0706
23Na Magnetic Resonance Imaging in Sepsis-Induced Acute Kidney Injury: A Preclinical Study1Heart Center Bonn, Department of Internal Medicine II, University Hospital Bonn, Bonn, Germany
Synopsis
Keywords: Small Animals, Preclinical, Sodium MRI
Motivation: Currently, there is a lack of research in 23Na-MRI, investigating the renal sodium concentration gradient in Sepsis-Induced acute kidney injury (AKI).
Goal(s): This study aimed to investigate sodium concentration changes across the renal parenchyma and to compare them with T1, T2, and T2* alterations as well as kidney perfusion.
Approach: 38 mice (N=19 as control and N=19 with septic AKI) were investigated by multi-parametric MRI.
Results: In septic AKI, thrombi developed in kidneys and caused renal hypoperfusion. Lack of blood supply to kidneys resulted in sodium retention at cortex and little sodium output at pelvis even in the absence of detectable edema.
Impact: This study helps to better understand the radiological pathology of sepsis-induced acute kidney injury in 23Na-MRI. It connects the concept of altered sodium concentration with changes in renal perfusion, T1, T2, and T2* relaxation constants.
INTRODUCTION
Sepsis is defined as an immense immune reaction to an infection, leading to multi-organ dysfunction syndrome (1). Acute kidney injury (AKI) is a common manifestation in sepsis because of a systemic reduced blood pressure and renal hypoperfusion, which leads to an imbalanced corticomedullary concentration gradient (CMG) and impaired urine production (2). To map CMG, 23Na-MRI has emerged as an advanced imaging method to assess the concentration of sodium from renal pelvis to cortex (2). Currently, there is no evidence about the pathophysiological changes of sodium during AKI in 23Na-MRI and its relationship to the established MRI biomarkers; hence, we concentrated on this gap in the present study. In addition, we performed gadolinium dynamic contrast-enhanced (Gd-DCE) perfusion MRI and renal relaxometry to connect the sodium changes to the concurrent renal hypoperfusion, edema, fluid imbalance, and clot formation.METHODS
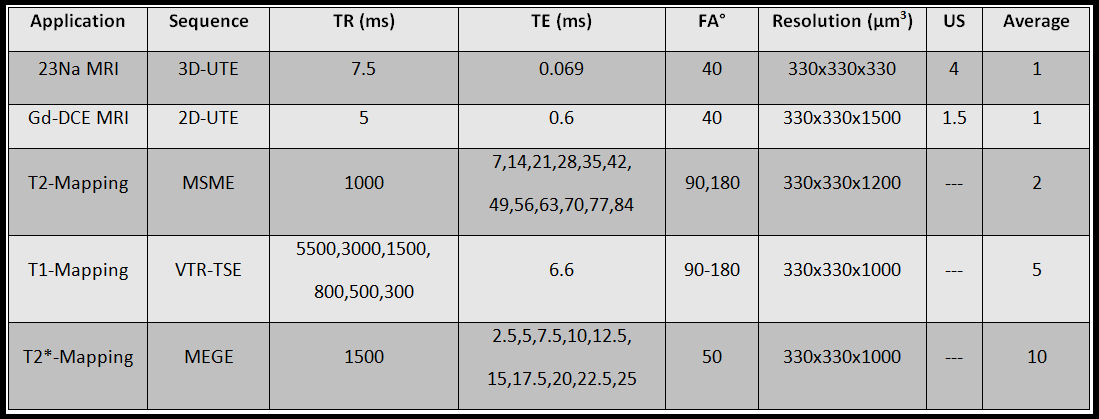
Hardware: An 11.7T preclinical MRI system (Bruker BioSpec USR 117/16) and a commercial 1H/23Na transmit-receive surface coil (Bruker, Ettlingen, Germany) with an inner diameter of 20mm were used.23Na MRI: A customized 3D-Ultra-Short-Echo (UTE) sequence was applied. A detailed description of the parameters can be found in Figure 1. Raw data were regridded by an iterative sampling density compensation and underwent inverse Fourier transform. Since the sodium signal is naturally weak in MRI, an iterative non-local means denoising algorithm (3) was applied to recover the signal of sodium. For group analysis and normalization, the sodium concentration in kidneys was divided by the signal of paravertebral muscles.
