0681
Highly-efficient free-breathing 3D whole-heart joint T1/T2 mapping and water/fat imaging at 0.55T1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 3School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 4Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Myocardium, Low-Field MRI, Parametric mapping
Motivation: Myocardial T1 and T2 mapping has emerged as a useful clinical tool for the diagnosis of different heart disease. However, current mapping sequences were mostly developed with 2D breathhold acquisitions and validated at 1.5T or 3T. The investigation of myocardial mapping techniques on more affordable low-field MRI systems is scarce.
Goal(s): To develop a highly-efficient free-breathing 3D whole-heart joint T1/T2 mapping sequence with isotropic-resolution at 0.55T.
Approach: The proposed sequence acquires 3 interleaved volumes for joint T1/T2 estimation and water/fat separation.
Results: The proposed sequence shows good agreement with spin-echo reference in phantom and provides comparable results in-vivo with conventional 2D mapping sequences.
Impact: The proposed sequence enables comprehensive 3D joint T1/T2 mapping and water/fat anatomical evaluation of the whole-heart with 2mm isotropic-resolution at 0.55T during a fast free-breathing scan and thus shows promise for the detection of different cardiac diseases.
INTRODUCTION
Myocardial T1 and T2 mapping has emerged as a useful clinical tool for the detection of both focal and diffused heart disease1. T1 and T2 values depend on the magnetic field strength2. The most common clinical field strengths are 1.5T and 3T. Recently, more affordable MRI systems with a lower field strength of 0.55T have become commercially available3. However, there is limited experience with parametric mapping at this new field strength. The shorter T1 and longer T2 relaxation time require specific optimization in sequence design. In addition, the limited gradient performance of current 0.55T scanners leads to longer repetition and echo times, increasing scan time3. Currently available T1 and T2 mapping sequences are time inefficient as they are performed in 2 breathholds sequentially and acquire several single-shot 2D images to produce single slice T1 and T2 maps. Thus, an efficient 3D T1/T2 mapping sequence at 0.55T is in high demand. Here, we propose and validate a motion-compensated free-breathing isotropic-resolution 3D whole-heart joint T1/T2 mapping sequence with Dixon water/fat separation at 0.55T.METHODS
Sequence designThe proposed sequence has a similar framework as a previous joint T1/T2 mapping sequence we developed at 1.5T4. However, the number of volumes is reduced from four to three considering the shorter T1 on 0.55T and to shorten the scan time. The three ECG triggered volumes are acquired in an interleaved scheme with inversion recovery preparation (TI=150ms), no preparation and T2-preparation (TE=50ms) respectively (Figure 1). 2D image navigators (iNAVs) with 14 echoes and 3° flip angle are performed before the acquisition of each volume for motion compensation, enabling 100% respiratory scan efficiency5. 2-point bipolar Dixon gradient echo is used to acquire pseudo in-phase and opposed-phase echoes for water/fat separation. A variable-density Cartesian trajectory with spiral-like profile order (VD-CASPR) is adopted with 4-fold under-sampling6. The acquired data are reconstructed with non-rigid motion corrected iterative-SENSE with water/fat separation and patch-based low-rank regularization (PROST)7. Co-registered 3D T1 and T2 maps are jointly calculated voxel-by-voxel from the three water volumes with a dictionary matching method8. The dictionary was generated with a subject-specific Bloch equation simulation to calculate the signal intensity of each volume. The third volume with T2-preparation generates the bright-blood water image and the fat image.
Simulation
Landscape graphs were simulated to analyse the T1 and T2 encoding of the proposed sequence in comparison with the previous 4-volume sequence4,9. The performance was evaluated for T1/T2 values of healthy myocardium (700/58ms), diseased myocardium (760/70ms), and blood (1100/250ms) at 0.55T2,3.
Phantom and in-vivo experiments
Experiments were performed on a T1MES phantom10 and 3 healthy subjects (1 males, 27±2 years) using a 0.55T MR scanner (MAGNETOM Free.Max, Siemens Healthcare, Erlangen, Germany). Imaging parameters for the 3D sequences were: 2mm isotropic-resolution, TR/TEs=9.81/2.65/6.5ms, FA=8°, bandwidth=401Hz/pixel, 16 segments per heartbeat. Reference phantom T1 and T2 values were measured with single-echo spin-echo sequences. Conventional 2D T1/T2 maps were acquired with MOLLI 5(3)3 and T2-prepared bSSFP (TE=0/25/55ms) respectively with 2.3×2.3mm2 in plane resolution and 10mm slice thickness.
