0710
Enhancing Liver Cyst Segmentation for ADPKD Patients Through Deep Learning Assistance1Radiology, Weill Cornell Medicine, New York City, NY, United States, 2Radiology, Columbia university, New York City, NY, United States, 3School of Electrical and Computer Engineering, Cornell University, New York City, NY, United States
Synopsis
Keywords: Liver, Segmentation, ADPKD, PLD, Liver Cyst, Deep Learning, Segmentation Model
Motivation: Autosomal dominant polycystic kidney disease (ADPKD) often also has polycystic liver disease (PLD), impacting patients' well-being. Manually segmenting liver cysts for measuring disease burden is time-consuming and error-prone, necessitating an automated solution.
Goal(s): We introduce a deep-learning (DL) framework for liver cyst segmentation in ADPKD/PLD patients.
Approach: An nnUNet-based framework ensembled 2D and 3D models trained on our institute's ADPKD dataset to detect liver cysts in an external test set. Additionally, we implemented patient, cyst, and voxel-level evaluation metrics for clinical impact assessment.
Results: Our model achieved an 84% cyst-level Dice score significantly reducing annotation time by 91%.
Impact: This research aims to revolutionize PLD monitoring by transitioning from qualitative to quantitative, replicable, and scalable approaches. Advanced DL models can produce high-quality liver cysts annotations and introduce cyst-level evaluation metrics, aiding radiologists with precise disease assessment and clinical decisions.
INTRODUCTION
Autosomal dominant polycystic kidney disease (ADPKD) is a genetic disorder1,2, leading to kidney and liver cyst formation (polycystic liver disease, PLD)3,4. PLD carries significant clinical implications, seriously affecting 2-5% of cases requiring cyst aspiration, fenestration, or liver transplantation5–10. While researchers use total liver volumes for disease assessment, detecting and characterizing early-stage disease is challenging, as small cysts may not significantly impact organ volumes. Therefore, directly measuring liver cysts improves PLD characterization early in its clinical course.Manual cyst annotation is time-consuming, and subject to operator error/variability. Automated MRI liver cyst analysis is challenging due to varying image quality caused by coil positioning, B1 inhomogeneities, and artifacts. While existing methods like thresholding, region growing, and diameter measurements11–13, work well in specific scenarios, they struggle with smaller, ill-defined cysts. Our proposed deep learning (DL) framework significantly reduces annotation time and improves cyst detection accuracy.
METHODS
Dataset. WCM and the Rogosin Institute served 500 ADPKD patients for two decades, collecting MRI data for disease analysis. To create ground-truth masks, 47 patients (with cyst counts 10-475, median=82) were manually annotated by experienced specialists, taking around 10 hours per patient covering all available modalities/planes. The model uses DICOM MRI sequences with NIFTI masks14,15, preprocessed with z-score normalization16 and resizing. 12 patients were reserved for external testing.Model. We employed a self-configuring nnU-Net17 medical image segmentation network with instance normalization, deep supervision18,19, and data augmentation techniques17,20 including contrast adjustments, low-resolution simulation, and gamma correction. The model combines Dice and cross-entropy loss functions21, iteratively adapting patch size for GPU memory optimization. We conducted 5-fold cross-validation using 2D and 3D ensemble models with a ResNet22,23 backbone, ensuring consistent liver size distribution through stratified sampling.
Training Experiments. We trained the following scenarios: 1) Single-channel inputs from different MR sequences (T1, T2, SSFP) and views (axial and coronal) treated as separate data points, with precautions to prevent data leakage between training and validation sets, 2) Single-channel inputs from T2-weighted MR inputs, and 3) Dual-channel inputs of MR images of different sequences and the corresponding organ masks24,25.
