0682
Improved 3D multi-contrast CMR for high-quality anatomical imaging and joint T1/T2 mapping in a single free-breathing scan1Department of Diagnostic and Interventional Radiology, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany, 2Institute for Advanced Study, Technical University of Munich, Munich, Germany, 3School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 4Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 5Millenium Institute for intelligent Healthcare Engineering, Santiago, Chile, 6MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 7School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Myocardium, Heart, Bright- and black blood imaging, T1/T2 mapping
Motivation: Cardiovascular MR (CMR) provides comprehensive assessment of heart disease. However, conventional CMR examinations involve multiple sequential 2D acquisitions under breath-hold conditions.
Goal(s): To devise and develop a novel 3D free-breathing sequence for simultaneous assessment of cardiovascular anatomy via bright- and black-blood imaging and myocardial tissue quantification in a single scan.
Approach: Implementation of an improved iNAV-based 5-heartbeat interleaved sequence (proACTION) with distinct IR and T2 preparation modules and non-rigid motion correction for robust and accurate myocardial tissue quantification.
Results: proACTION provides accurate delineation of cardiac and vascular structures, while demonstrating good agreement with conventional mapping sequences in healthy subjects.
Impact: Comprehensive 3D whole-heart tissue characterization and clinically relevant anatomical information can be obtained in an efficient, free-breathing, and easier to use one-click-scan with the proposed proACTION approach.
Introduction
Cardiovascular MR (CMR) is a well-established imaging modality for a comprehensive evaluation of the structure and function of the heart1. In addition, myocardial T1 and T2 mapping contribute valuable clinical insights into a variety of cardiovascular diseases2. However, typical clinical protocols involve several sequential 2D acquisitions in different orientations under multiple breath-holds leading to long and unpredictable examination times. Recently, we have proposed a free-breathing motion-compensated 3D sequence for simultaneous Assessment of whole-heart Cardiovascular anaTomy via bright- and black-blood Imaging3 and myocardial tissue quantificatiON (ACTION4). In this study, we introduce its imPROved version for more robust and accurate estimation of T1 values – proACTION.Methods