RESULTS
Landscape graphs showed that the proposed 3-volume sequence had a higher least square error (LSE) variation for the T1/T2 values of different tissue and a narrower minimum compared with the previous 4-volume sequence (Figure 2), which indicated a better T1 and T2 encoding.For phantom imaging (Figure 3), both joint T1/T2 sequences with 3 or 4 volumes and MOLLI showed excellent agreement with reference T1 values (R2=0.99), while the joint T1/T2 sequence with 3 or 4 volumes (R2=0.99) demonstrated better agreement with reference T2 values than the bSSFP sequence (R2=0.93). Joint T1/T2 sequences with 3 and 4 volumes had a comparable T1 and T2 coefficient of variation, which were higher than that of MOLLI and comparable with the bSSFP sequence.
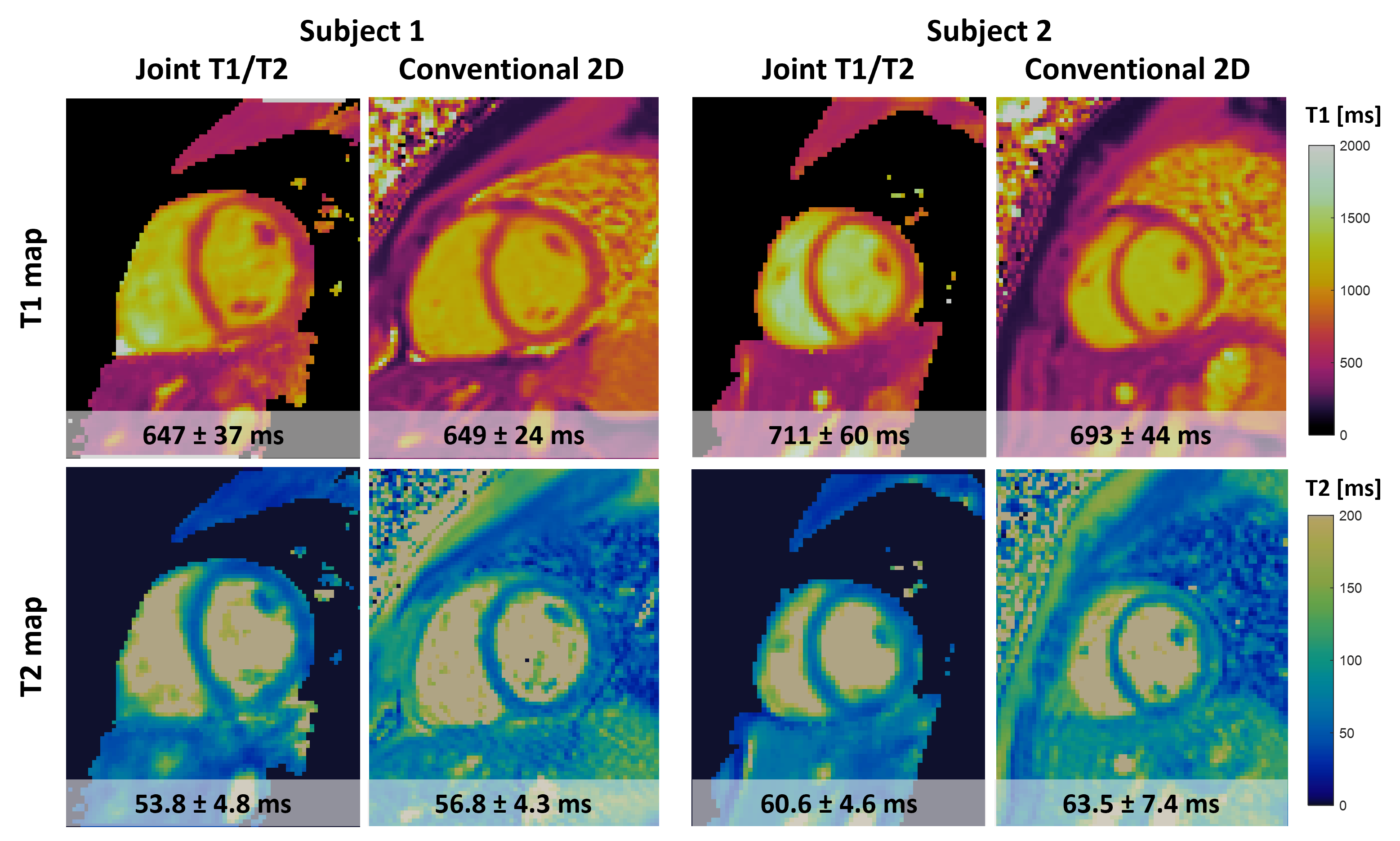
Representative images acquired in a healthy subject are shown in Figure 4. The proposed sequence provides co-registered water/fat images and T1/T2 maps of the whole-heart within a scan time of ~7.1 mins. Isotropic-resolution enabled reformatting in different orientations. T1 and T2 maps acquired with the proposed sequence had comparable image quality and myocardial T1/T2 values compared to the conventional 2D sequences (Figure 5).
