNR, and SSIM) detect changes in the reconstruction pipeline, providing ongoing QC in clinical practice without a significant burden on resources.Acknowledgements
This study represents independent research funded by the National Institute for Health and Care Research (NIHR) Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, London, and by the Royal Marsden Cancer Charity. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.References
1. A. Hosny, C. Parmar, J. Quackenbush, H. J. W. L. Aerts and L. H. Schwartz, "Artificial intelligence in radiology," Nature Reviews Cancer, vol. 18, no. 8, pp. 500-510, 2018.
2. J. H. Thrall, Q. Li, X. Li, C. Cruz, S. Do, K. Dreyer and J. Brink, “Artificial Intelligence and Machine Learning in Radiology: Opportunities, Challenges, Pitfalls, and Criteria for Success,” Journal of the American College of Radiology, vol. 15, pp. 504-508, 2017.
3. K. Hammernik, F. Knoll and D. Rueckert, "Deep Learning for Parallel MRI Reconstruction: Overview, Challenges, and Opportunities," MAGNETOM Flash, vol. 4, pp. 10-15, 2019.
4. D. Daye, W. F. Wiggins, M. P. Lungren, T. Alkasab, N. Kottler, B. Allen, C. J. Roth, B. C. Bizzo, K. Durniak, J. A. Brink and C. P. Langlotz, "Implementation of clinical artificial intelligence in radiology: who decides and how?," Radiology, vol. 305, no. 3, pp. 555-563, 2022.
5. D. B. Larson and G. B. Boland, “Imaging Quality Control in the Era of Artificial Intelligence,” Journal of the American College of Radiology, vol. 16, pp. 1259-1266, 2019.
6. K. Hammernik, T. Klatzer, E. Kobler, M. P. Recht, D. K. Sodickson, T. Pock and F. Knoll, "Learning a variational network for reconstruction of accelerated MRI data," Magnetic resonance in medicine, vol. 79, no. 6, pp. 3055-3071, 2018.
7. The Mathworks Inc., Image Processing Toolbox, MATLAB 9.9.0.2037887 (R2020b) Update 8, Natick, Massachusetts: The MathWorks Inc., 2020.
8. The Mathworks Inc., Wavelet Toolbox, MATLAB 9.9.02037887 (R2020b) Update 8., Natick, Massachusetts: The MathWorks Inc., 2020.
9. A. Simmons, E. Moore and S. C. Williams, "Quality control for functional magnetic resonance imaging using automated data analysis and Shewhart charting," Magnetic Resonance in Medicine, vol. 41, no. 6, pp. 1274-1278, 1999.
Figures