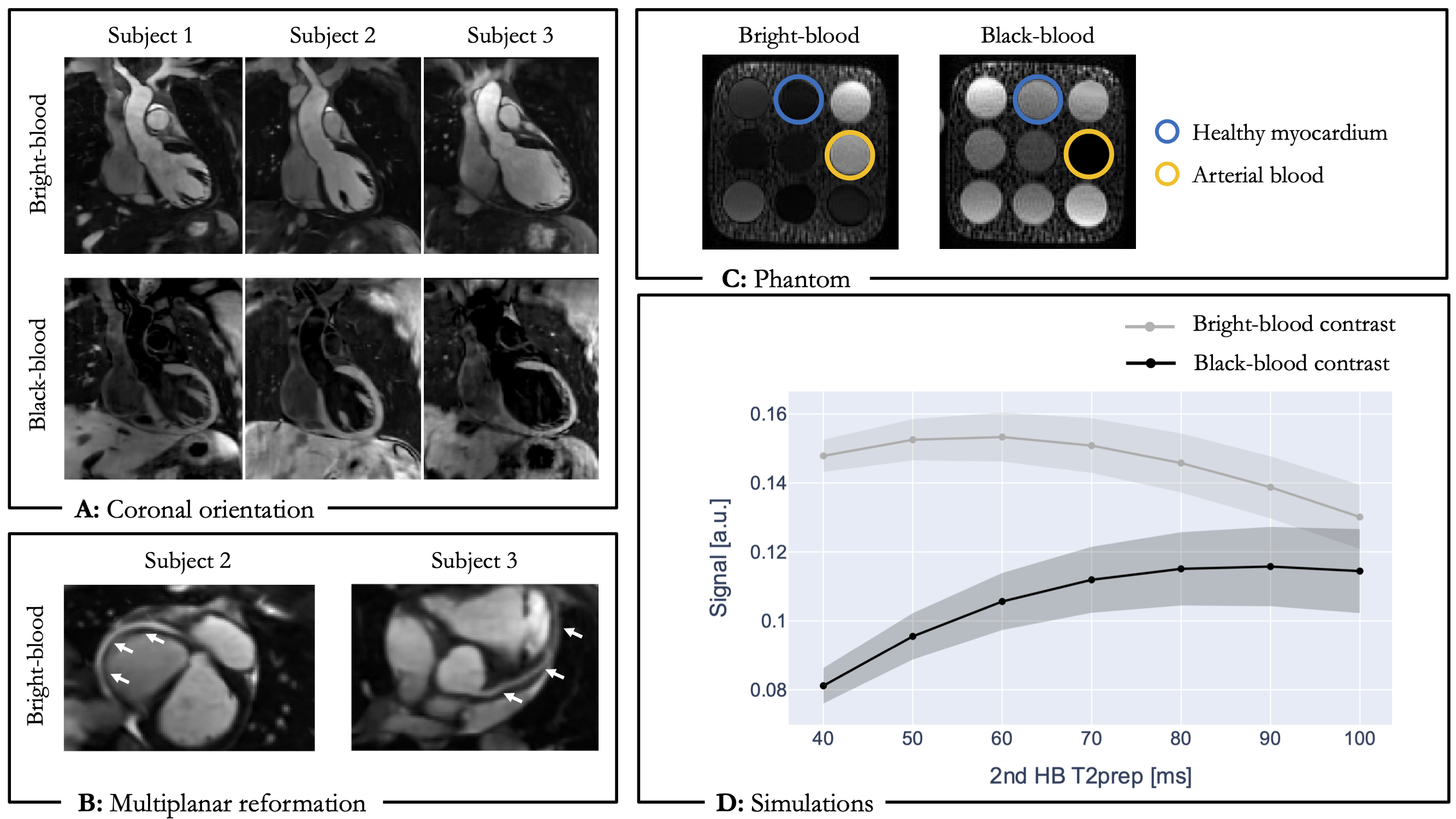
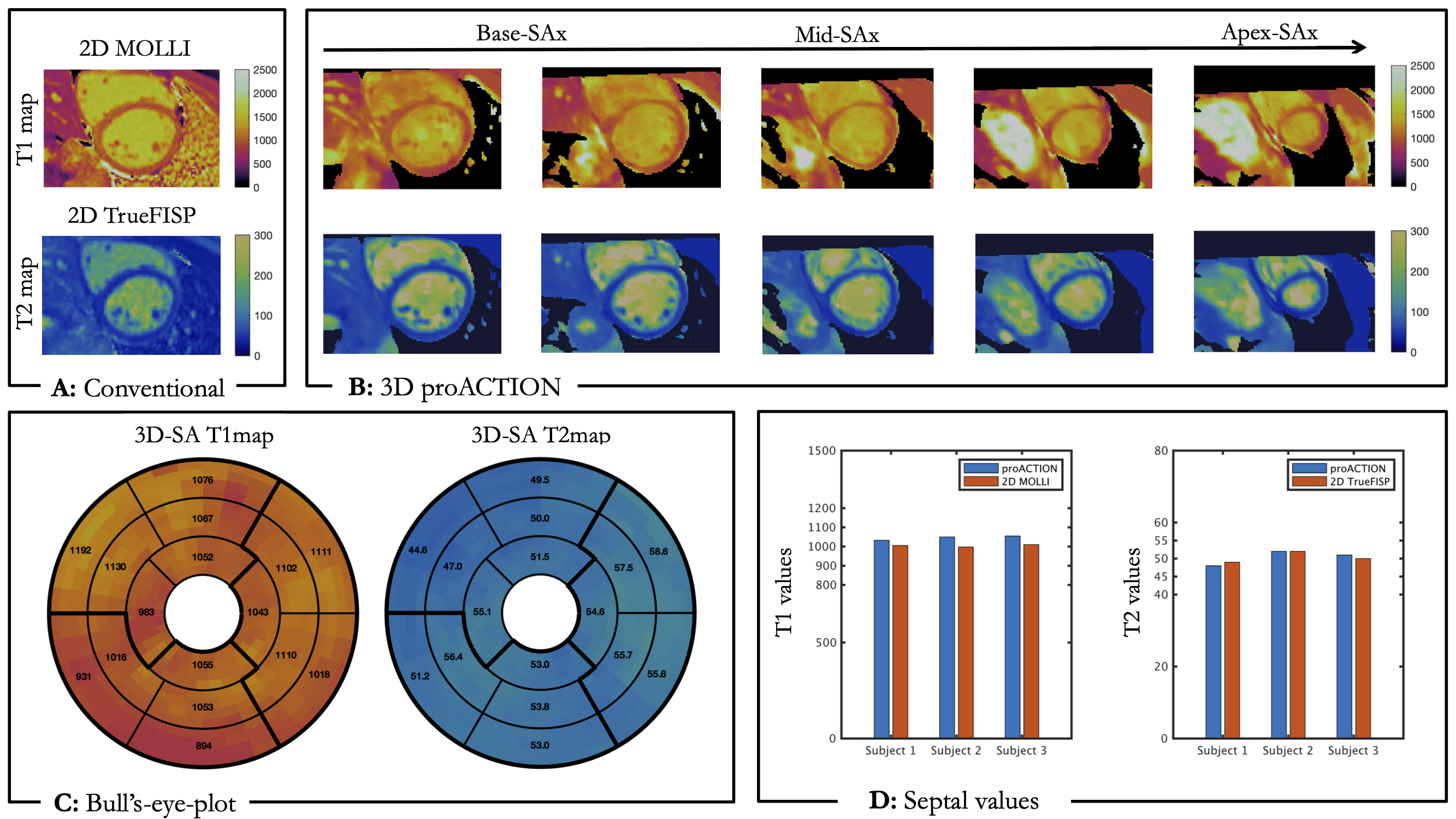
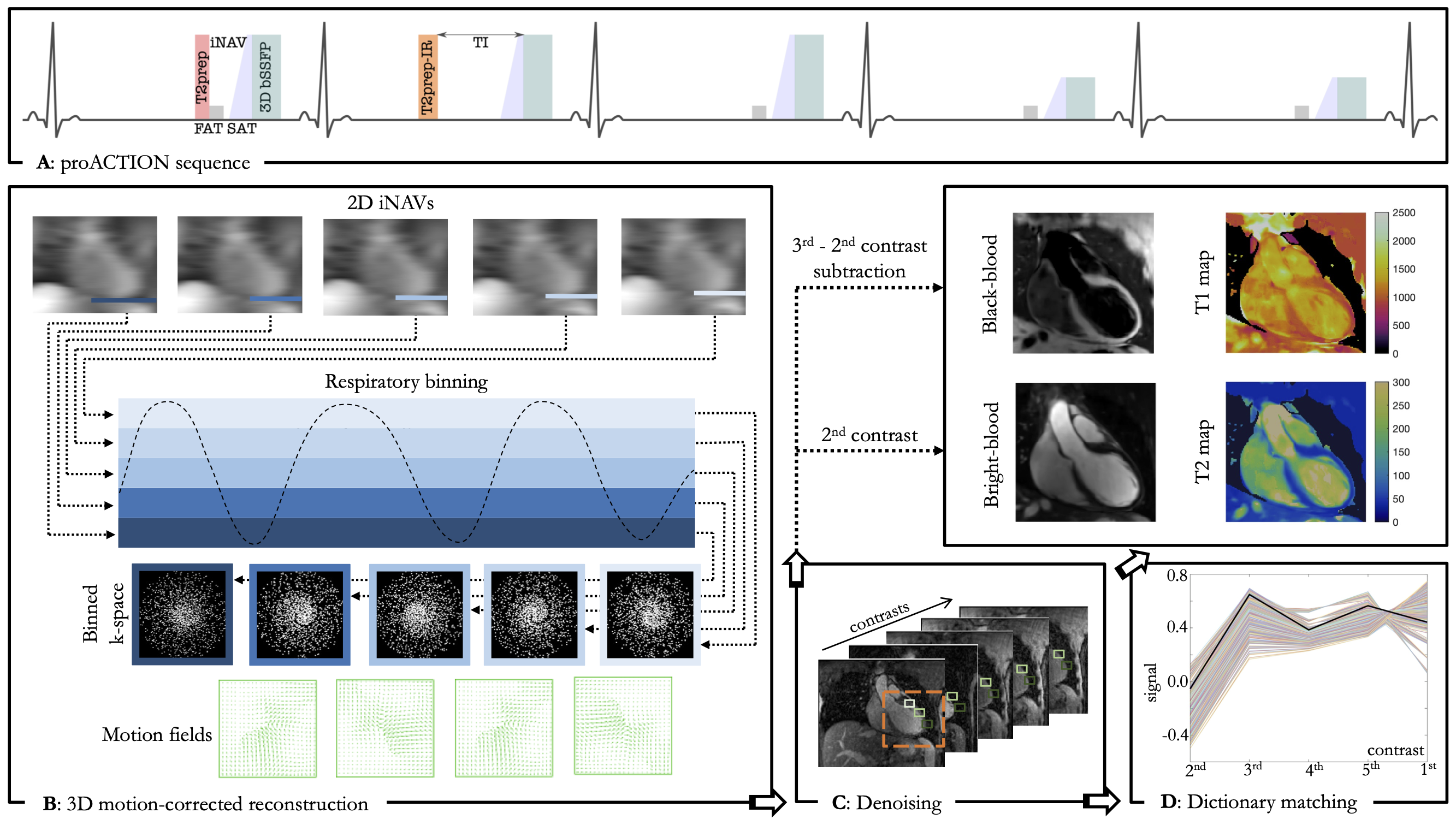
The proposed ECG-triggered proACTION research sequence consists of a repeating set of five heartbeats (HB) arranged in an interleaved manner, incorporating distinct T2 preparation (T2prep) modules, an inversion recovery pulse and acquisition with varying flip angles (FA) (Fig.1). 2D low-resolution image-based navigators (iNAV5) are acquired prior to each HB by spatially encoding the ramp-up pulses to perform beat-to-beat intra-bin translational motion estimation and correction, as well as respiratory binning of 3D data. A variable-density 3D cartesian trajectory with spiral profile order6 and golden angle step is employed to collect a 5-fold undersampled data with 100% respiratory efficiency resulting in a predictable scan time of 10 min for a normal heart-rate (HR) of 60bpm. Images are reconstructed using 3D non-rigid motion corrected7 itSENSE followed by patch‐based low-rank regularization (HD-PROST8). A short TI of 110ms was chosen to enable epicardial fat suppression in the 2ndHB. In the remaining HBs, frequency selective inversion recovery (SPIR) fatsat pulses are employed (flip angle = 110°-130°). The