Evaluation. We validate the model by comparing its predictions to radiologist-created ground-truth masks. While Dice score is common for segmentation evaluation26,27, it may not suit cysts segmentation due to variations in cyst numbers and sizes among patients. We propose weighting patients by cyst count to calculate macro-Dice (mean Dice score across all patients) and micro-Dice (weighted average of cyst-level Dice scores). To consider cyst size, we propose introducing voxel-level true positive rate (TPR) assessing the overlap of cyst voxels across all patients and cysts. We will consider the time spent correcting the model outputs, offering insight into real-world clinical performance.
Online-learning pipeline. The preliminary framework integrates into an online-learning pipeline24 to provide initial segmentation for new patients, refined through expert correction to generate ground-truth and extend the training set for further training.
RESULTS
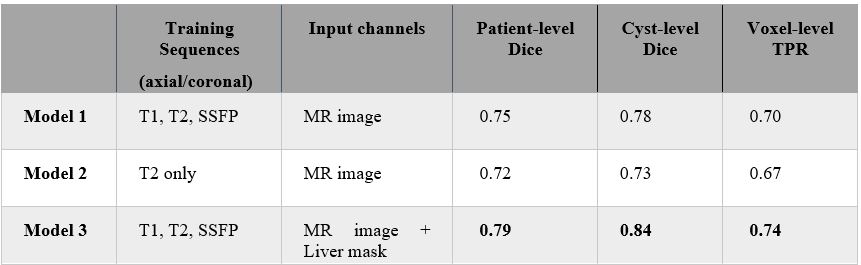
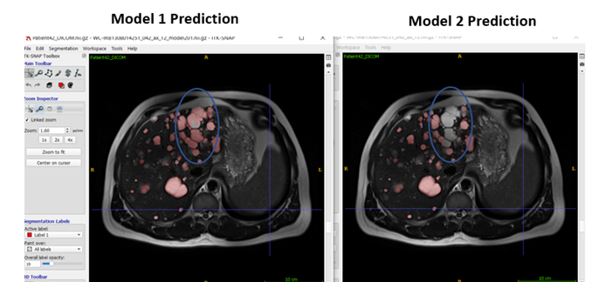
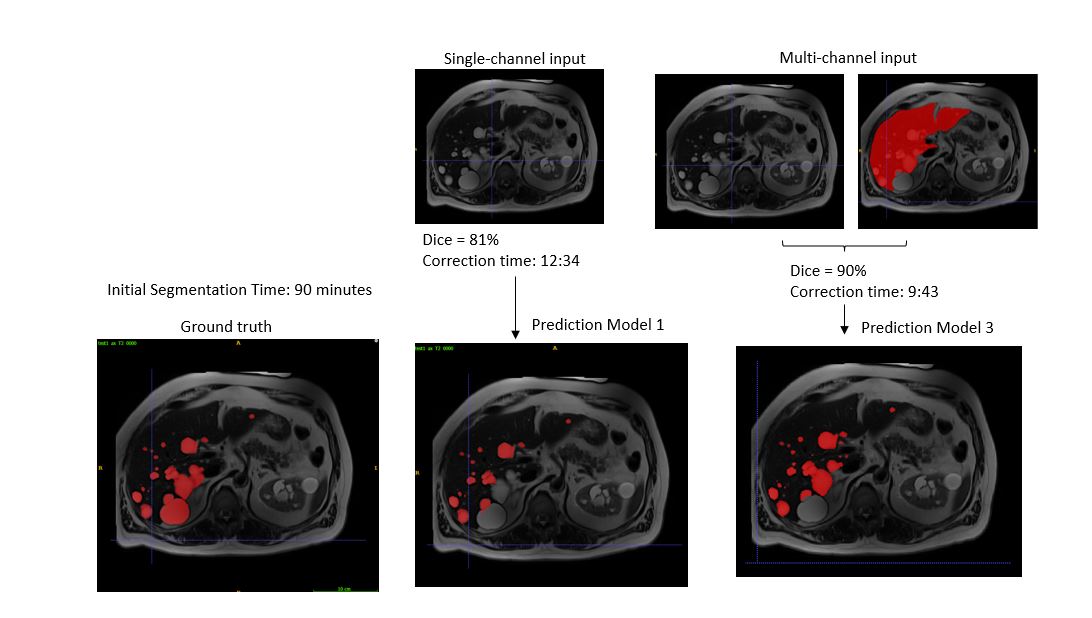
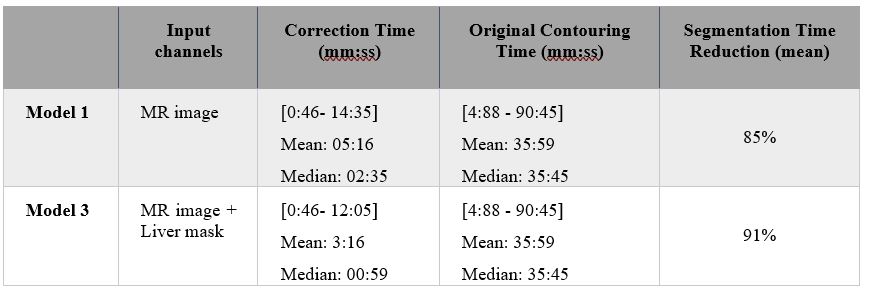
Table 1 demonstrate the DL framework's potential for liver cyst segmentation in ADPKD patients using an external validation set of 12 patients with T2-weighted MR imaging. Model1 outperforms Model2 with a cyst-level Dice score of 0.78 compared to 0.73 in Model2. Figure 1 shows the models’ performance on a T2-weighted axial sample. Results also indicate that, on average, incorporating the MR image and liver mask as a second channel improves cyst detection (Figure 2). Table 2 displays radiologists correction times, revealing an 85% reduction in radiologist time in the model-assisted scenario (Model1), further enhanced to 90% in Model3 by integrating the liver mask as a secondary channel.DISCUSSION
