0686
Accelerated T1ρ,adiab Mapping using Slice Selective Spin-Lock Preparation Pulses (FAST1ρ)1Biomedical Engineering and Imaging Science, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Camberly, United Kingdom
Synopsis
Keywords: Myocardium, Relaxometry
Motivation: T1ρ mapping is a promising non-contrast technique for the assessment of myocardial scar. Myocardial T1ρ mapping techniques commonly acquire multiple images in one breath hold to calculate a single-slice T1ρ map. Recently, non-selective adiabatic pulses have been employed for spin-lock preparation (T1ρ,adiab). FAST1ρ provides a two-fold acceleration for multi-slice myocardial T1ρ,adiab mapping.
Goal(s): To assess the T1ρ,adiab map quality of FAST1ρ compared to a single-slice 2D T1ρ,adiab mapping sequence.
Approach: 10 healthy-volunteers were scanned with FAST1ρ and a single-slice sequence.
Results: FAST1ρ had no significant difference in intra-subject variability or subject-wise precision, to the single-slice sequence, and successfully visualized a myocardial scar.
Impact: FAST1ρ provides a two-fold acceleration for multi-slice myocardial T1ρ,adiab mapping. It has no significant difference in intra-subject variability or subject-wise precision, compared to a single-slice sequence, and shows promise for characterization a myocardial scar.
Introduction
T1ρ mapping is a promising non-contrast technique for the assessment of myocardial scar [1]. Myocardial T1ρ mapping techniques commonly acquire multiple images (with non-selective T1ρ prep) in one breath hold to calculate a single slice T1ρ map. Myocardial scar assessment using T1ρ mapping requires full left ventricular (LV) coverage and a large number of breath holds (BH). Recently, non-selective adiabatic pulses have been employed for spin-lock preparation (T1ρ,adiab)with improved robustness against field inhomogeneities [2]. In this study we developed a novel fast myocardial T1ρ mapping sequence (FAST1ρ) which enables 2x acceleration of full LV coverage using slice selective adiabatic T1ρ,adiab preparation.Methods
A diagram of the FAST1ρ research pulse sequence is shown in Figure 1 and consists of the interleaved acquisition of two slices in one BH. Three T1ρ,adiab -weighted images are acquired per slice, each with an n-heartbeat recovery (n=4/6/8 so that the breath hold time does not exceed 14s). A slice-selective T1ρ,adiab preparation module was developed to minimize disturbances on the magnetization of the other slice. This was based on a series of slice-selective 180° hypersecant (HS) tip down/up pairs (BW=1.5kHz, β=6, B1max=825 Hz, 6x readout slice thickness). 0, 2, and 4 pairs of HS pulses were used to generate T1ρ,adiab prep times of 0, 41, 82ms. Imaging was performed using a bSSFP readout: TE/TR=1.35/188ms, FA=70°, BW=1085Hz/px, matrix=144x256, FOV=323x380mm, slice thickness=8mm, slice gap=40mm, GRAPPA=2 (external ref lines), partial Fourier=7/8). A reference [1] non slice selective sequence (Non-Sel) was also implemented with the same HS pulse (without slice select gradient), the same readout, and an equal number of heartbeats between each T1ρ,adiab-weighted image of the same slice as FAST1p. All imaging was performed at 1.5T (MAGNETOM Sola, Siemens Healthineers).A cardiac T1 phantom [3] was scanned with FAST1ρ and the reference approach (Figure 2). FAST1ρ was repeated twice, with planned slice A (1st repeat) and B (2nd repeat) over the center of the phantom, respectively.