DISCUSSION and CONCLUSION
A 3D joint T1/T2 mapping sequence that acquires 3 volumes was developed at 0.55T. The scan efficiency was improved compared with a previous 4-volume sequence, while the performance of T1/T2 measurements was not sacrificed as simulation and phantom experiments demonstrated. In-vivo experiments showed that the proposed sequence allows for whole-heart imaging at 0.55T with comparable performance compared to conventional 2D sequences. Further validations are required on a larger cohort of healthy subjects and patients with cardiovascular disease.Acknowledgements
The authors acknowledge financial support from: (1) BHF RG/20/1/34802 (2) EPSRC EP/V044087/1 (3) ANID Millennium Institute iHEALTH, ICN2021_004; Fondecyt 1210637 and 1210638 and (4) the Technical University of Munich – Institute for Advanced Study.References
1. Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). Journal of Cardiovascular Magnetic Resonance. 2017;19(1):75. doi:10.1186/s12968-017-0389-82. Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
3. Varghese J, Jin N, Giese D, et al. Building a comprehensive cardiovascular magnetic resonance exam on a commercial 0.55 T system: A pictorial essay on potential applications. Front Cardiovasc Med. 2023;10. doi:10.3389/fcvm.2023.1120982
4. Milotta G, Bustin A, Jaubert O, Neji R, Prieto C, Botnar RM. 3D whole-heart isotropic-resolution motion-compensated joint T1/T2 mapping and water/fat imaging. Magn Reson Med. 2020;84(6):3009-3026. doi:https://doi.org/10.1002/mrm.28330
5. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012;67(2):437-445. doi:10.1002/mrm.23027
6. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary mra using golden-step Cartesian acquisition. Journal of Magnetic Resonance Imaging. 2015;41(3):738-746. doi:10.1002/jmri.24602
7. Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med. 2019;81(1):102-115. doi:10.1002/mrm.27354
8. Si D, Guo R, Liu B, Herzka DA, Ding H. 3D free-breathing simultaneous whole heart T 1 and T 2 mapping based on SAturation Recovery and Variable flip Angle ( SAVA ). In Proceedings of the 30th Annual Meeting of ISMRM. 2022.
