0685
3D free-breathing simultaneous myocardial T1 and T1ρ mapping with B1+ correction and subject-specific non-rigid motion correction1School of Biomedical Engineering, ShanghaiTech University, Shanghai, China, 2Shanghai Clinical Research and Trial Center, Shanghai, China, 3United Imaging Healthcare, Shanghai, China, 4UIH America, Inc., Houston, TX, United States, 5King's College London, London, United Kingdom, 6School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Multi-parametric mapping is useful for comprehensive myocardial tissue characterization. However, 3D free-breathing cardiac multi-parametric mapping faces challenges.
Goal(s): Develop a 3D free-breathing cardiac multi-parametric mapping framework that is robust to confounders of motion, fat and field inhomogeneities and validate it for joint T1 and T1ρ mapping at 3T.
Approach: A subject-specific respiratory motion model was constructed to enable intra-bin 3D translational and inter-bin non-rigid motion correction. B1+ inhomogeneities were corrected with optimized dual-flip-angle strategy. A dual-echo Dixon readout was adopted for water-only mapping.
Results: The proposed technique achieved good agreement with conventional techniques in measuring T1 and T1ρ in phantoms and healthy subjects.
Impact: A novel framework was proposed for efficient 3D free-breathing multi-parametric mapping. The 3D simultaneous cardiac T1 and T1ρ mapping technique with scan time of ~ 5 minutes may serve as an efficient tool for diagnosing ischemic and non-ischemic cardiomyopathies.
Introduction
Native T1 is a well-recognized parameter for detecting various cardiomyopathies. For example, increase in free water or amyloid in the myocardium leads to increased T1, while iron deposition or Fabry disease causes reduced T11. T1ρ a longitudinal relaxation time in a rotating frame, depicting the process of the transverse magnetization relaxing along a spin-lock (SL) pulse with a relatively low frequency of several hundred Hz. It is sensitive to macromolecule content changes, and has been used to detect focal and diffuse myocardial fibrosis2,3. For obtaining co-registered T1 and T1ρ maps and improving acquisition efficiency, there is emerging research interest in developing joint T1 and T1ρ mapping techniques4,5. However, 3D free-breathing