contrast in the 2ndHB serves as a bright-blood image. The black-blood volume is obtained by a direct magnitude subtraction of the 2nd from the 3rdHB with a positiv contrast window. Joint T1/T2 maps are generated voxel-wise by maximizing the inner product of the measured signal with a previously generated dictionary using the extended phase graph (EPG) method. To allow for appropriate signal-to-noise, FA was set to 70° for the HBs involved in the anatomical imaging, while lower FA of 30° was used to increase T1-sensitivity for remaining HBs. As the bSSFP signal at 1.5T is sensitive to inaccuracies in FA, the nominal FA may vary because of B1 inhomogeneities. To account for this, B1 variation up to 5% is included as an additional dictionary entry for EPG. Data was acquired on a 1.5T scanner (MAGNETOM Avanto Fit, Siemens Healthineers, AG, Erlangen, Germany) with a bSSFP readout (TR/TE=3.4/1.7ms, FOV=320x320x90-115m, isotropic spatial resolution=1.4mm) in coronal orientation, utilizing subject dependent trigger delay and acquisition window of 100ms. Imaging was performed during the mid-diastolic rest period to minimize cardiac motion. proACTION sequence was evaluated in the standardized T1MES9 phantom and three healthy subjects (28±3 years, heart-rates of 47-62 bpm) against conventional 2D MOLLI and T2prep bSSFP mapping sequences. Bull’s-eye-plots were generated from 3D proACTION T1/T2maps with 16 segments AHA model across the short-axis.Results
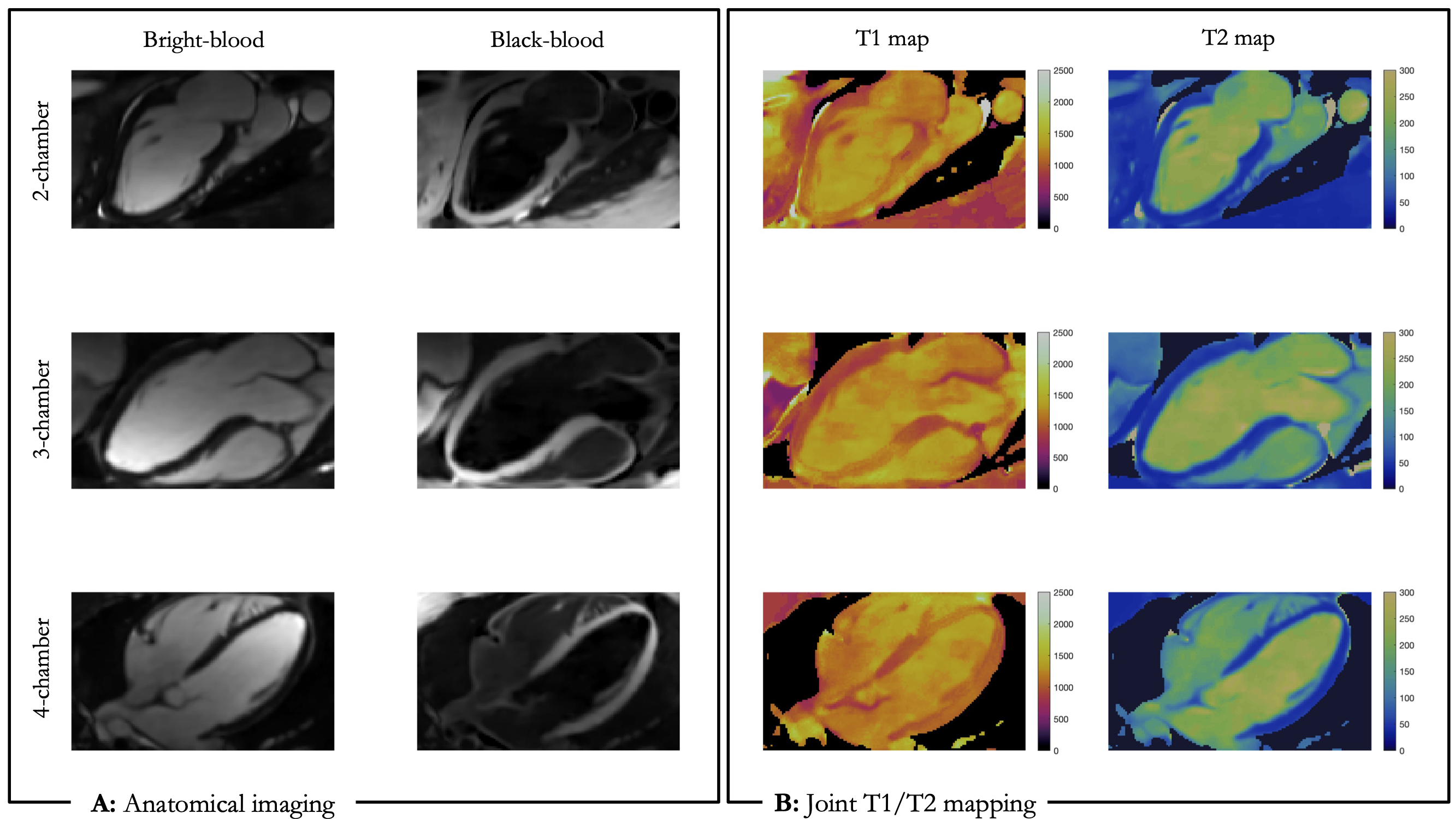
Phantom: Phantoms results (Fig.2) showed good agreement for T1 and T2 values in comparison to 2D conventional MOLLI and T2prep bSSFP mapping sequences. In the phantom study (Fig3,C), the optimal T2prep duration of 70ms in the 2ndHB also showed expected visual agreement with Bloch simulations (Fig2,D).Healthy subjects: The whole-heart cardiovascular anatomy in coronal orientation via bright- and black-blood imaging is illustrated in Fig3,A. Left and right coronary arteries can be seen on the high-resolution bright-blood images (Fig3,B). proACTION representative 3D anatomical images, providing good delineation of cardiac and vascular structures from different views (Fig4.A), are displayed together with corresponding T1 and T2 maps (Fig4.B). Comparable map quality (Fig.5A,B) and similar mid-cavity septal parametric values (Fig.C,D) were observed on healthy subjects with respect to conventional mapping techniques. proACTON provides slightly higher values than 2D MOLLI, which is known to underestimate10 T1 values.