9. Gómez PA, Molina-Romero M, Buonincontri G, Menzel MI, Menze BH. Designing contrasts for rapid, simultaneous parameter quantification and flow visualization with quantitative transient-state imaging. Sci Rep. 2019;9(1):8468. doi:10.1038/s41598-019-44832-w
10. Captur G, Gatehouse P, Keenan KE, et al. A medical device-grade T1 and ECV phantom for global T1 mapping quality assurance — the T 1 Mapping and ECV Standardization in cardiovascular magnetic resonance ( T1MES ) program. Journal of Cardiovascular Magnetic Resonance. 2016:1-20. doi:10.1186/s12968-016-0280-z
Figures
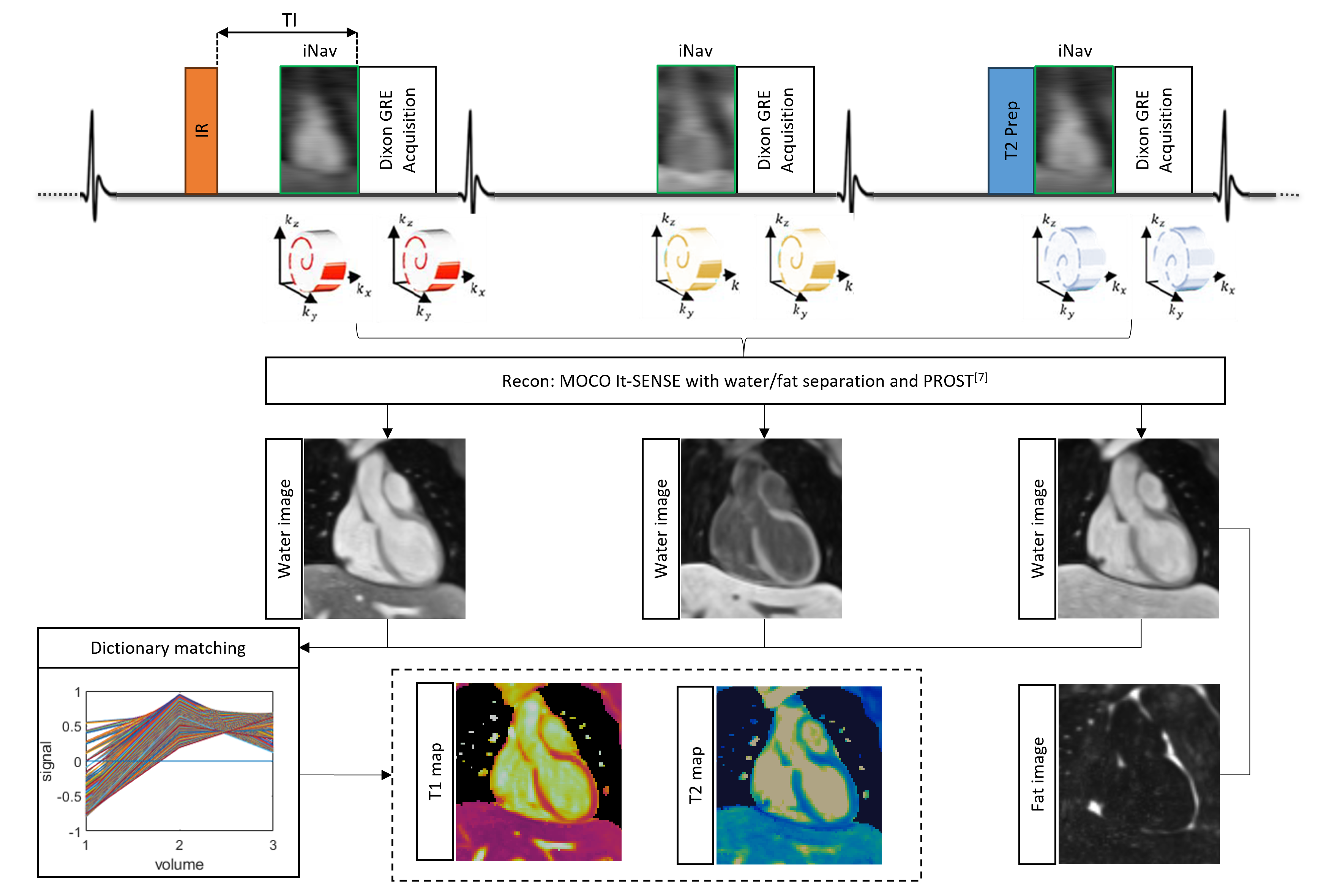
Figure 1. Framework of the proposed joint T1/T2 mapping sequence. 3 ECG triggered volumes are acquired with IR (TI=150ms), no preparation and T2-prep (TE=50ms) respectively. 2D iNAVs are performed for respiratory motion compensation with 100% scan efficiency. Dixon GRE using 4-fold under-sampled VD-CASPR is adopted. The acquired data are reconstructed with non-rigid motion corrected iterative-SENSE with water/fat separation and PROST denoising7. Coregistered 3D T1/T2 maps are jointly calculated voxel-by-voxel from the three water volumes with a dictionary matching method.