multi-parameter mapping of the heart is challenging as confounders such as motion, fat and field inhomogeneities affect estimation accuracy. We develop a novel technique to address these challenges, which is characterized by subject-specific non-rigid respiratory motion correction, spin history B1+ correction and Dixon readout for water-only T1 and T1ρ measurements at 3T.Methods
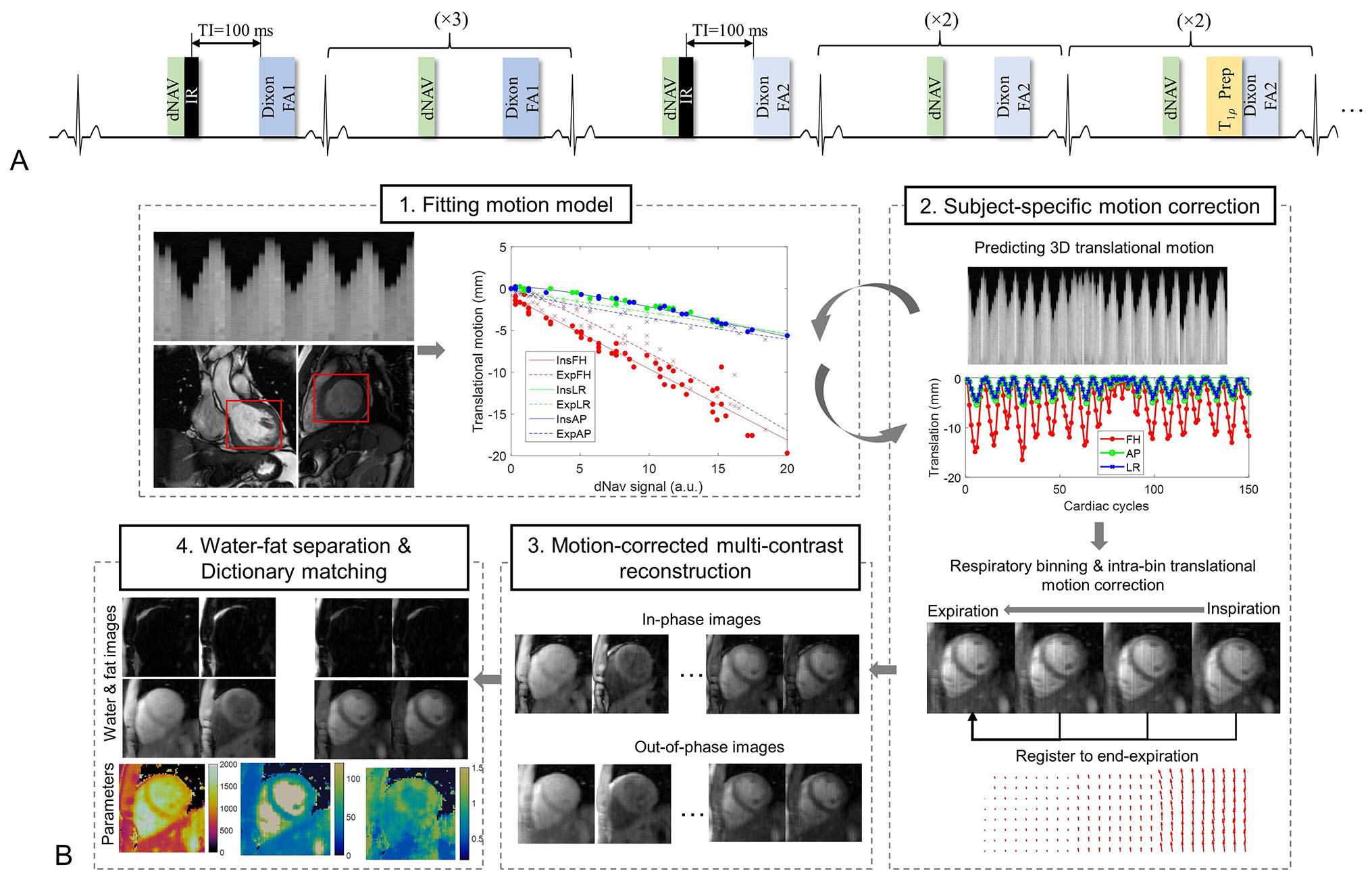
The proposed technique adopts ECG-triggered diastolic acquisition with dual-echo Dixon readout. The repetitively acquired module consists of 9 cardiac cycles (Fig. 1A), where the inversion recovery (IR) pulse is performed at the first and fifth cardiac cycle and the T1ρ preparation with different spin-lock times (TSL) is performed at the last two cardiac cycles. For B1+ sensitization, the flip angle after the second IR is varied. The dual-flip-angle strategy was optimized with numerical simulations. A diaphragmatic navigator (dNav)6 is performed in each heartbeat before the preparation pulse, which is used as a surrogate for the subject-specific motion model as explained below.Subject-specific non-rigid motion correction
The subject-specific motion model relating the respiration-induced motion of the heart along the foot-head, anterior-posterior and left-right directions to the dNav signal (Fig. 1B) was constructed with a short training scan acquiring dNav and a single-shot cardiac image in each heartbeat7. The trained motion model can be used to calculate the 3D translational motion of the heart in the 3D acquisition. Then, the multi-contrast data was binned into four respiratory states based on the estimated foot-head motion. The intra-bin 3D translational motion was corrected using the calculated motion parameters. The non-rigid inter-bin motion was estimated by registering the bin images and corrected in the under-sampled multi-contrast reconstruction8: $$argmin_{x}\sum_b\parallel E_{b}T_{b}x-y_{b} \parallel_2^2+\lambda\sum_p\parallel T_{p}(x) \parallel_*$$where x indicates the multi-contrast images, Tb is the motion-warping operator for bin b, Eb is the encoding operator and Tp selects the local and non-local image patches around pixel p for patch-based low-rank regularization9, ||.||* calculates the nuclear norm. λ is the regularization parameter.