Ten healthy volunteers (6M/4F, Age = 34±8 years, BMI=24±3 kg/m2) were scanned with FAST1ρ (full stack of 12 slices) and Non-Sel (mid, basal and apical slices). AHA 16 segment analysis was performed on the whole image stacks. Segment-wise and subject-wise analysis of mean, precision, and variability of T1ρ,adiab are reported. One patient with acute ST-segment elevation myocardial infarction was imaged with FAST1ρ (one scan of two slices only)
Results
In the phantom experiments (Figure 2), the mean difference between FAST1ρ slice A and B was 2.85±1.65ms or 1.72±0.99%. Example T1ρ,adiab maps, for FAST1ρ and Non-Sel are shown in figure 3. Segment wise healthy volunteer results are shown in Figure 4, subject wise analysis showed FAST1ρ had a significantly lower T1ρ,adiab (125±2ms vs. 136±7ms , p<0.01), not significantly different precision (19.1±2.6ms vs. 21.0±3.3ms , p = 0.10), and not significantly different intra-subject myocardial segment variability (5.5±1.5% vs 6.7±2.0%, p = 0.12) with respect to Non-Sel. The patient showed elevated segmental T1ρ,adiab in the infarct region (AHA segments 1,2,6 T1ρ,adiab= 158±1ms) with lower values in the remote region (AHA segments 4,5 T1ρ,adiab= 131±4ms).Conclusion
FAST1ρ provides a two-fold acceleration for multi-slice myocardial T1ρ,adiab mapping. It has no significant difference in intra-subject variability or subject-wise precision, compared to a 2D T1ρ,adiab mapping sequence based on non-selective