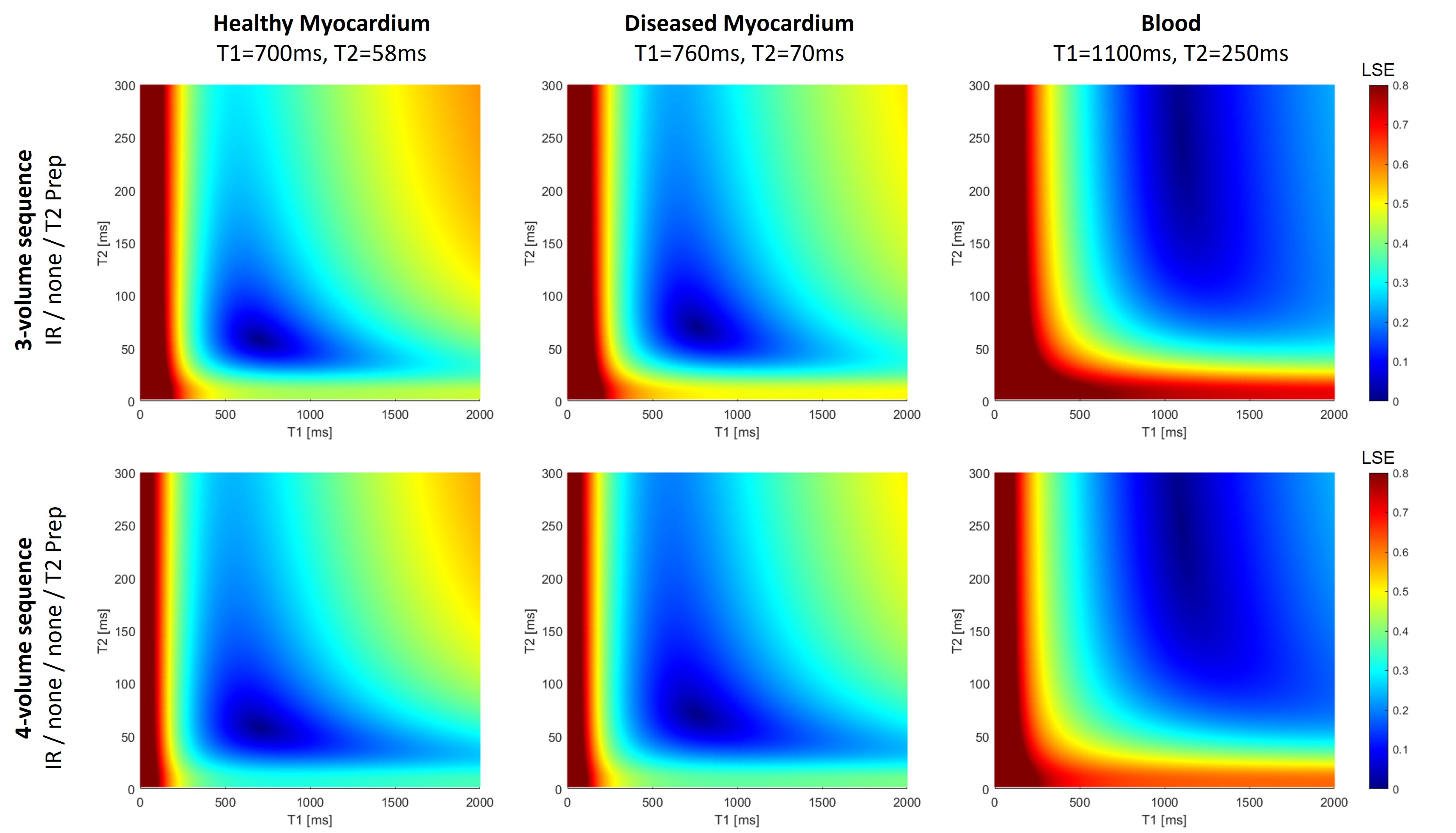
Figure 2. Landscape graphs simulation of 3 and 4-volume sequences for healthy myocardium, diseased myocardium and blood for a field strength of 0.55T. Least square error (LSE) is calculated between the fixed T1/T2 pair and all the other T1/T2 entries. T1 and T2 encoding capability is represented by the narrowness of the minimum identified by the LSE (steepness of the gradient in T1 and T2 direction). Higher T1 and T2 encodings (higher LSE variation and narrower minimum around the T1/T2 values) are obtained with the 3-volume sequence for all three simulated tissues.