Discussion and further work
The proposed 3D proACTION sequence enables simultaneous acquisition of bright- and black-blood images alongside with joint T1/T2 mapping in a single fast scan, providing good agreement against conventional sequences and promising results in healthy subjects. Compared to the previous version of the sequence with four contrasts4, proACTION uses five interleaves with variable FA, which resulted in better in better precession for T1 parametrical mapping. The acceleration factor has been increased from 4 to 5 as well to maintain the same scan time duration without any visible decrease in image or map quality. Future work will include validation on a larger cohort of healthy subjects and in patients with suspected cardiovascular disease.Acknowledgements
The authors acknowledge financial support from: (1) BHF RG/20/1/34802 (2) EPSRC EP/V044087/1 (3) Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1), (4) ANID Millennium Institute iHEALTH, ICN2021_004; Fondecyt 1210637 and 1210638; Basal Funding, IMPACT, FB210024 and (6) the Technical University of Munich – Institute for Advanced StudyReferences
[1] Grizzard, J. D., Judd, R. M., & Kim, R. J. (2008). Cardiovascular MRI in practice a teaching file approach. Springer.
[2] Messroghli, D.R., Moon, J.C., Ferreira, V.M. et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 19, 75 (2017). https://doi.org/10.1186/s12968-017-0389-8
[3] Milotta G, Ginami G, Cruz G, Neji R, Prieto C, Botnar RM. Simultaneous 3D whole-heart bright-blood and black blood imaging for cardiovascular anatomy and wall assessment with interleaved T2 prep-IR. Magn Reson Med. 2019 Jul;82(1):312-325. doi: 10.1002/mrm.27734. Epub 2019 Mar 21. PMID: 30896049.
[4] Ivan Kokhanovskyi, Michael G Crabb, Karl P Kunze, Radhouene Neji, Carl Ganter, Donovan P Tripp, Carlos Castillo-Passi, Dimitrios C Karampinos, Claudia Prieto, and Rene M Botnar. (2023). Multiparametric 3D cardiac MR for simultaneous bright- and black-blood imaging and joint T1/T2 myocardial tissue mapping. Proc. Intl. Soc. Mag. Reson. Med. 31, 1687.
[5] Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012 Feb;67(2):437-45. doi: 10.1002/mrm.23027. Epub 2011 Jun 7. PMID: 21656563.
[6] Prieto C, Doneva M, Usman M, Henningsson M, Greil G, Schaeffter T, Botnar RM. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015 Mar;41(3):738-46. doi: 10.1002/jmri.24602. Epub 2014 Feb 27. PMID: 24573992.
[7] Cruz G, Atkinson D, Henningsson M, Botnar RM, Prieto C. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2017 May;77(5):1894-1908. doi: 10.1002/mrm.26274. Epub 2016 May 25. PMID: 27221073; PMCID: PMC5412916.
[8] Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med. 2019 Jun;81(6):3705-3719. doi: 10.1002/mrm.27694. Epub 2019 Mar 4. PMID: 30834594; PMCID: PMC6646908.
[9] Gabriella Captur et al. “A medical device-grade T1 and ECV phantom for global T1 mapping quality assurance—the T1 Mapping and ECV Standardization in cardiovascular magnetic resonance (T1MES) program”. In: Journal of Cardiovascular Magnetic Resonance 18 (Sept. 2016). doi: 10.1186/s12968-016-0280-z.
[10] Cooper MA, Nguyen TD, Spincemaille P, Prince MR, Weinsaft JW, Wang Y. How accurate is MOLLI T1 mapping in vivo? Validation by spin echo methods. PLoS One. 2014 Sep 11;9(9):e107327. doi: 10.1371/journal.pone.0107327. PMID: 25211243; PMCID: PMC4161413.