Gd-DCE MRI: Golden angle 2D-UTE sequence was applied by administering 200 µl of 0.013 mmol/ml gadobutrol (Figure 1). The reconstruction pipeline was the same as for 3D-UTE, except for two dimensions. The renal arterial blood flow (RABF) was calculated after cubic spline interpolation from the perfusion curves. The glomerular filtration and venous drainage decays (i.e. durations) were quantified using a bi-exponential signal model from the onset of the enhancement peak to the end of the measurement.
Relaxometry: For T2, T1, and T2* mappings, a multi-echo spin-echo, variable-TR turbo-spin-echo, and multi-echo gradient-echo sequences were applied respectively, and the corresponding relaxation maps were generated by a pixel-wise fitting of a suitable physical model (Figure 1).
Animal Model: 38 male C57BL/6 mice at the age of 9 weeks were included in the study. 19 mice were infected by intraperitoneal injection of a feces suspension according to the standard PCI model (4), and 19 mice were used as controls. Infected animals underwent MRI 6 hours post sepsis induction.
Analysis: A region-of-interest (ROI) based analysis was used to assess the individual changes at the renal cortex, medulla, and pelvis. For statistics, Mann-Whitney U-Test was applied.
RESULTS
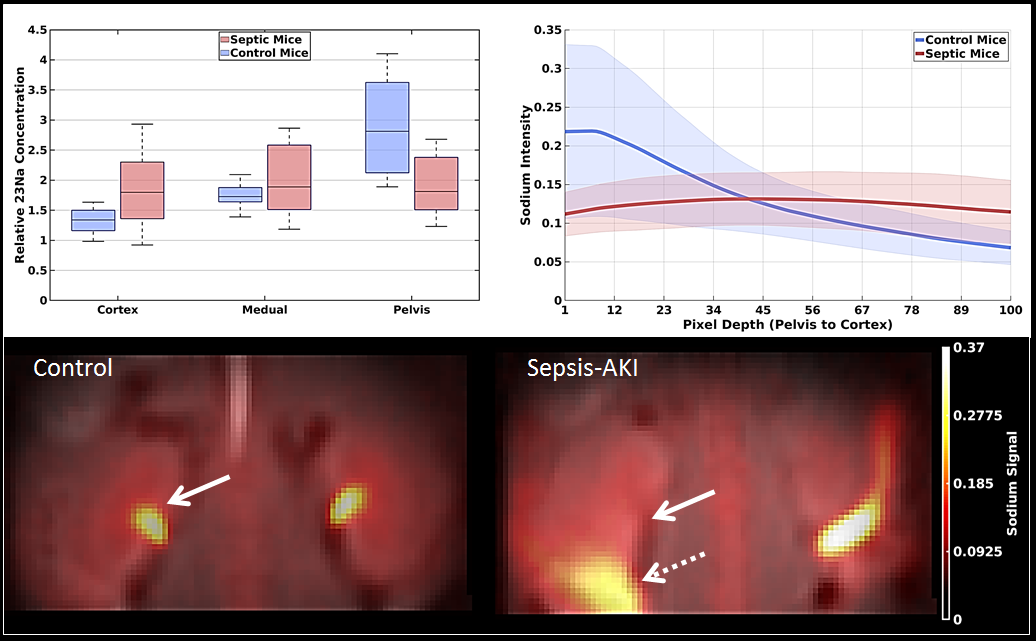
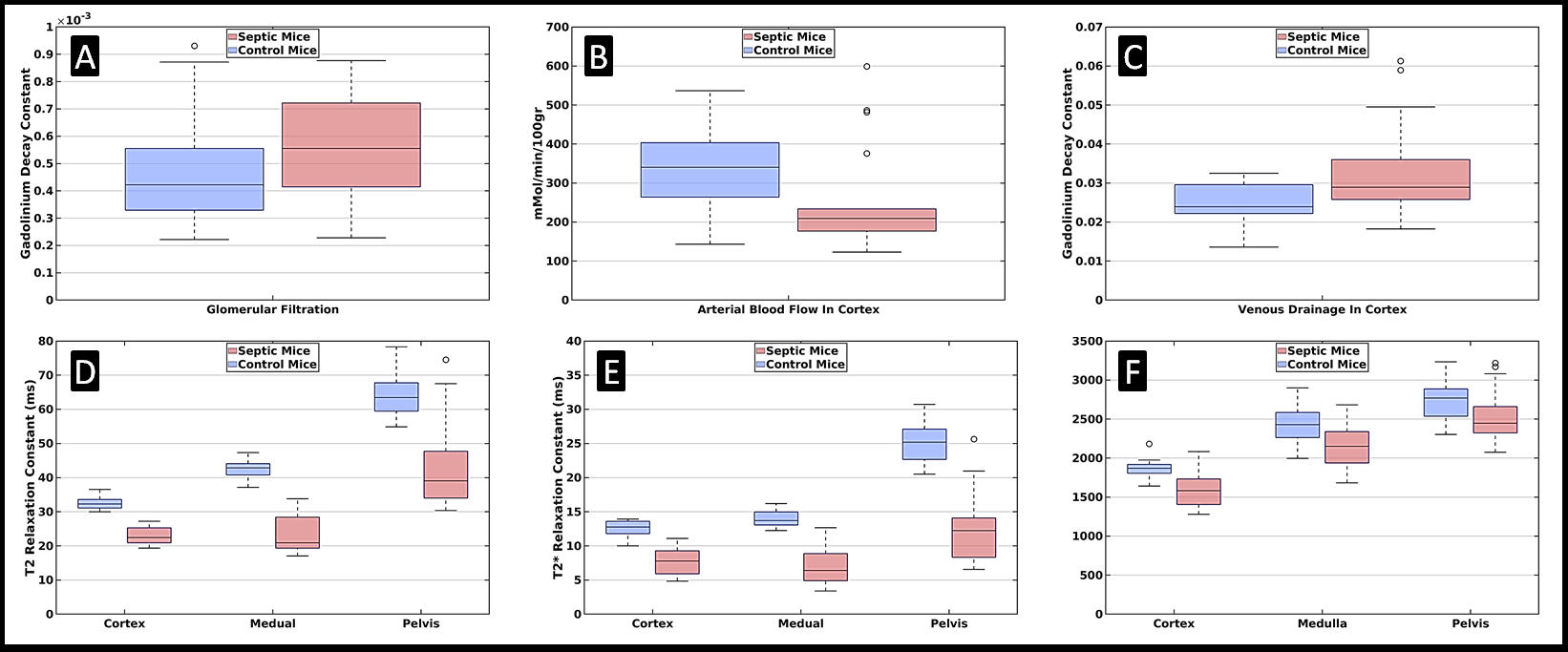
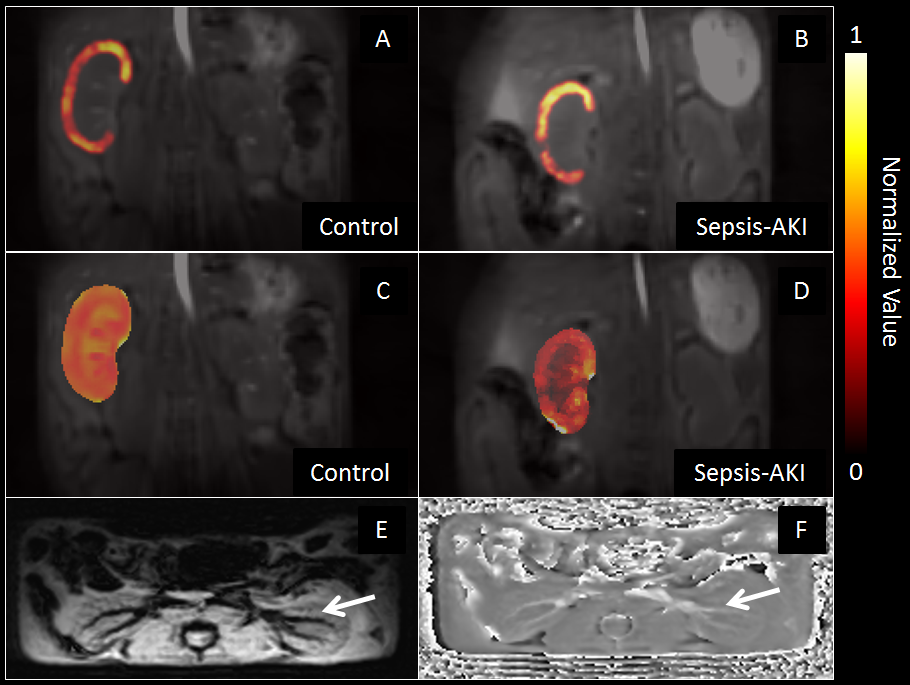