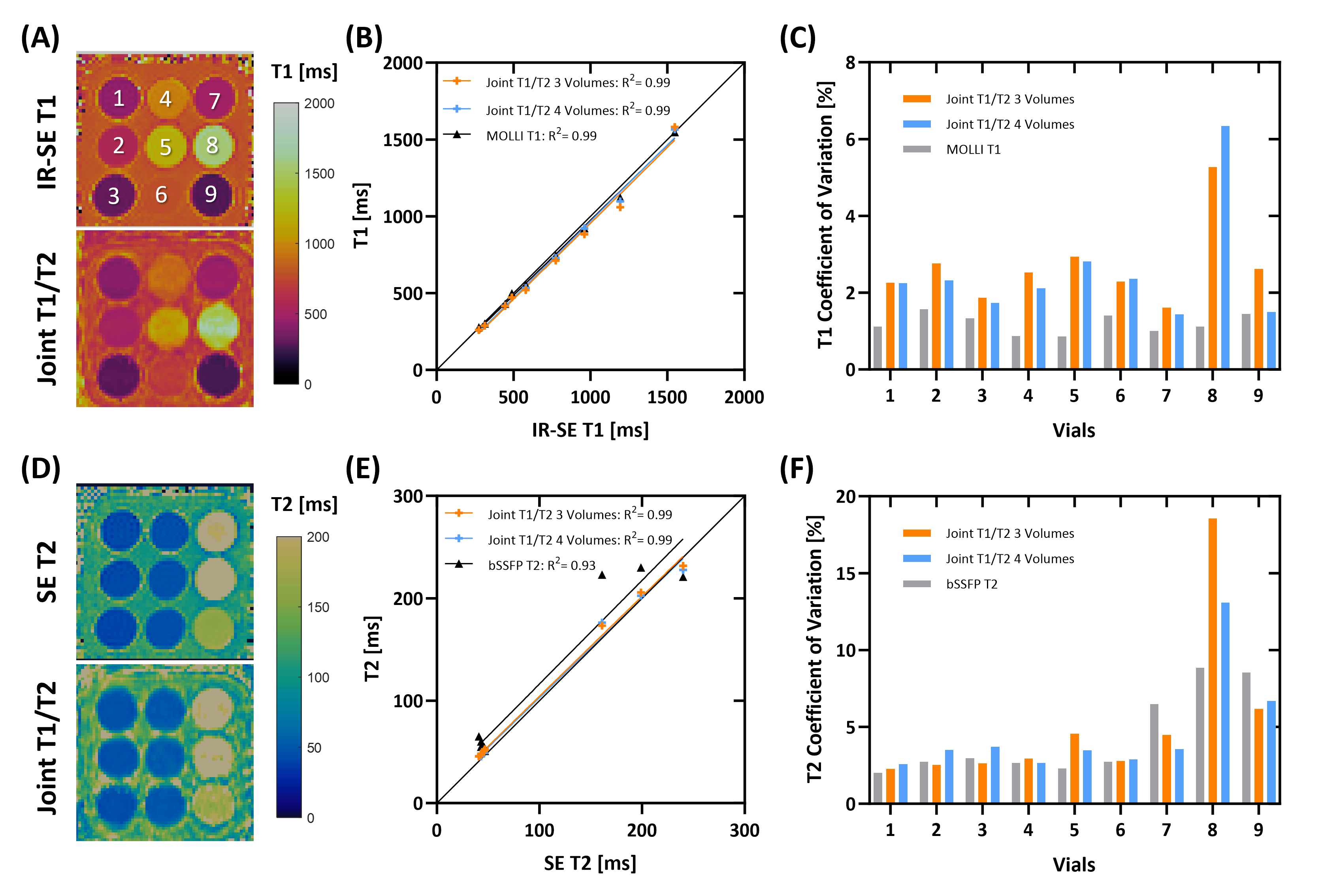
Figure 3. Phantom results comparing the different sequences at a simulated heart rate of 60bpm. (A, D) Representative T1 and T2 maps acquired with reference and the proposed joint T1/T2 mapping sequence. (B, E) Linear regression plot of T1/T2 measured by conventional 2D and 3D joint T1/T2 sequences in comparison with reference values. (C, F) T1/T2 coefficient of variation (CV) acquired with conventional and proposed mapping sequences. For the 8th phantom vial with longer T1, a higher T1 and T2 CVs is observed for the joint T1/T2 mapping sequences due to lower SNR.