Water-only parameter mapping
After multi-contrast reconstruction, the water-fat separation was performed with the B0-NICEbd algorithm10. Then, dictionary matching was performed to estimate T1 and T1ρ from the water-only images with the dictionary simulated for a range of T1 and T1ρ values for each subject.
Imaging experiments
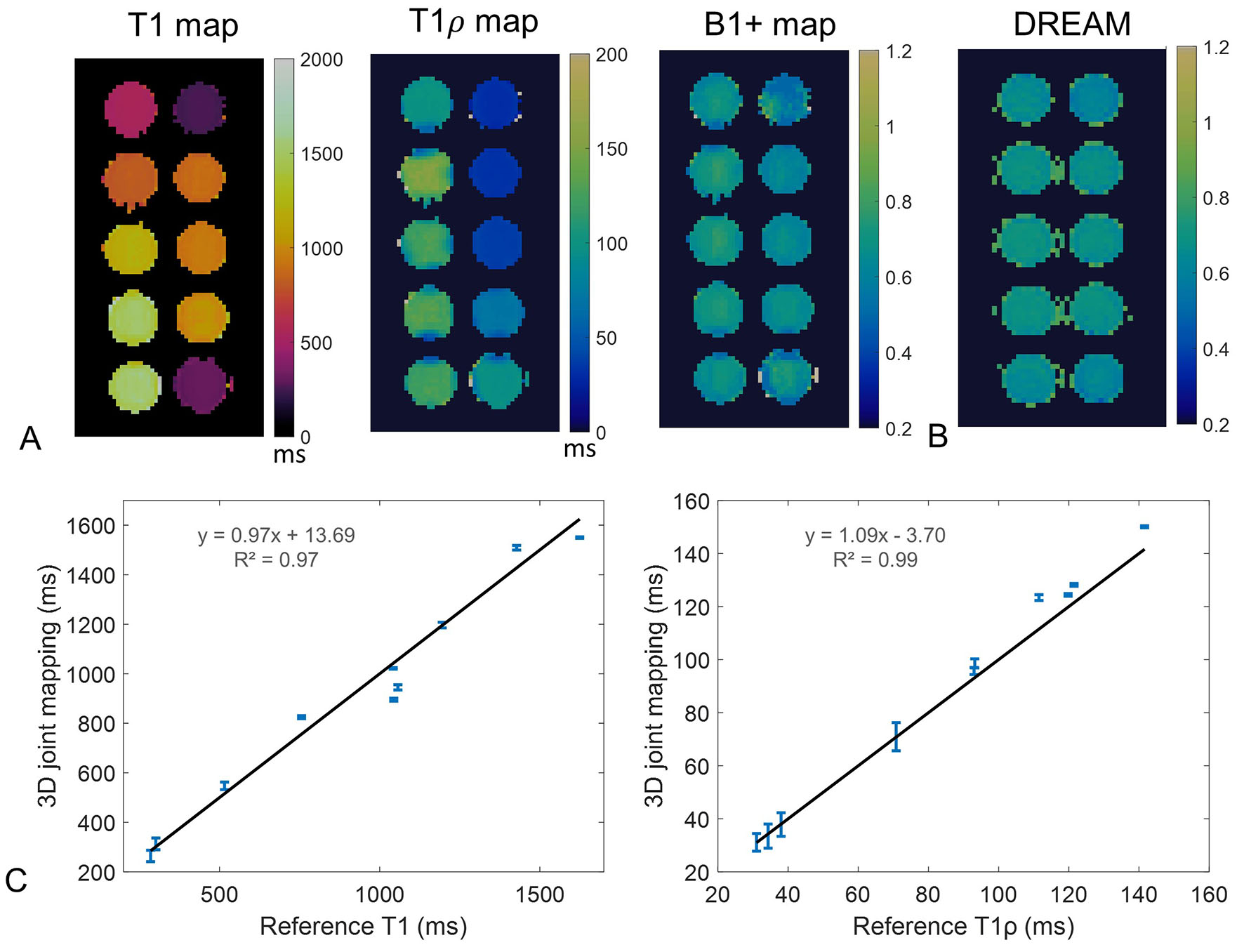
The imaging acquisitions were performed in a 3T MR scanner. Prior to the 3D imaging, the training scan was performed in the coronal and sagittal view, acquiring 50 single-shot images for each view. Then, the 3D mapping acquisition was performed in the short-axis view with FOV=320×300×144mm, voxel size=2×2×4mm, TR/TE1/TE2=4.21/1.12ms/2.24ms, flip angle=2/16°, TI=100ms, TSL=30/50ms, spin lock frequency=350Hz, number of segments=26-30, 4x variable-density Cartesian undersampling11,12. For comparison, the IR spin echo, T1ρ-prepared gradient echo3 and DREAM B1+ mapping13 techniques were performed to obtain the reference values of phantoms. Five healthy subjects were recruited with IRB approval and written informed consent, for whom the 2D breath-hold MOLLI14 and T1ρ-bSSFP15 were performed along with the 3D mapping technique.
