0704
Comparison of cardiomyocyte orientation assessed with diffusion tensor imaging and a high-angular resolution diffusion imaging model1CMR unit, Royal Brompton Hospital, London, United Kingdom, 2NHLI, Imperial College, London, United Kingdom, 3Imperial College, London, United Kingdom
Synopsis
Keywords: Preclinical Image Analysis, Diffusion/other diffusion imaging techniques
Motivation: The orientation of the cardiomyocytes can be probed non-invasively with diffusion imaging. In-vivo, this is typically assessed by the orientation of the primary eigenvector in a diffusion tensor model, although questions remain about the ability of this model to probe complex cardiomyocyte arrangements.
Goal(s): To assess the agreement of cardiomyocyte orientation measures given by a diffusion tensor and a more robust q-ball model.
Approach: A diffusion tensor model was compared to a q-ball diffusion model in a healthy porcine heart.
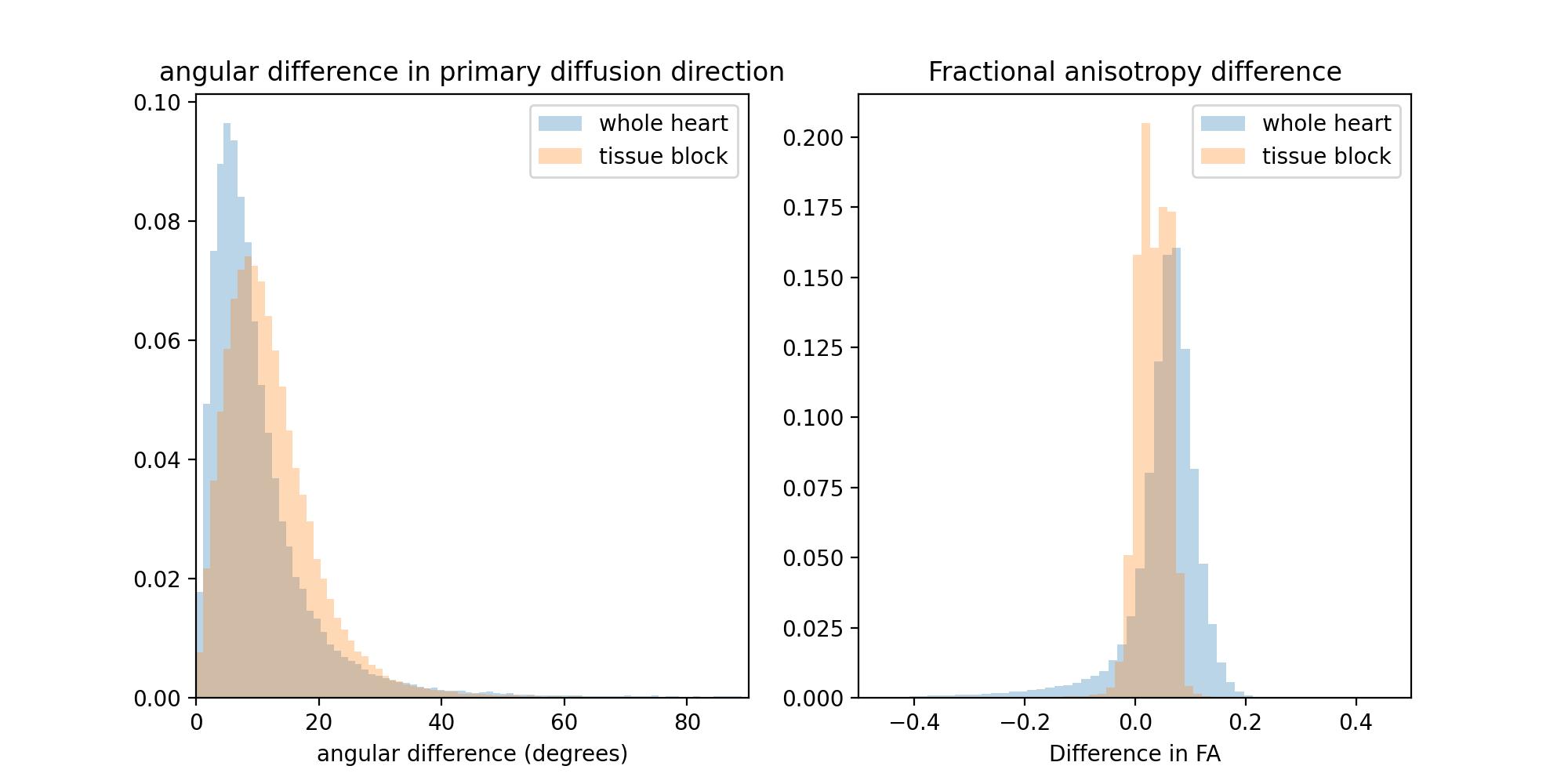
Results: Median angular deviations of 7.8 and 10.8 degrees were found for the main diffusion direction between the two models.