We developed a DL framework for liver cyst detection in ADPKD, introducing patient, cyst, and voxel-level evaluation metrics to assess performance. Our model reduces annotation time by 91%, achieving an 84% cyst-level Dice score and a 74% voxel-level TPR on the external test set. Our algorithm efficiently detects liver cysts of various sizes, including very small ones. In future studies, we plan to expand to multi-class cyst segmentation to differentiate between simple and hemorrhagic cysts as significant biomarkers for disease severity28,29. Further, our future work seeks to establish cyst counts, volumes, and surface area as biomarkers for disease assessment and progression using our efficient liver cyst detection algorithm.CONCLUSION
In conclusion, our motivation to address the time-consuming and error-prone manual segmentation of liver cysts in ADPKD patients led to a DL framework based on nnU-Net and ensemble models. Our approach effectively detects liver cysts and incorporates comprehensive clinical impact assessment metrics. By significantly reducing annotation time and enhancing accuracy, it improves ADPKD-related liver cyst diagnosis and management, benefiting patients’ well-being.Acknowledgements
The authors have nothing to declare.
References
- Chapman, A. B. et al. Autosomal-dominant polycystic kidney disease (ADPKD): Executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 88, (2015).
- Chapman, A. B. et al. Renal structure in early autosomal-dominant polycystic kidney disease (ADPKD): The Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) cohort. Kidney Int 64, (2003).
- Zhang, Z. Y., Wang, Z. M. & Huang, Y. Polycystic liver disease: Classification, diagnosis, treatment process, and clinical management. World J Hepatol 12, (2020).
- Norcia, L. F. et al. Polycystic Liver Disease: Pathophysiology, Diagnosis and Treatment. Hepat Med Volume 14, (2022).
- Van Keimpema, L. et al. Patients with isolated polycystic liver disease referred to liver centres: Clinical characterization of 137 cases. Liver International 31, (2011).
- Macutkiewicz, C. et al. Complications arising in simple and polycystic liver cysts. World J Hepatol 4, (2012).
- Joost P H Drenth, M. C. D. M. N. P. S. K. V. E. T. Medical and surgical treatment options for polycystic liver disease. HEPATOLOGY 52, 2223–2230 (2010).