adiabatic spin-lock preparations, and shows promise for characterization a myocardial scar.Acknowledgements
Biomedical Research Centre at Guy's and St Thomas' National Health Service (NHS) Foundation Trust; British Heart Foundation (BHF), Grant/Award Numbers:(PG/19/11/34243), (PG/21/10539); Engineering and Physical Sciences Research Council (EPSRC), Grant/Award Number: (EP/R010935/1); King's College London; National Institute for Health Research (NIHR); This research was funded in whole, or in part, by the Wellcome Trust (WT 203148/Z/16/Z).
References
[1] Bustin, A., Witschey, W.R.T., van Heeswijk, R.B. et al. Magnetic resonance myocardial T1ρ mapping. J Cardiovasc Magn Reson 25, 34 (2023).
[2] Coletti, C, Fotaki, A, Tourais, J, et al. Robust cardiac T1ρ mapping at 3T using adiabatic spin-lock preparations. Magn Reson Med. 2023; 90(4): 1363-1379.
[3] Captur, G., Bhandari, A., Brühl, R. et al. T1 mapping performance and measurement repeatability: results from the multi-national T1 mapping standardization phantom program (T1MES). J Cardiovasc Magn Reson 22, 31 (2020).
Figures
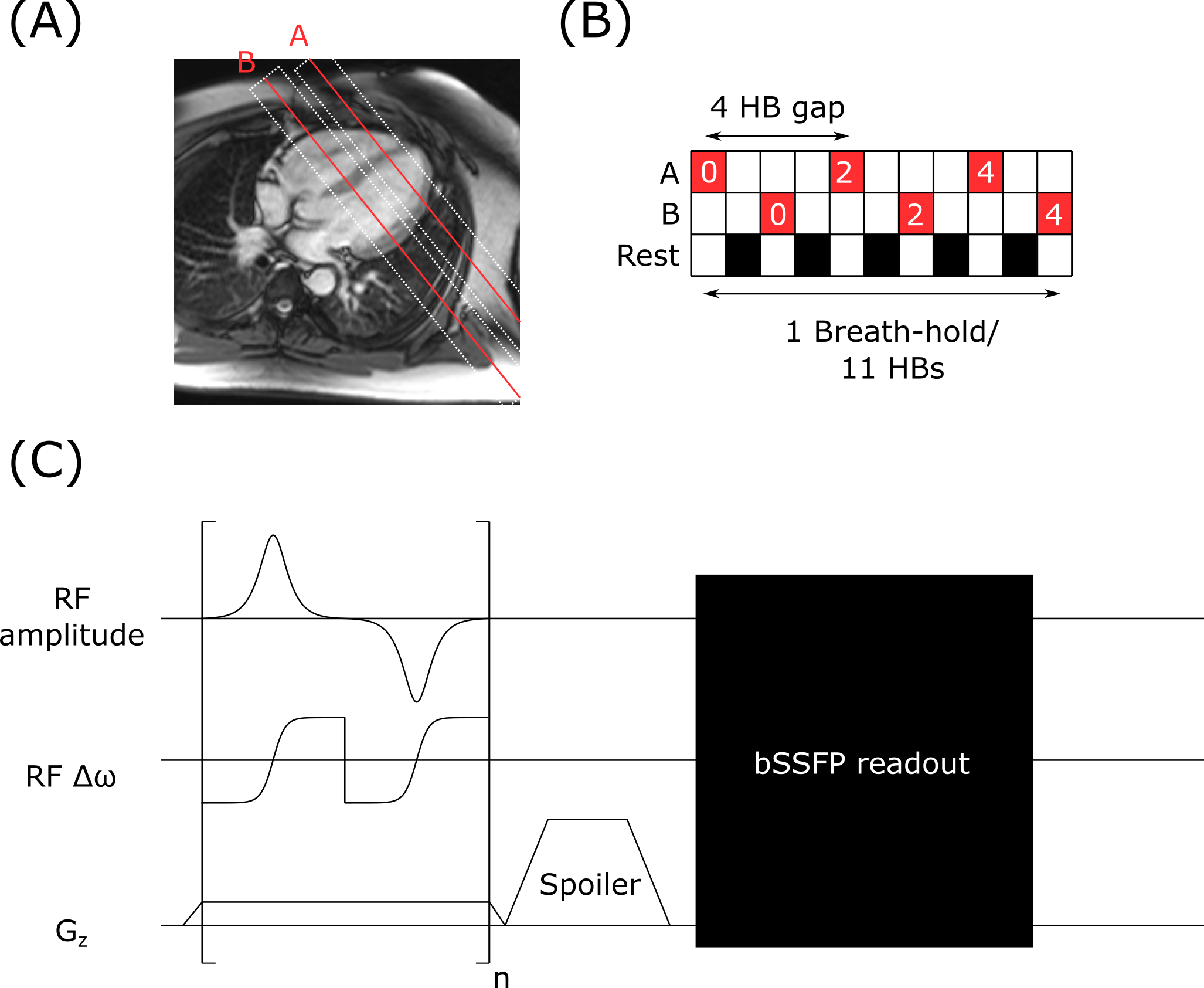
Figure 1. Fast1ρ diagram. (A) Two slices are acquired in a single breath hold, slice thickness of the T1ρ,adiab preparation is shown by the white dashed boxes. (B) Acquisition of the two slices is interleaved to allow recovery between T1ρ,adiab preparation pulses of the same slice. The number of T1ρ,adiab prep modules (n) is shown in white. (C) Pulse sequence diagram showing the slice selective T1ρ prep module and readout.