Impact: We provide an estimate of cardiomyocyte angular orientation differences between a diffusion tensor model and a more robust diffusion q-ball model with a higher angular resolution in a healthy porcine heart.
INTRODUCTION
Diffusion Tensor Cardiac Magnetic Resonance (DTCMR) is a novel non-invasive imaging technique that can uncover details of the cardiac microstructure in the living heart. This new imaging technique provides us with a unique opportunity to probe the complex and dynamic cardiac muscle architecture in-vivo in health and disease [1].DTCMR acquires multiple diffusion weighted images (DWIs), measuring the 3D diffusion of water molecules. These DWIs need to be processed to extract the microstructural information. This can be done by diffusion tensor imaging (DTI) [2], where one fits a rank-2 tensor assuming a 3D Gaussian diffusion. This method is often used in-vivo as a tensor can be fitted with a minimum of 7 DWIs, although in practice more images are usually acquired to reduce noise. A major limitation of DTI is that the diffusion model is inappropriate to accurately measure diffusion in voxels with a complex microstructure, for example with crossing or diverging cardiomyocytes. To overcome this limitation more complex models, capable of modelling multiple cardiomyocyte orientations per voxel, exist. Higher Angular Resolution Diffusion Imaging (HARDI) offers increased degrees of freedom compared to DTI [3], but this advantage comes at the cost of requiring a significantly higher number of diffusion images, and therefore HARDI is currently only practical for ex-vivo scans, where imaging times can span for more than a day.
