0697
Multiparametric MRI of a Mouse-INtraDuctal (MIND) in vivo model of human invasive lobular breast carcinoma1Division of Radiotherapy and Imaging, The Institute of Cancer Research, London, United Kingdom, 2Division of Breast Cancer Research, The Institute of Cancer Research, London, United Kingdom, 3INSERM U1148, Laboratory for Vascular Translational Science, University Paris Diderot, Paris, France, 4Faculty of Life Sciences and Medicine, King's College London, London, United Kingdom
Synopsis
Keywords: Biology, Models, Methods, Cancer, preclinical, biomarkers, elastography
Motivation: Invasive lobular carcinoma (ILC) is a major subtype of breast cancer but remains very difficult to detect until late stage. There is a lack of sensitive imaging techniques for the diagnosis of ILC.
Goal(s): To define clinically-translatable MRI biomarkers of the heterogeneous tumour microenvironment in ILC.
Approach: A Mouse-INtraDuctal (MIND) model was used to emulate late stage ILC. Multiparametric MRI was performed on ~10 month-old tumours.
Results: ILC exhibited bimodal ADC and stiffness profiles. Invasive tumour regions displayed low ADC and elevated stiffness compared to lobular in situ regions.
Impact: Multiparametric MRI can inform on the evolving microenvironment within MIND model of invasive lobular carcinoma.
Invasive regions displayed restricted water diffusion and elevated stiffness, highlighting the utility of DWI and MRE as informative techniques for detecting and assessing invasiveness.
Introduction
Invasive lobular carcinoma (ILC) is the second most common subtype of breast cancer, accounting for 15% of all breast cancers. ILC arises within the milk-producing terminal ductal lobular units, and intraepithelial growth will ultimately invade through the basement membranes into the surrounding breast tissue. ILC is characterised by an insidious growth pattern where the stromal invasion causes little disturbance of the normal architecture, making it difficult to detect on conventional mammography 1. There is an unmet clinical need for more sensitive imaging techniques for the detection and diagnosis of ILC.Studying ILC has been challenging due to the paucity of suitable pre-clinical models. Using the Mouse-INtraDuctal (MIND) model, in which human cancer cells are engrafted into the primary milk ducts of immunocompromised mice, more faithfully emulates human tumour biology and progression 2. Non-invasive imaging of MIND models represents a powerful preclinical approach for longitudinal investigation of tumour progression and therapeutic response in vivo. This refined approach can improve the accuracy of pre-clinical data, and, in defining relevant imaging biomarkers, be used to guide their introduction into clinical trials.
In this study, late stage ILC was modelled using intraductal engraftment and characterised with multiparametric MRI and histopathology.
Methods
The lobular cell line IPH-926-RFP-Luc2 was bilaterally injected into the milk ducts of the 4th mammary glands of female NSG mice (2x105 cells/8mL/gland) (n=6) 3. Tumour growth was monitored by bioluminescence imaging (Fig.1).In vivo MRI was performed ~10 months after engraftment using a 7T horizontal system (Bruker) and a 40mm birdcage coil. MRI included acquisition of anatomical T2-weighted RARE images, and diffusion-weighted spin echo images (TE/TR=39/1500ms, 5 b-values=200-1000s/mm2) for determination of ADC, inversion recovery-TrueFISP images (TE/TR=1.7/3.4ms, 50 TI=0-2720ms) for estimating T1 and T2 relaxation times, and multi-echo GE images (TE/TR=3/200ms, 8 echoes) to quantify R2* from the slice with the largest tumour cross-section. One tumour-bearing mouse underwent MR elastography (MRE), acquired using a 1,000Hz mechanical vibration applied directly to the tumour/gland and a synchronised spin echo sequence with 4 phase time-points (TE/TR=30/504ms).
Tumour volumes were obtained from segmentation of the T2-weighted images. Tumour ADC, native T1, T2 and R2* for all 12 tumours were extracted from whole tumour ROIs and displayed as frequency histograms from which the median and IQR were computed.
Following MRI, tumours were excised, and MRI-aligned formalin-fixed paraffin-embedded sections were stained with either haematoxylin and eosin (H&E), or picrosirius red, to evaluate cellularity and collagen I & III respectively.