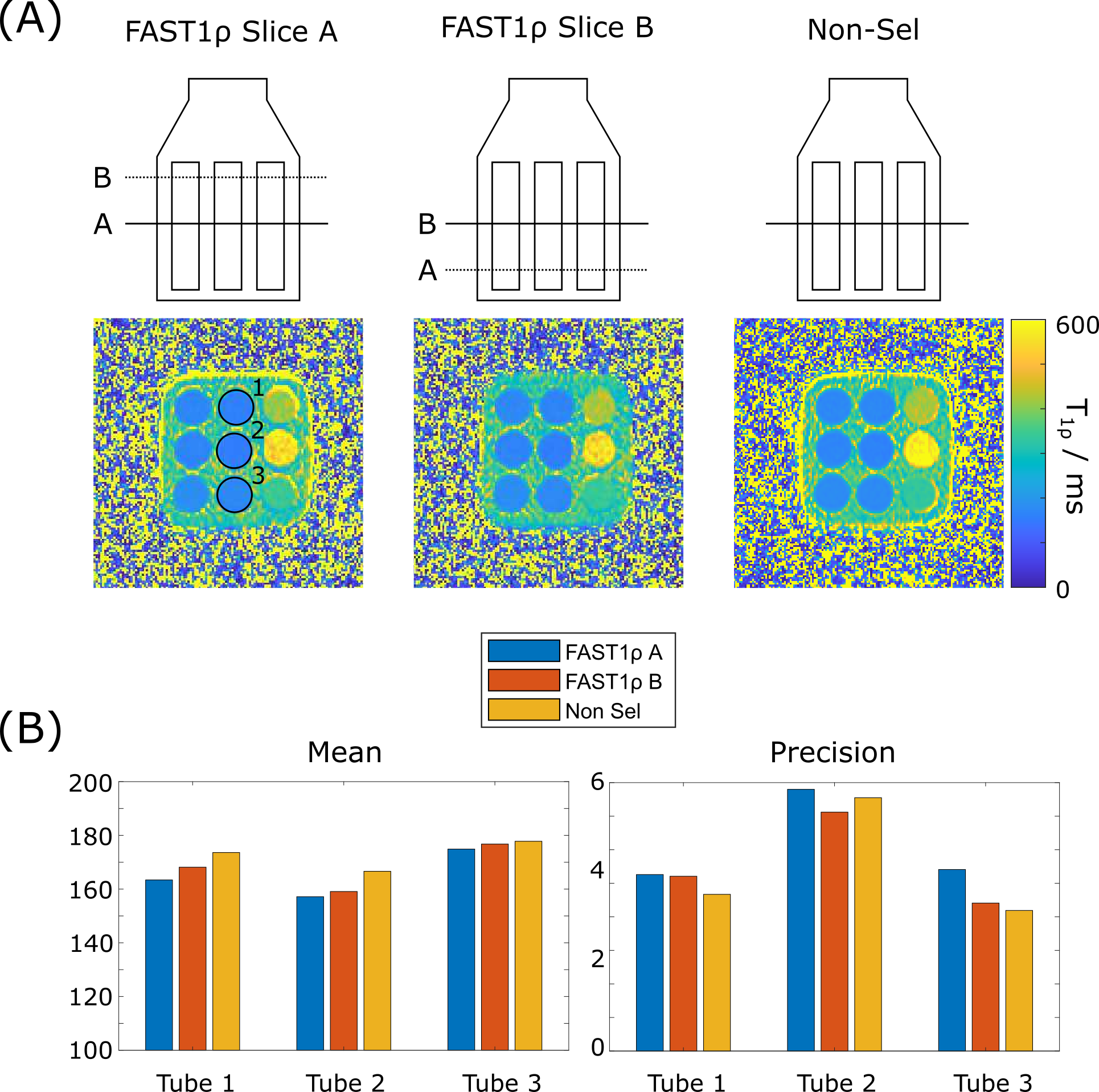
Figure 2. Results for the phantom experiment. (A) Example images, acquired with FAST1ρ slice A and B and Non-Sel, showing the same plane through the T1 phantom. (B) Bar charts of mean and precision values for the three myocardium tubes indicated in (A).
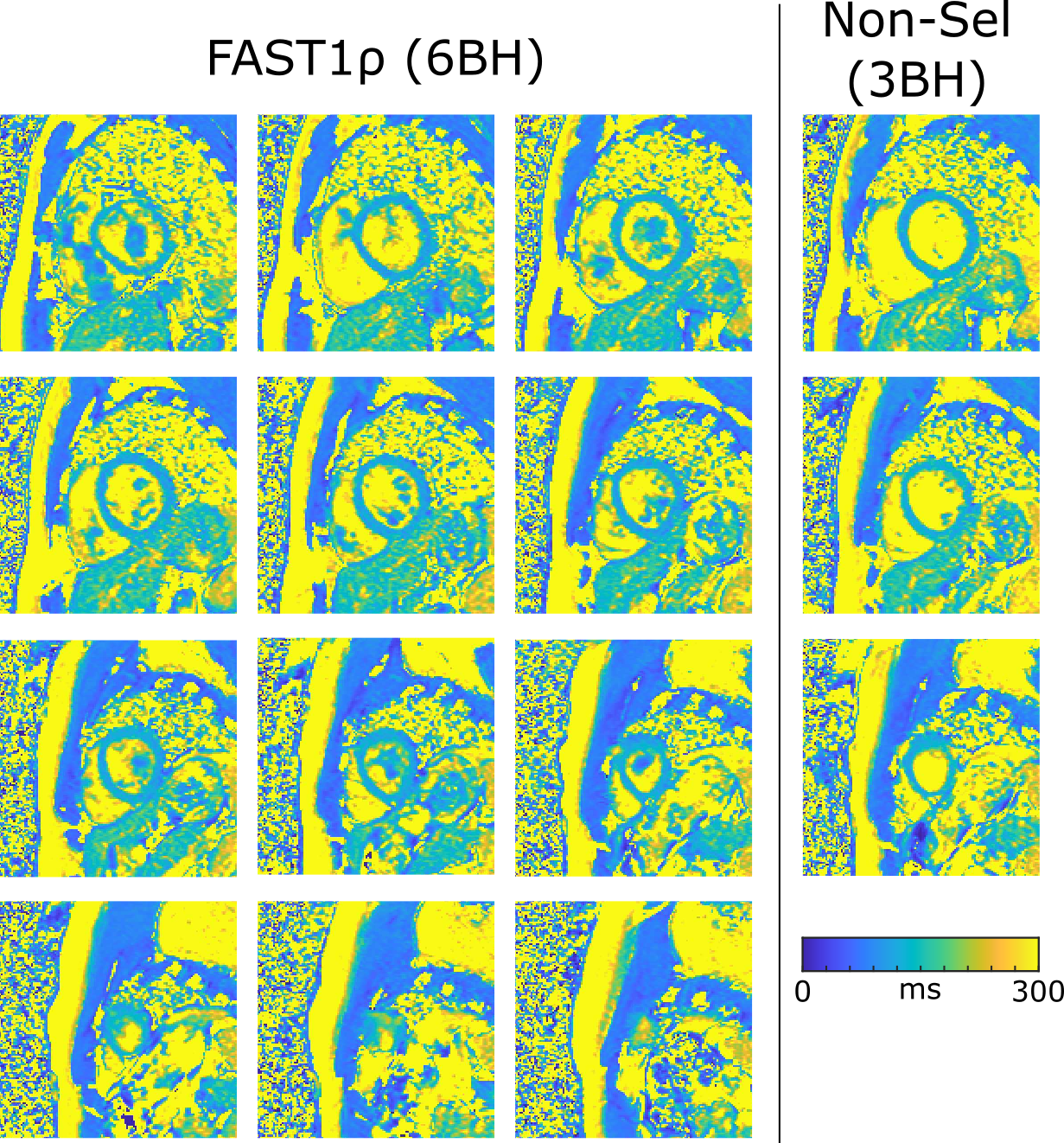
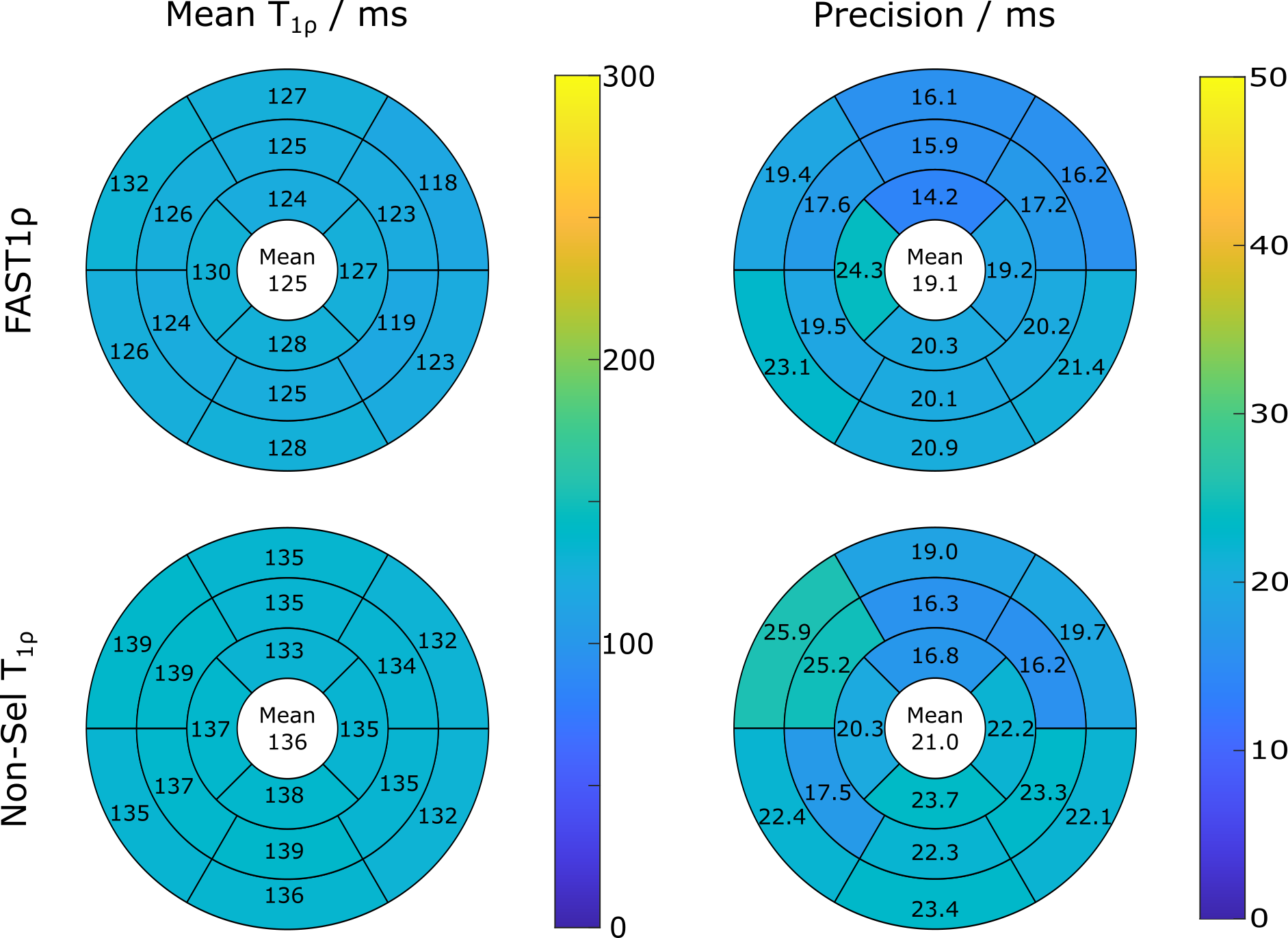
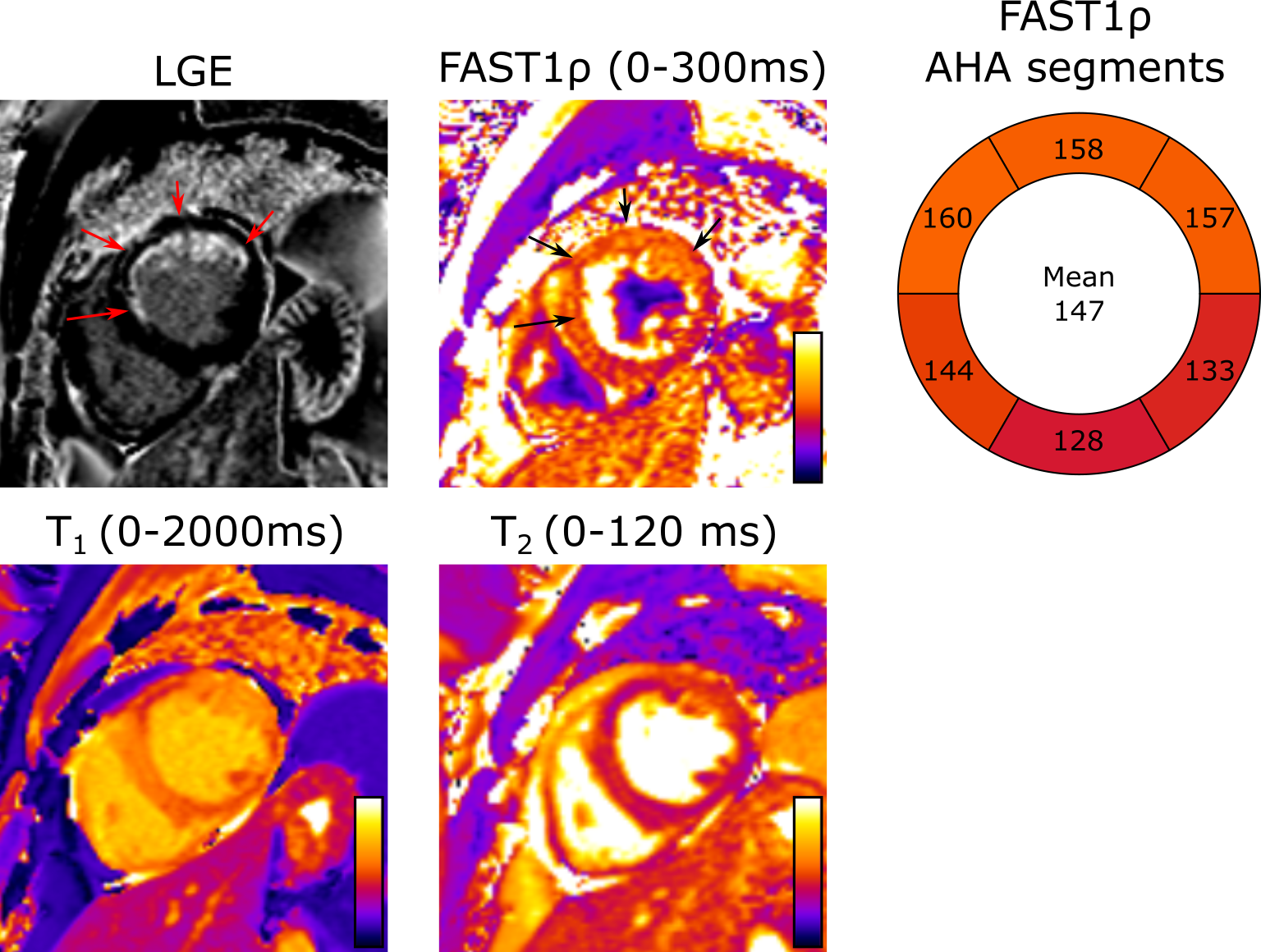
Figure 5. LGE, T1ρ,adiab (acquired with FAST1ρ), T1 and T2 maps of a patient with ST-segment elevated myocardial infarction. T1ρ,adiab is elevated above the healthy cohort mean value in the region of the infarct.