It has been shown that the primary diffusion direction in DTI aligns with the cardiomyocyte long-axis [4]. In this work we compare the direction of cardiomyocytes given by DTI and a HARDI (q-ball) model [5] to determine if DTI’s limitations are significant in a healthy heart.
METHODS
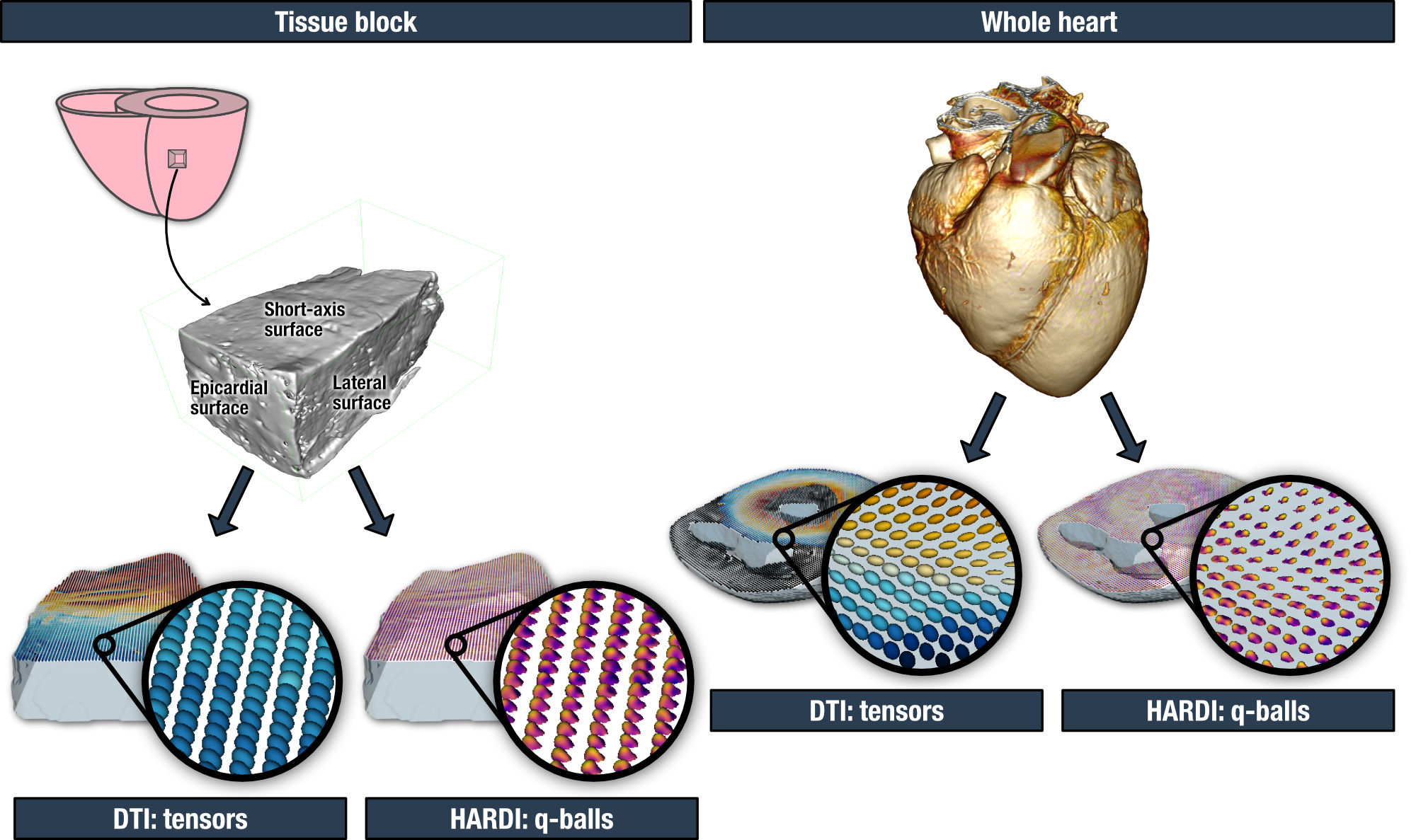
A healthy porcine whole heart was scanned with a diffusion weighted spin-echo sequence in a 3T scanner (SIEMENS Vida): 1.5mm isotropic resolution, b = 500, 1000 s/mm2, 256 directions. A porcine healthy left ventricular tissue block was also imaged in a 9.4T scanner (Bruker BioSpec): 0.2mm isotropic resolution, b = 600, 1100 s/mm2, 150 directions.We used DiPy [6] libraries to fit a tensor model and a Constant Solid Angle (q-ball) model to the data (Figure 1). The q-ball peaks were set at a relative peak threshold weight of 0.1 and a minimum separation angle of 20 degrees.
We extracted the main diffusion direction (E1) with both models and calculated the angular deviation for each voxel (ΔE1) across the entire volume. We also calculated the difference in fractional anisotropy given by both models (ΔFA). Finally, we generated tractograms in the heart block with an Euler integration with trilinear interpolation [7] method: propagation step size 0.5, quantitative anisotropy stopping threshold 0.1, and minimum length of 10 voxels.