Results and Discussion
All mice developed two tumours spanning from the 4th mammary gland towards the flank, with an average volume of 232±44 mm3. IPH-926 engrafted glands displayed a heterogeneous tumour growth pattern, exhibiting both in situ regions within the ducts (Fig.2, red arrow), alongside invasive regions (blue arrow). ADC showed a bimodal distribution emanating from lobular (ADCmode1=1061x10-6 mm2/s) and infiltrative (ADCmode2=511x10-6 mm2/s) tumour regions respectively (Fig.3A,E). The tumours displayed monomodal, narrow T1, T2 and R2* distributions (Fig.3B-H), with T1-median=1783 ms (T1-IQR=373), T2-median=56 ms (T2-IQR=15) and R2*median=100 s-1 (R2*IQR=63). Higher T1, T2 and R2* values were measured in the lobular in situ regions, as compared to the invasive densely cellular areas (Fig.2), that can be explained by the lower cellular density and higher vascularisation. Tumour R2* was relatively fast compared to other breast cancer models orthotopically propagated in the mammary fat pad [4], consistent with a more haemodynamic vasculature.The selected tumour that underwent MRE displayed two different viscoelastic profiles, with both soft (Fig.4, red) and stiff (blue) regions identifiable. The invasive area showed a dense stroma stained with picrosirius red (Fig.4F, blue), with an associated elevated elasticity, viscosity, and stiffness as compared to the in situ region (red). Interestingly, the tumour stiffness was markedly elevated in this tumour model compared to orthotopic 4T1 tumours grown in the mammary fat pad 4. These results are consistent with relatively high stiffness determined in other stromal dense breast cancer models using MRE, for which fibrillar collagen content is a major determinant 5. Elevated stiffness has also been reported in ILC patients using ultrasound elastography 6.
Conclusion
This study describes the first multiparametric MRI investigation of intraductal xenografts to model late-stage ILC, providing a more clinically relevant system in which to evaluate informative imaging biomarkers of tumour microenvironment and heterogeneity. Compared to in situ regions, invasive regions displayed restricted water diffusion and elevated stiffness, highlighting the utility of DWI and MRE as informative techniques for detecting and assessing ILC invasiveness.Acknowledgements