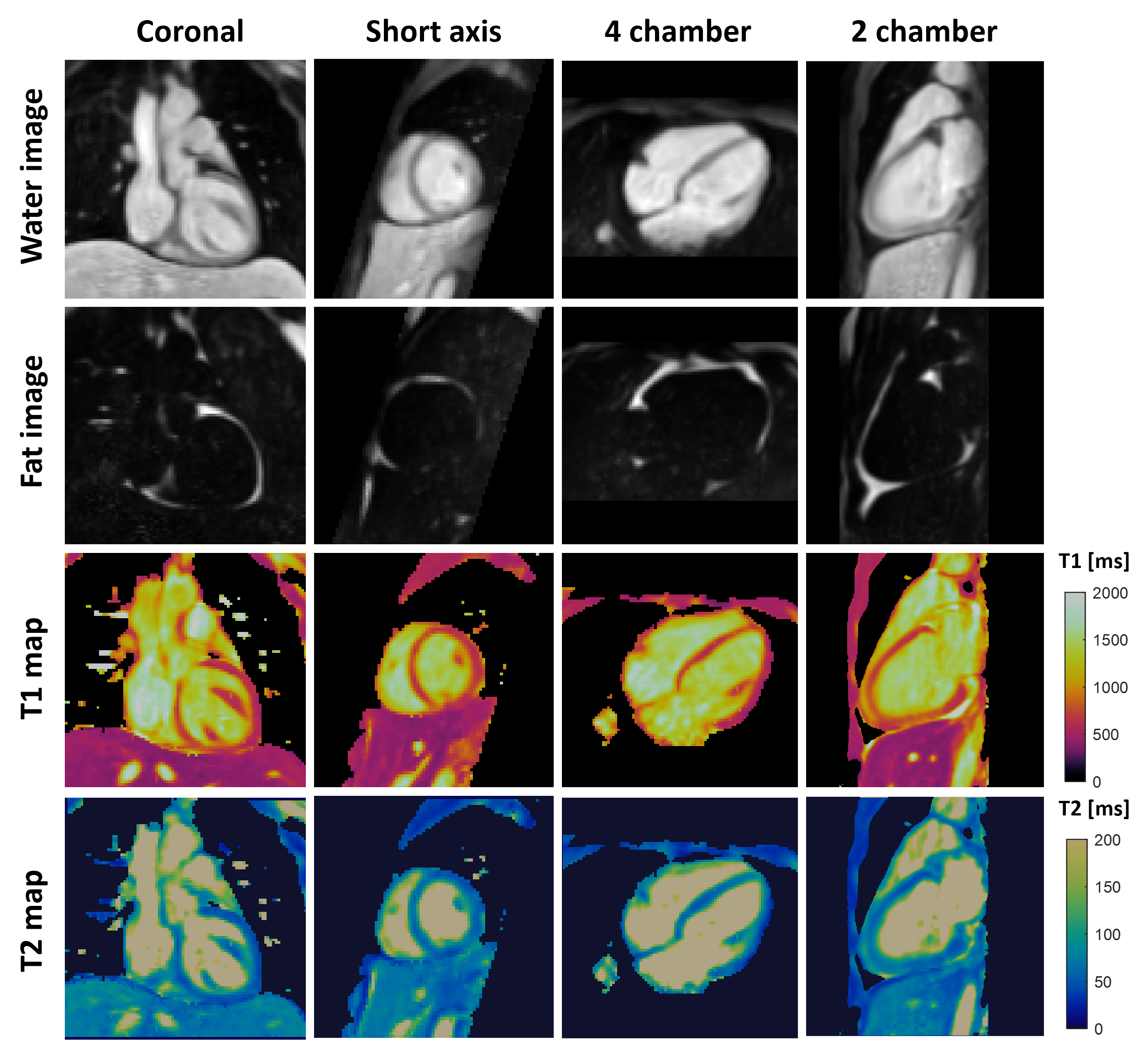
Figure 4. Representative co-registered 3D bright-blood water and fat image (from the third volume with T2-prep), and T1/T2 maps obtained with the proposed sequence from a healthy subject. Good depiction of cardiac structure and separation of water/fat are achieved across the whole 3D volume. Uniform whole-heart T1 and T2 quantification can be observed in different orientations.