RESULTS
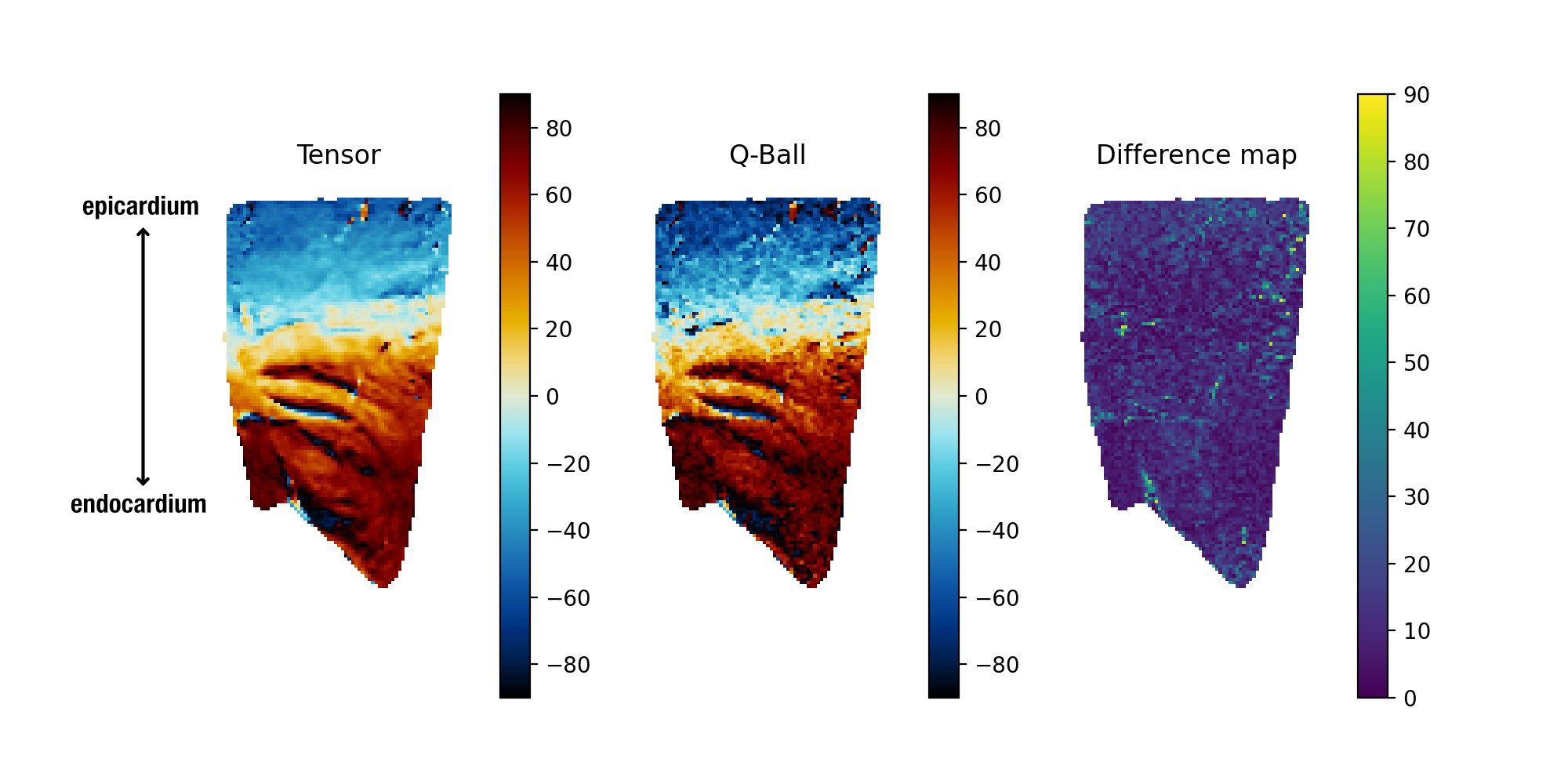
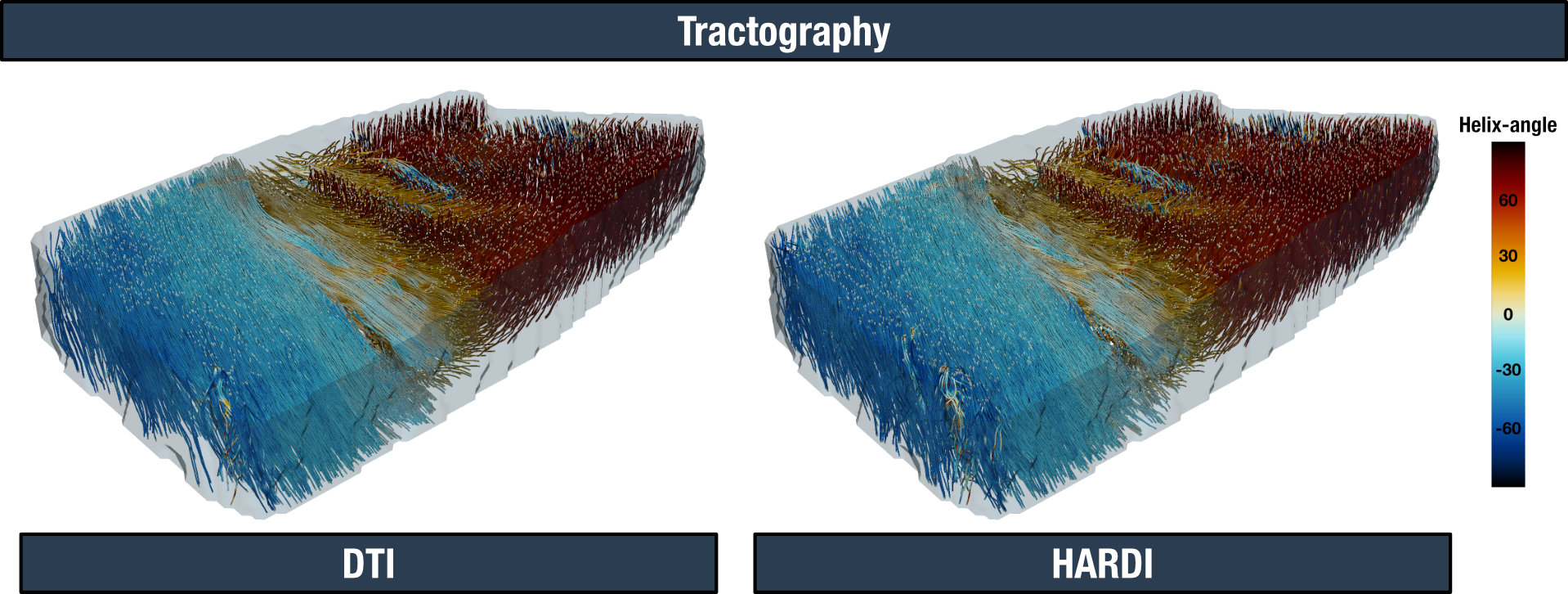
Whole heart and tissue block ΔFA and ΔE1 are shown in Table 1 and Figure 2. All paired comparisons with p<0.001, i.e. FA and E1 values are statistically different between DTI and HARDI. Figure 3 shows the helix-angle of the tissue block for one slice. Figure 4 shows the generated tractograms for both models; a total of 5700 tracts were generated for the DTI (lengths = 50 [43, 73]), and 6687 tracts for the HARDI model (lengths = 45 [42, 61]).DISCUSSION
The primary diffusion direction and fractional anisotropy value distributions are significantly different between the two models, although, more than half the voxels have angular differences of less than 8 degrees (whole heart) and 11 degrees (tissue block) for the primary diffusion direction. Thus, tensor model limitations, at this spatial resolution, do not introduce large errors when assessing cardiomyocyte orientation in a healthy heart. Tractography results are visually very similar, although we must emphasise that the tracts do not represent a real cardiac structure, solely the orientation stream of a syncytium of cardiomyocytes. Future work is planned to perform the same analysis at longer diffusion mixing times.Acknowledgements
This work was supported by the British Heart Foundation RG/19/1/34160.References
[1] Nielles-Vallespin S, Khalique Z, Ferreira PF, et al. Assessment of Myocardial Microstructural Dynamics by In Vivo Diffusion Tensor Cardiac Magnetic Resonance. J Am Coll Cardiol. 2017; 69: 661-676.
[2] Basser PJ, Mattiello J, LeBihan D. Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magn Reson B. 1994; 103: 247-54.
[3] Descoteaux M. High Angular Resolution Diffusion Imaging (HARDI). In: Wiley Encyclopedia of Electrical and Electronics Engineering John Wiley & Sons, Ltd; 2015. p. 1-25.
[4] Scollan DF, Holmes A, Winslow R, et al. Histological validation of myocardial microstructure obtained from diffusion tensor magnetic resonance imaging. Am J Physiol. 1998; 275: H2308-18.
[5] Tuch DS. Q-ball imaging. Magn Reson Med. 2004; 52: 1358-72.
[6] https://dipy.org/
[7] Garyfallidis E. (2012). Towards an Accurate Brain Tractography. PhD thesis, University of Cambridge
Figures