Results
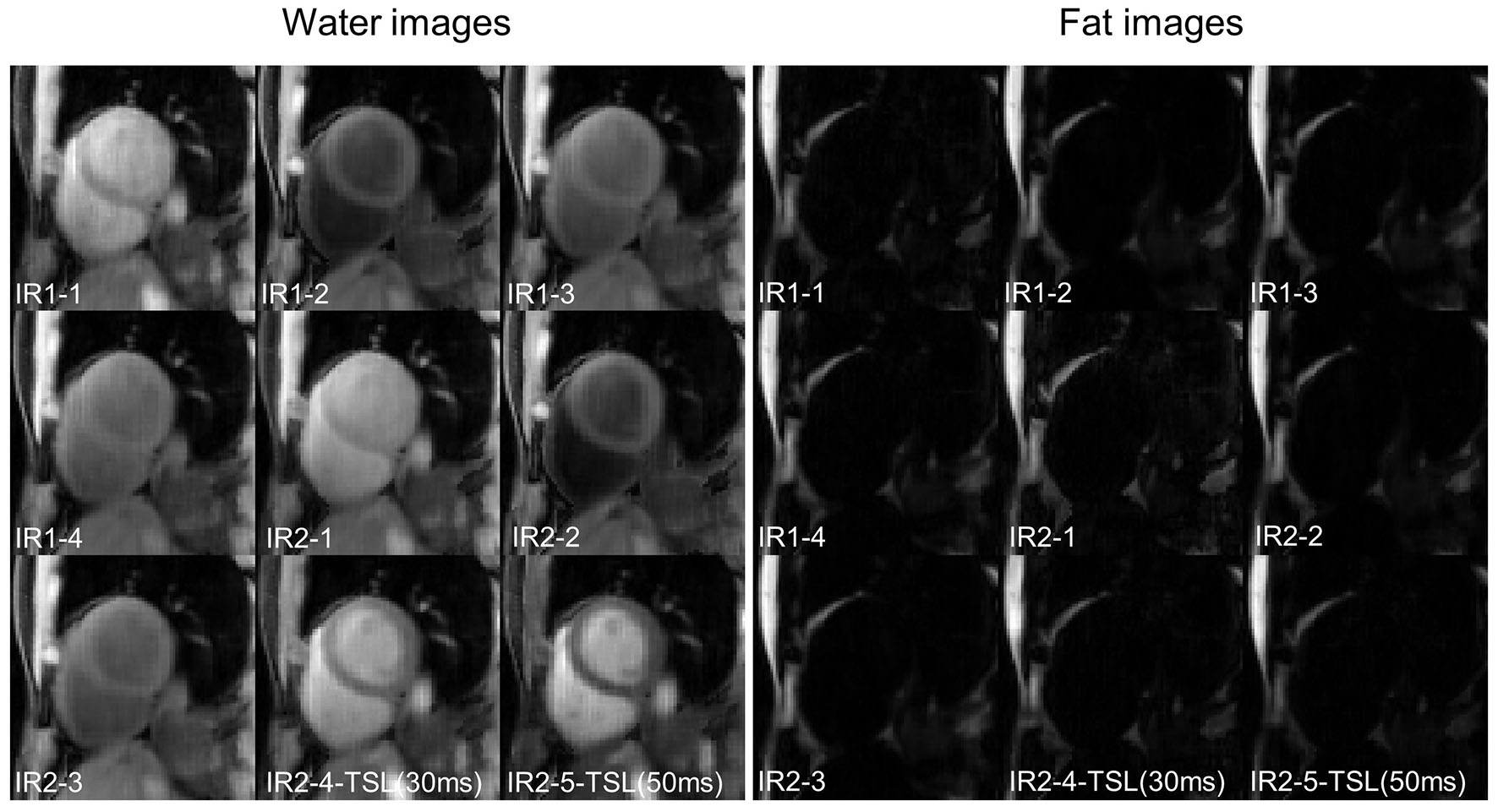
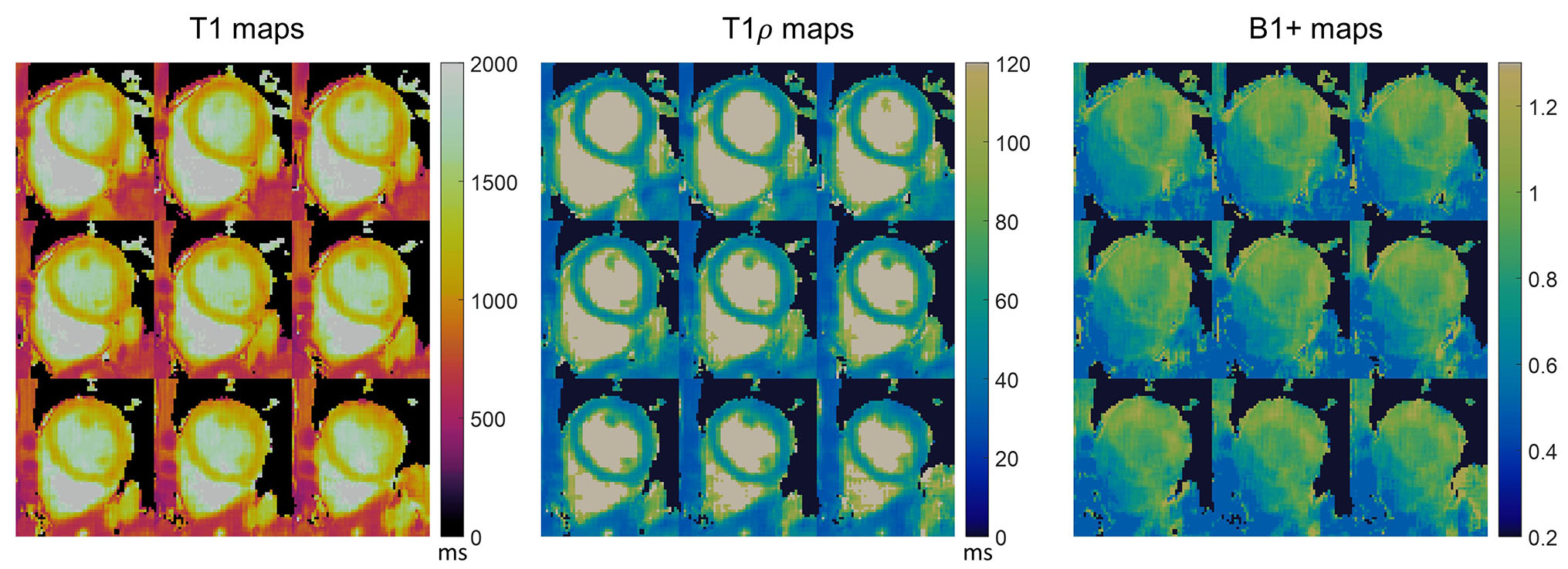
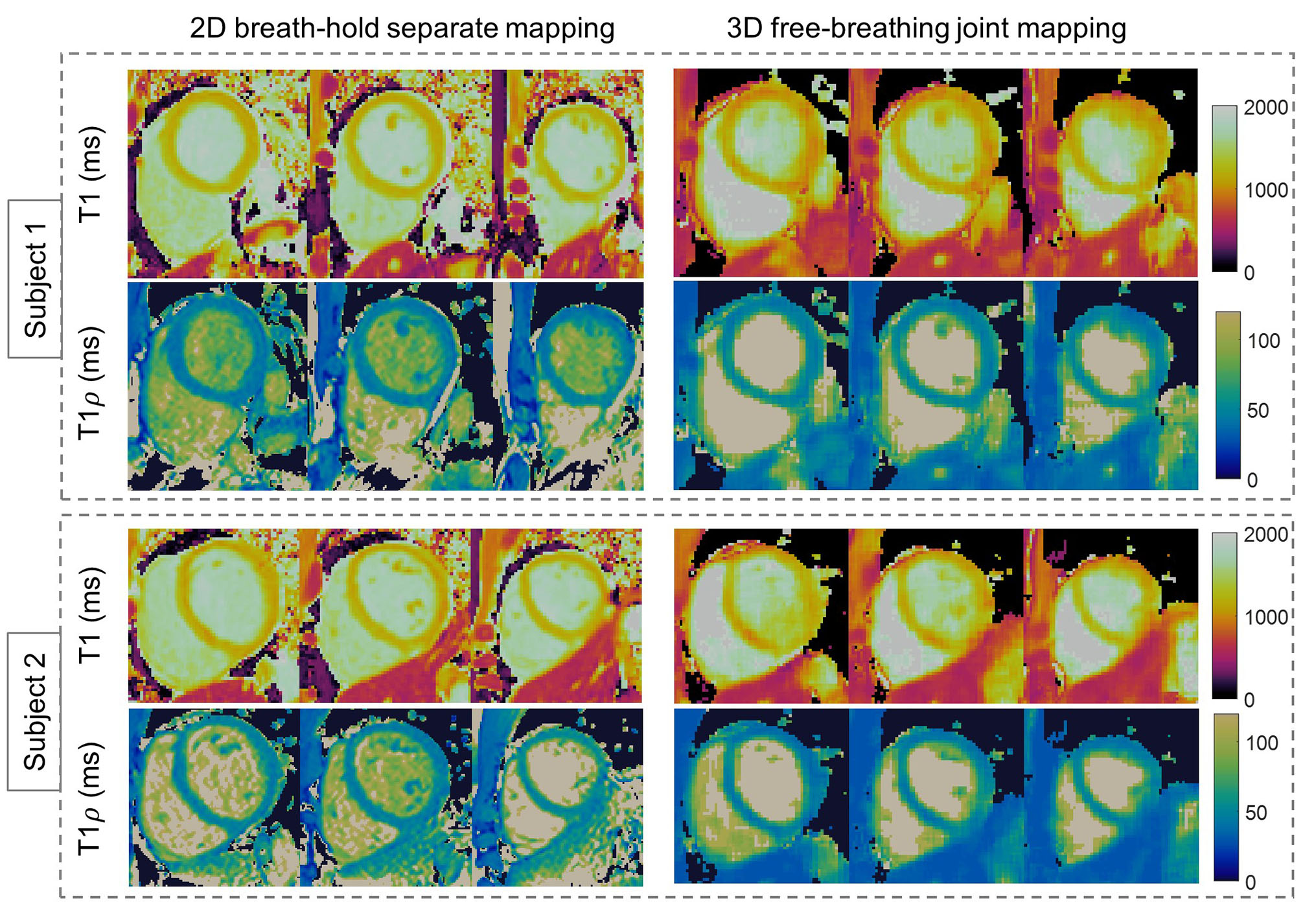
The phantoms results are shown in Fig. 2, indicating good estimation accuracy of the proposed technique. Figure 3 shows example water/fat separation for the 9 contrasts. Water-only 3D parameter maps of the same subject are visualized in Fig. 4. The T1 and T1ρ maps are overall homogeneous, while for B1+ map, the septal myocardium exhibits lower values than the lateral region. Figure 5 compares the 3D maps and 2D breath-hold maps for two subjects, where slight blurring can be observed for the 3D technique, which may be caused by residual respiratory motion or regularized reconstruction. The measurements of the proposed and breath-hold techniques are comparable (septal T1: 1125.1±23.3ms vs. 1159.6±42.0ms; septal T1ρ: 46.9±4.7ms vs. 46.1±1.0ms). The acquisition time of the proposed technique is ~5 minutes.Discussion & Conclusion
The 3D simultaneous cardiac T1 and T1ρ mapping technique with robustness to confounders of motion, fat and field inhomogeneities achieved good mapping quality in phantom and healthy subjects, representing as a novel framework for efficient 3D free-breathing cardiac multi-parametric mapping.Acknowledgements
No acknowledgement found.References
1. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19(1):75.