- Jung, D.-H. et al. Fenestration of liver cysts in polycystic liver disease to improve quality of life: a case report and literature review. Korean J Hepatobiliary Pancreat Surg 19, (2015).
- Pirenne, J. et al. Liver transplantation for polycystic liver disease. Liver Transplantation 7, (2001).
- Alsager, M. et al. Liver transplantation in adult polycystic liver disease: the Ontario experience. BMC Gastroenterol 21, (2021).
- Farooq, Z., Behzadi, A. H., Blumenfeld, J. D., Zhao, Y. & Prince, M. R. Comparison of MRI segmentation techniques for measuring liver cyst volumes in autosomal dominant polycystic kidney disease. Clin Imaging 47, (2018).
- Kim, Y. et al. A Deep Learning Approach for Automated Segmentation of Kidneys and Exophytic Cysts in Individuals with Autosomal Dominant Polycystic Kidney Disease. Journal of the American Society of Nephrology 33, (2022).
- Li, C. et al. IRIS—Intelligent Rapid Interactive Segmentation for Measuring Liver Cyst Volumes in Autosomal Dominant Polycystic Kidney Disease. Tomography 8, (2022).
- Larobina, M. & Murino, L. Medical image file formats. Journal of Digital Imaging vol. 27 Preprint at https://doi.org/10.1007/s10278-013-9657-9 (2014).
- Li, X., Morgan, P. S., Ashburner, J., Smith, J. & Rorden, C. The first step for neuroimaging data analysis: DICOM to NIfTI conversion. J Neurosci Methods 264, (2016).
- Shinohara, R. T. et al. Statistical normalization techniques for magnetic resonance imaging. Neuroimage Clin 6, (2014).
- Isensee, F., Jaeger, P. F., Kohl, S. A. A., Petersen, J. & Maier-Hein, K. H. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat Methods 18, (2021).
- Liwei Wang, C.-Y. L. Z. T. S. L. Training Deeper Convolutional Networks with Deep Supervision. (2015).
- Renjie Li, X. W. G. H. W. Y. K. Z. X. G. S. N. T. S. G. J. A. Q. B. A Comprehensive Review on Deep Supervision: Theories and Applications. (2020).
- Shorten, C. & Khoshgoftaar, T. M. A survey on Image Data Augmentation for Deep Learning. J Big Data 6, (2019).
- Shruti Jadon. A survey of loss functions for semantic segmentation. (2020).
- Foivos I. Diakogiannis, F. W. P. C. C. W. ResUNet-a: a deep learning framework for semantic segmentation of remotely sensed data. (2019).
- Francesco Visin, K. K. K. C. M. M. A. C. Y. B. ReNet: A Recurrent Neural Network Based Alternative to Convolutional Networks. (2015).
- Xinzi He, Z. H. H. D. D. J. R. A. S. S. I. R. S. J. W. K. T. G. S. J. M. C. M. R. S. M. R. P. Test Retest Reproducibility of Organ Volume Measurements in ADPKD Using 3D Multimodality Deep Learning. (2023).
- Sharbatdaran, A. et al. Deep Learning Automation of Kidney, Liver, and Spleen Segmentation for Organ Volume Measurements in Autosomal Dominant Polycystic Kidney Disease. Tomography 8, (2022).
- Bertels, J. et al. Optimizing the Dice Score and Jaccard Index for Medical Image Segmentation: Theory and Practice. in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics) vol. 11765 LNCS (2019).
- Eelbode, T. et al. Optimization for Medical Image Segmentation: Theory and Practice When Evaluating With Dice Score or Jaccard Index. IEEE Trans Med Imaging 39, (2020).
- Suwabe, T. et al. Clinical features of cyst infection and hemorrhage in ADPKD: New diagnostic criteria. Clin Exp Nephrol 16, (2012).
- Marion, Y., Brevart, C., Plard, L. & Chiche, L. Hemorrhagic liver cyst rupture: An unusual life-threatening complication of hepatic cyst and literature review. Ann Hepatol 12, (2013).
Figures