We acknowledge support from Cancer Research UK grant C16412/A27725 and the European Union Horizon 2020 Research and Innovation Programme (Grant #668039).
References
1. Sflomos, G., et al., Atlas of Lobular Breast Cancer Models: Challenges and Strategic Directions. Cancers, 2021. 13(21): p. 5396.
2. Sflomos, G., et al., A Preclinical Model for ERα-Positive Breast Cancer Points to the Epithelial Microenvironment as Determinant of Luminal Phenotype and Hormone Response. Cancer Cell, 2016. 29(3): p. 407-422.
3. Sflomos, G., et al., Optimized Modeling of Metastatic Triple-Negative Invasive Lobular Breast Carcinoma. Cancers (Basel), 2023. 15(13).
4. Reeves, E.L., et al., Investigating the contribution of hyaluronan to the breast tumour microenvironment using multiparametric MRI and MR elastography. Molecular Oncology, 2023. 17(6): p. 1076-1092.
5. Li, J., et al., Investigating the contribution of collagen to the tumor biomechanical phenotype with noninvasive magnetic resonance elastography. Cancer research, 2019. 79(22): p. 5874-5883.
6. Denis, M., et al., Correlating tumor stiffness with immunohistochemical subtypes of breast cancers: prognostic value of comb-push ultrasound shear elastography for differentiating luminal subtypes. PloS one, 2016. 11(10): p. e0165003.
Figures
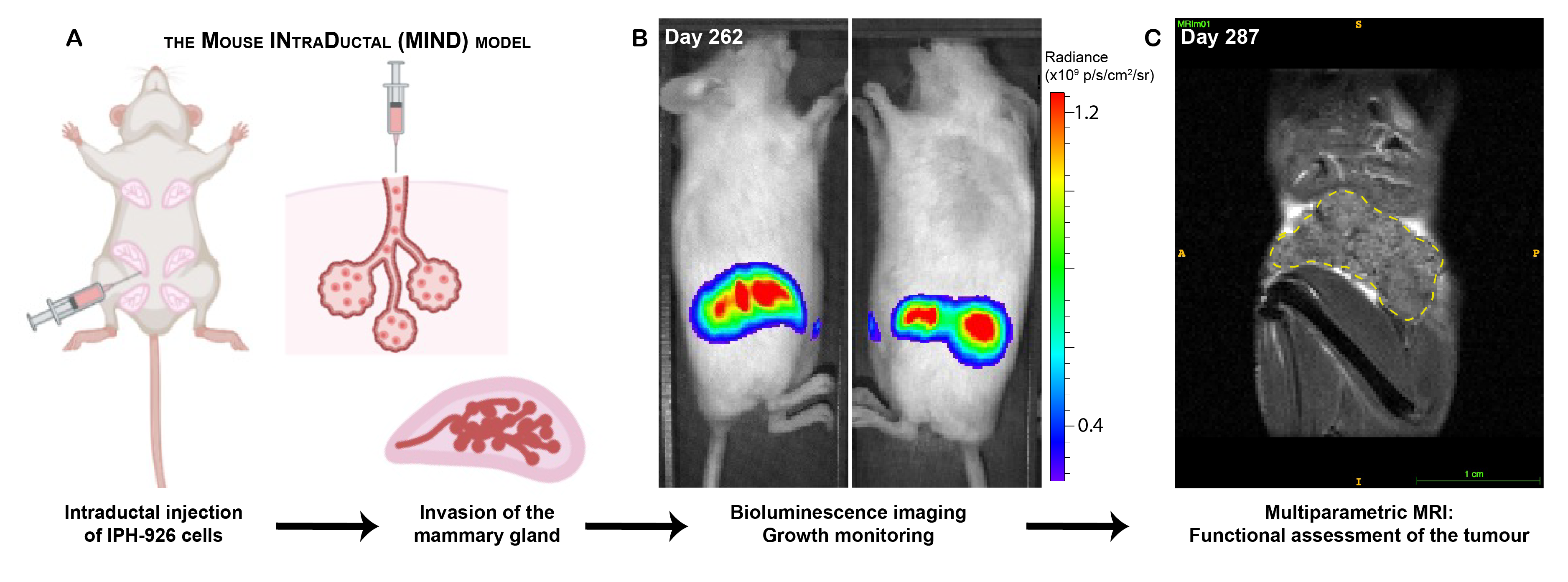
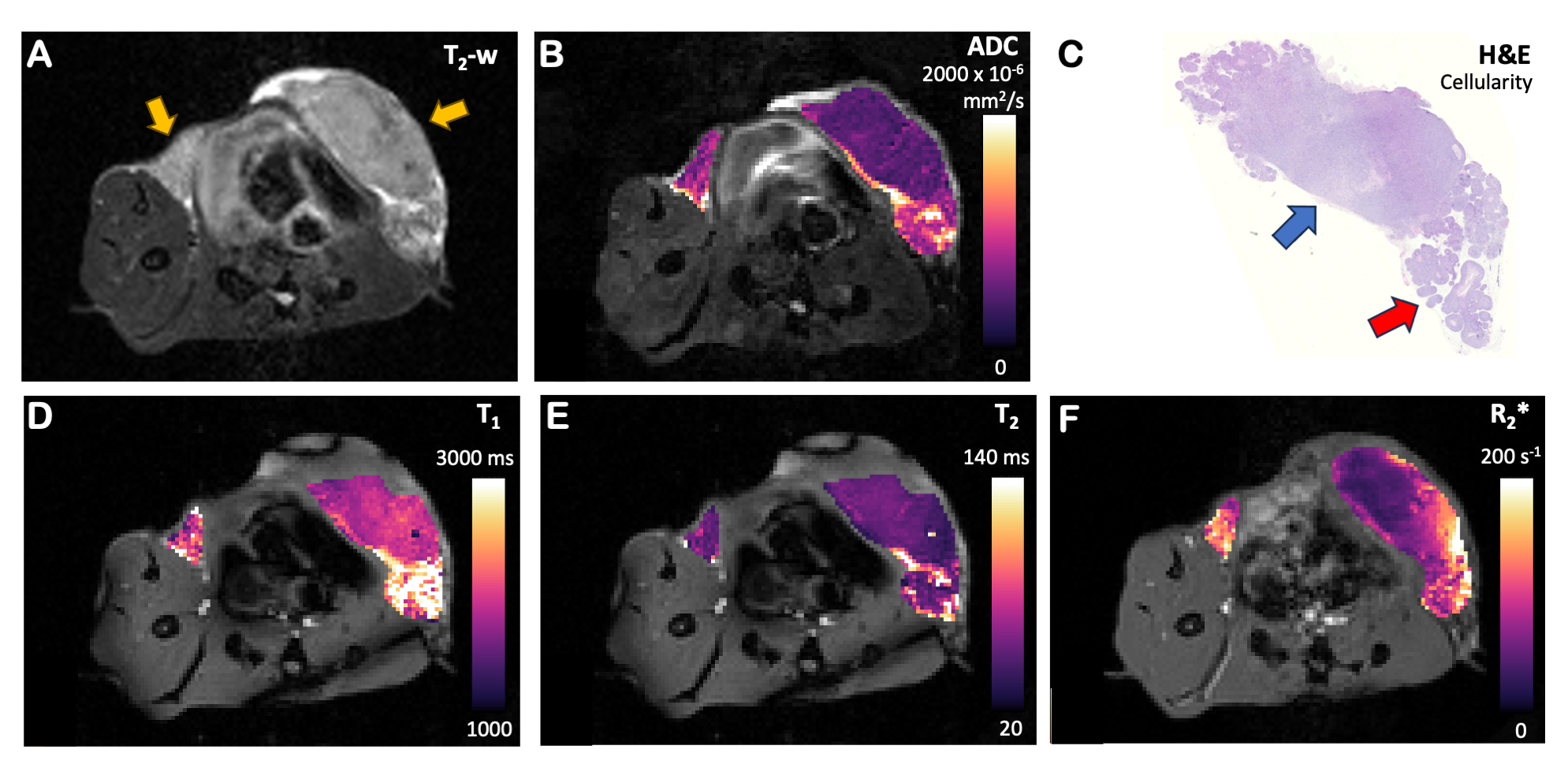
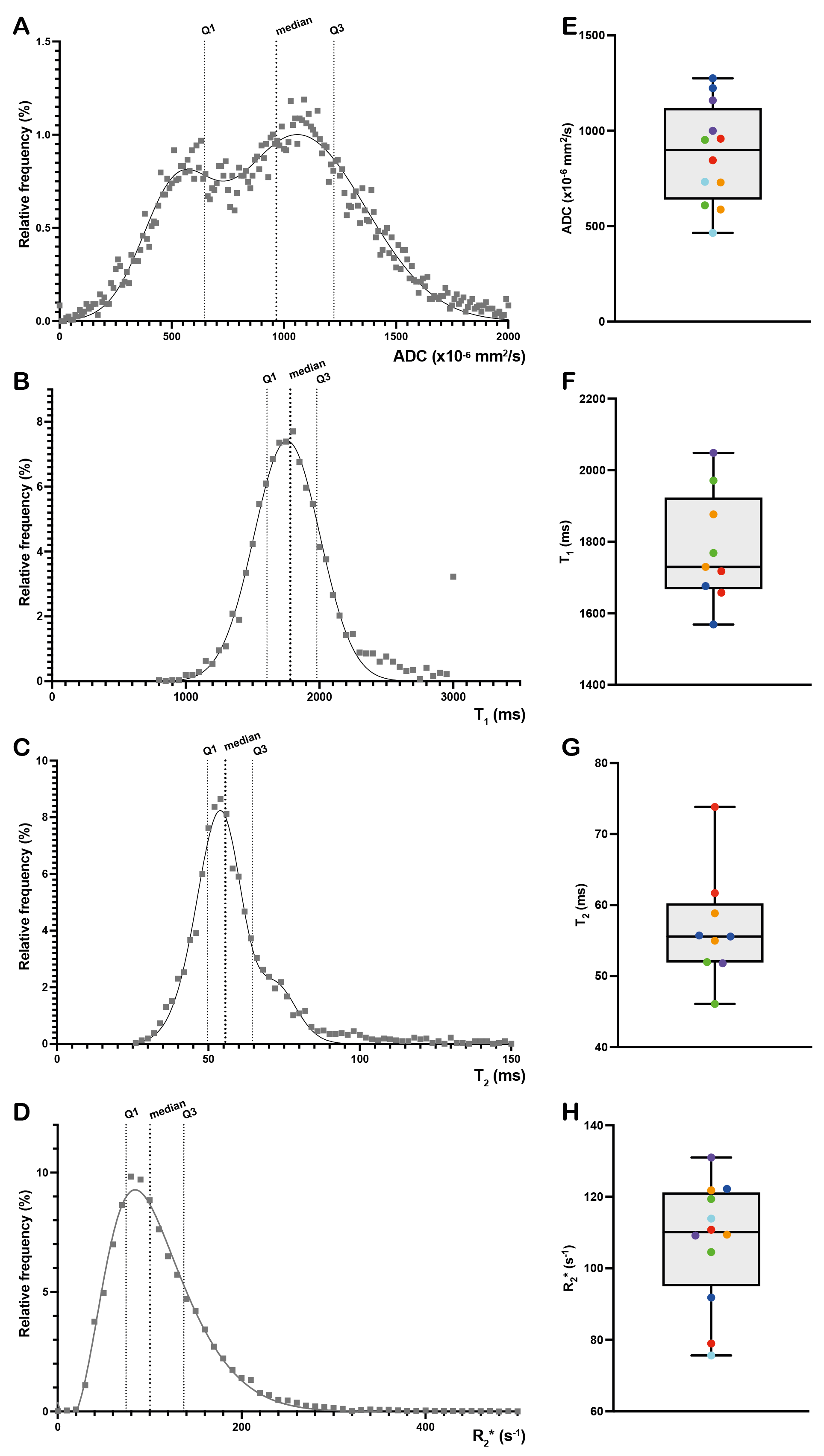
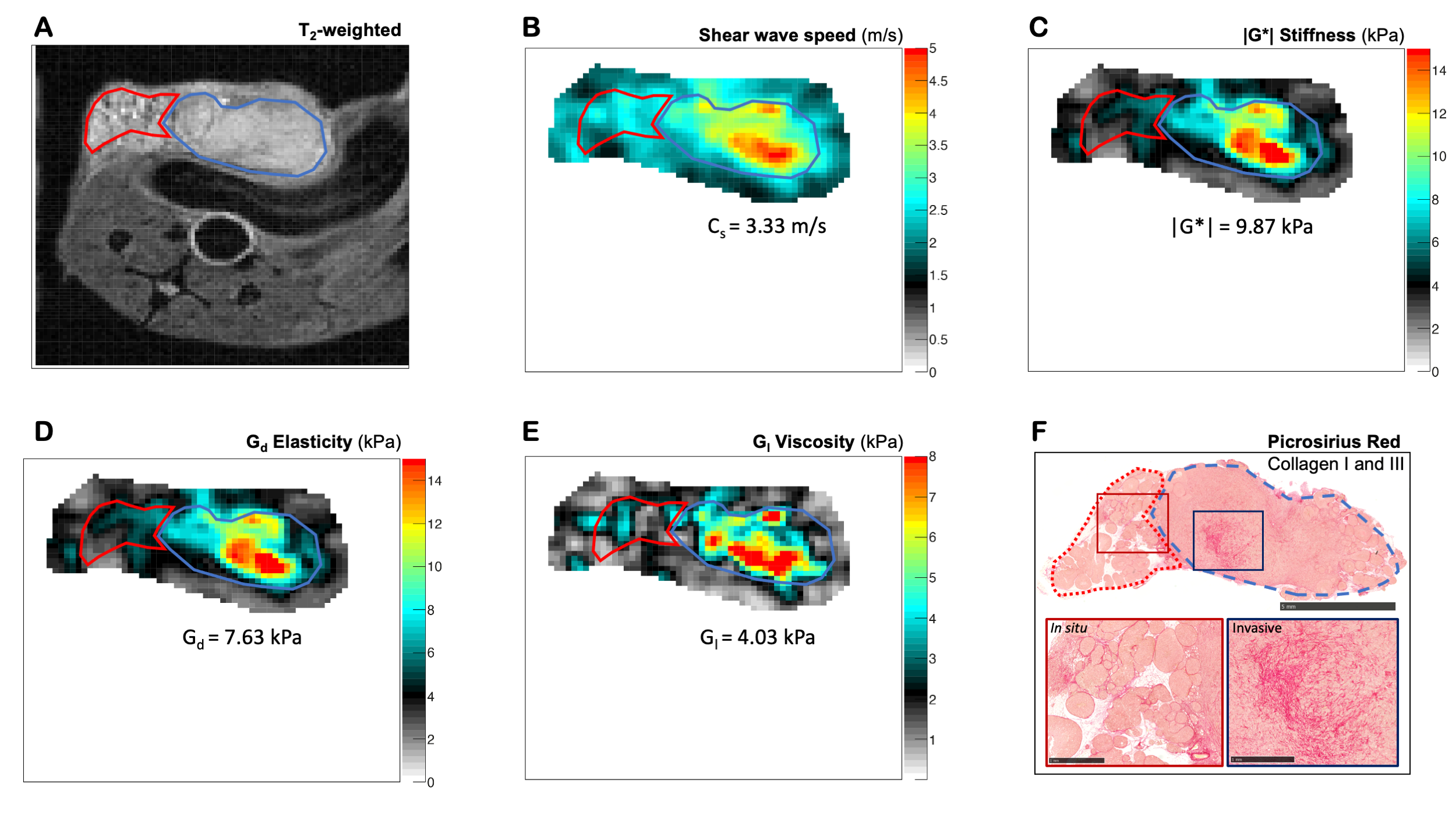
Figure 4: MRE data acquired from the same tumour as in Fig.3. T2-weighted image depicting two different areas of the tumour (A). Shear wave speed (B), stiffness (C), elasticity (D), and viscosity (E) maps showing different properties in the in situ (red) and invasive tumour regions (blue). Median values from the invasive area (blue) are summarised under each parametric map. MRI-aligned picrosirius red stained tissue section is shown in (F), with the in situ lobular region delineated in red and the invasive region delineated in blue, and zoomed-in images from each indicated region.