2. Han Y, Liimatainen T, Gorman RC, Witschey WR. Assessing Myocardial Disease Using T1rho MRI. Curr Cardiovasc Imaging Rep 2014;7(2):9248.
3. Qi H, Bustin A, Kuestner T, Hajhosseiny R, Cruz G, et al. Respiratory motion-compensated high-resolution 3D whole-heart T1rho mapping. J Cardiovasc Magn Reson 2020;22(1):12.
4. Velasco C, Cruz G, Lavin B, Hua A, Fotaki A, et al. Simultaneous T1 , T2 , and T1rho cardiac magnetic resonance fingerprinting for contrast agent-free myocardial tissue characterization. Magn Reson Med 2022;87(4):1992-2002.
5. Crabb M, Kunze K, Velasco C, Fotaki A, Munoz C, et al. 3D joint T1/T1ρ mapping and water-fat imaging for contrast-agent free myocardial tissue characterization. Proc. Intl. Soc. Mag. Reson. Med. 30 (2022); London, UK.
6. Stuber M, Botnar RM, Danias PG, Kissinger KV, Manning WJ. Submillimeter three-dimensional coronary MR angiography with real-time navigator correction: comparison of navigator locations. Radiology 1999;212(2):579-587.
7. Bush MA, Ahmad R, Jin N, Liu Y, Simonetti OP. Patient specific prospective respiratory motion correction for efficient, free-breathing cardiovascular MRI. Magn Reson Med 2019;81(6):3662-3674.
8. Cruz G, Qi H, Jaubert O, Kuestner T, Schneider T, et al. Generalized low-rank nonrigid motion-corrected reconstruction for MR fingerprinting. Magn Reson Med 2022;87(2):746-763.
9. Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, et al. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med 2019;81(6):3705-3719.
10. Liu J, Peters DC, Drangova M. Method of B0 mapping with magnitude-based correction for bipolar two-point Dixon cardiac MRI. Magnetic Resonance in Medicine 2017;78(5):1862-1869.
11. Cheng JY, Zhang T, Ruangwattanapaisarn N, Alley MT, Uecker M, et al. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J Magn Reson Imaging 2015;42(2):407-420.
12. Prieto C, Doneva M, Usman M, Henningsson M, Greil G, et al. Highly Efficient Respiratory Motion Compensated Free-Breathing Coronary MRA Using Golden-Step Cartesian Acquisition. J Magn Reson Imaging 2015;41(3):738-746.
13. Nehrke K, Versluis MJ, Webb A, Börnert P. Volumetric Mapping of the Brain at 7T Using DREAM. Magnetic Resonance in Medicine 2014;71(1):246-256.
14. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, et al. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T-1 mapping of the heart. Magn Reson Med 2004;52(1):141-146.
15. Qi H, Lv Z, Hu J, Xu J, Botnar R, et al. Accelerated 3D free-breathing high-resolution myocardial T(1rho) mapping at 3 Tesla. Magn Reson Med 2022;88(6):2520-2531.
Figures