There was a significant difference between the sodium concentrations of cortex and pelvis in AKI in comparison to the control group (p<0.05, Figure 2). CMG of sodium was flattened in AKI compared to the healthy animals (Figure 2). The cortical, medullary, and pelvical T1, T2, and T2* relaxation times were systematically and significantly lower in AKI than in healthy kidneys (p<0.05, Figure 3). RABF was significantly reduced in sepsis in comparison to control (p<0.05, Figures 3-4). Renal venous drainage and glomerular filtration were both substantially slower (i.e. longer constant or longer duration) in septic-AKI (Figures 3-4).DISCUSSION
According to the visual assessments of gradient echo images (Figure 4), septic animals developed micro- and macro-thrombi inside the renal vessels, which led to a reduced RABF at the renal cortex and medulla. The reduced T2* relaxation times in AKI confirmed the formation of micro-/macro-clots. The corticomedullary hypoperfusion caused slower filtration and resulted in reduced urine excretion. Accordingly, the decreased T2 and T1 relaxation constants suggested the loss of fluid inside the kidneys with AKI. The T2 relaxation times showed no signs of edema in the injured kidneys. In addition, the venous drainage of the kidneys with AKI was on average slowed down, which could be an explanation for an increased sodium concentration at the cortical regions post-sepsis. Since the animals with AKI excreted less urine than normal, the