[11] Castillo-Passi, C, Coronado, R, Varela-Mattatall, G, Alberola-López, C, Botnar, R, Irarrazaval, P. KomaMRI.jl: An open-source framework for general MRI simulations with GPU acceleration. Magn Reson Med. 2023; 1- 14. doi: 10.1002/mrm.29635
Figures
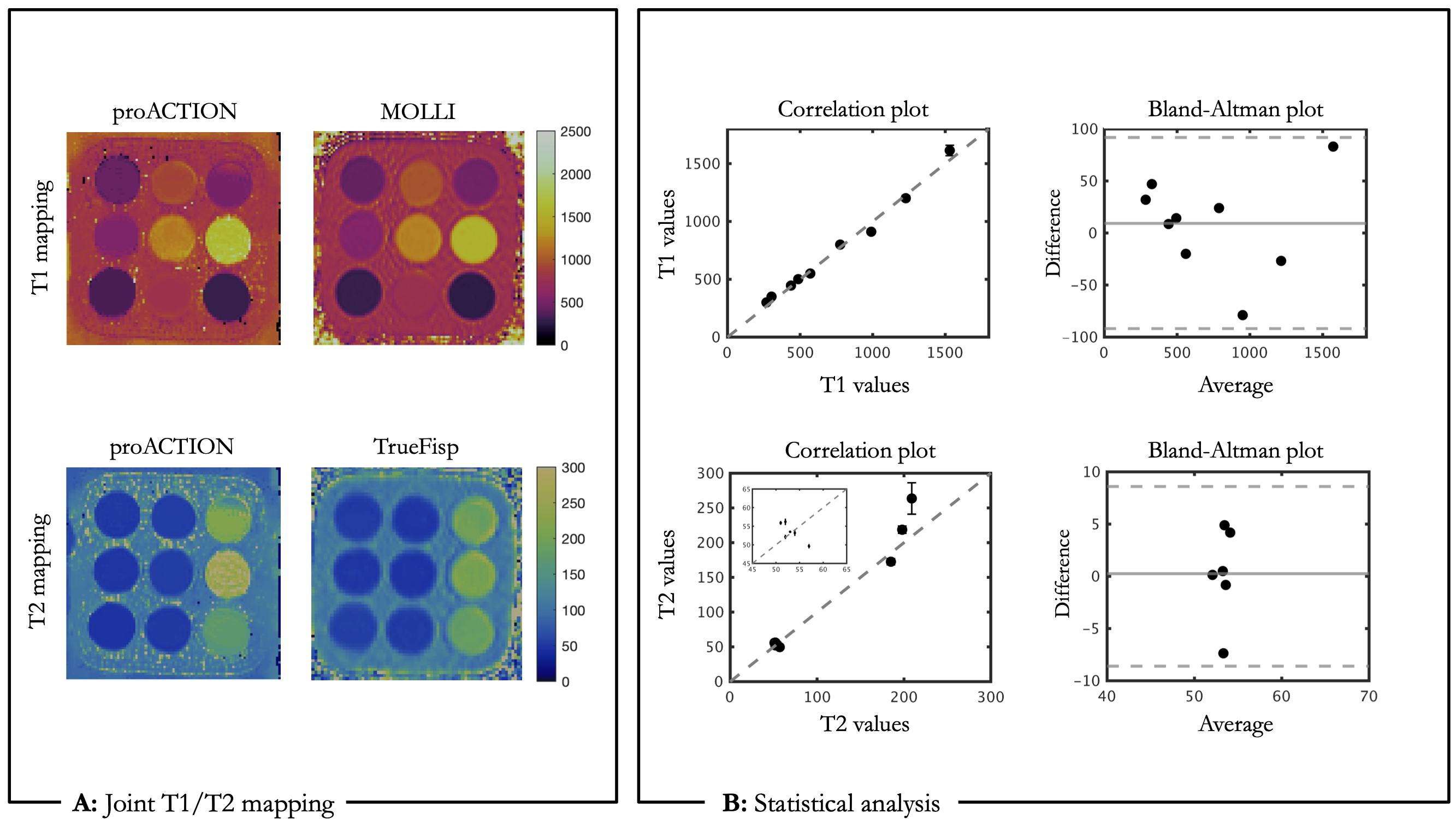
Validation of proposed 3D proACTION sequence in the standardized T1MES9 phantom against reference 2D T1 and T2 mapping sequences (MOLLI/TrueFisp) with simulated HR=60 bpm.