concentration of sodium was also lost at pelvis, which resulted in a flattened sodium CMG in combination with the increase of cortical sodium concentrations. According to the author’s knowledge, this study was the first instance of the sodium MRI application in the AKI investigations.CONCLUSION
In conclusion, renal sodium MRI can give valuable information on sodium hemostasis. Accordingly, the sodium CMG was lost in AKI which might be an early indication factor about the kidney involvement in acute sepsis.Acknowledgements
There are no acknowledgments regarding this study.References
1.Guarino M, Perna B, Cesaro AE, et al. 2023 Update on Sepsis and Septic Shock in Adult Patients: Management in the Emergency Department. J Clin Med. 2023;12(9):3188. Published 2023 Apr 28. doi:10.3390/jcm120931882.
2. Akbari A, Lemoine S, Salerno F, et al. Functional Sodium MRI Helps to Measure Corticomedullary Sodium Content in Normal and Diseased Human Kidneys. Radiology. 2022;303(2):384-389. doi:10.1148/radiol.2112383.
3. Manjón JV, Coupé P, Martí-Bonmatí L, Collins DL, Robles M. Adaptive non-local means denoising of MR images with spatially varying noise levels. J Magn Reson Imaging. 2010;31(1):192-203. doi:10.1002/jmri.220034.
4. Gonnert FA, Recknagel P, Seidel M, et al. Characteristics of clinical sepsis reflected in a reliable and reproducible rodent sepsis model. J Surg Res. 2011;170(1):e123-e134. doi:10.1016/j.jss.2011.05.019
Figures