0680
Physically and Anatomically Constrained Self-Supervised Motion Correction for Free-Breathing Cardiac T1 Mapping1The Technion – Israel Institute of Technology, Haifa, Israel, 2Bnai Zion medical center, Haifa, Israel, Haifa, Israel
Synopsis
Keywords: Myocardium, Machine Learning/Artificial Intelligence, Motion Correction
Motivation: Cardiac T1 mapping is often limited by the need for breath-holding to prevent motion artifacts, which restricts its use in patients who cannot hold their breath.
Goal(s): To create a self-supervised deep learning method for motion-corrected, free-breathing cardiac T1 mapping without requiring large datasets or worrying about data variability.
Approach: We present a new self-supervised model that combines a signal relaxation model with anatomical constraints and employs the voxel-morph framework for motion correction. Our model's performance was assessed using a publicly available myocardial T1 mapping dataset.
Results: Our approach outperformed other state-of-the-art registration methods in terms of R2, DICE, and Hausdorff distance.
Impact: Our model offers the possibility of extending cardiac T1 mapping to patients who cannot perform breath-hold MRI procedures by ensuring robust motion correction for accurate T1 mapping, all without the necessity for large training datasets or worries about data anomalies.
Introduction
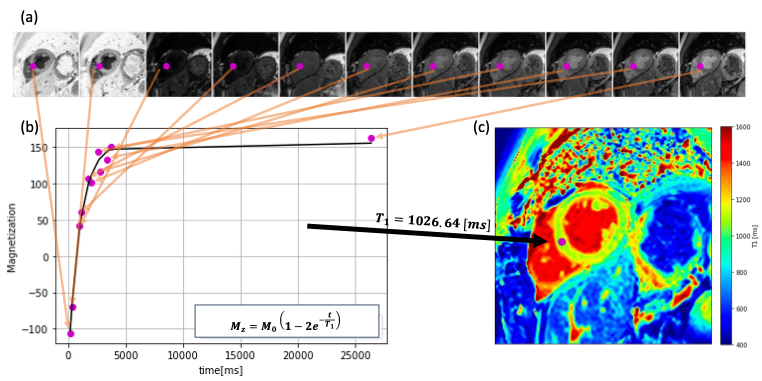
Quantitative T1 mapping via MRI (Fig.1) is crucial for diagnosing diffuse heart diseases by measuring myocardial tissue's relaxation time1 . Yet, its accuracy is often compromised by heart and respiratory motion, as well as patient movement, which can distort T1 maps and risk misdiagnosis2. While echo-triggering addresses heart motion and breath-hold techniques like MOLLI sequences3 reduce respiratory effects, they're not suitable for patients who can't hold their breath or have irregular heartbeats, limiting the technique's use and potentially affecting the reliability of diagnoses.Recently, supervised deep-learning techniques have been introduced for aligning images to correct motion as a preliminary step in cardiac T1 mapping4,5,6. However, these techniques don't consider the signal decay inherent in the imaging process, which may result in unrealistic image distortions. Further, these methods require extensive training datasets and might be unstable to out-of-distribution data.Data
We employed an open-access dataset for myocardial T1 mapping12, comprising 210 individuals (134 males, 76 females), all with confirmed or potential cardiovascular issues. This data was collected on a 1.5T Philips Achieva MRI scanner with a 32-channel cardiac coil, using the ECG-triggered STONE sequence for free-breathing, slice-interleaved T1 mapping7. It provided 5 slices across 11 time points per patient, with expertly segmented myocardium.Algorithms
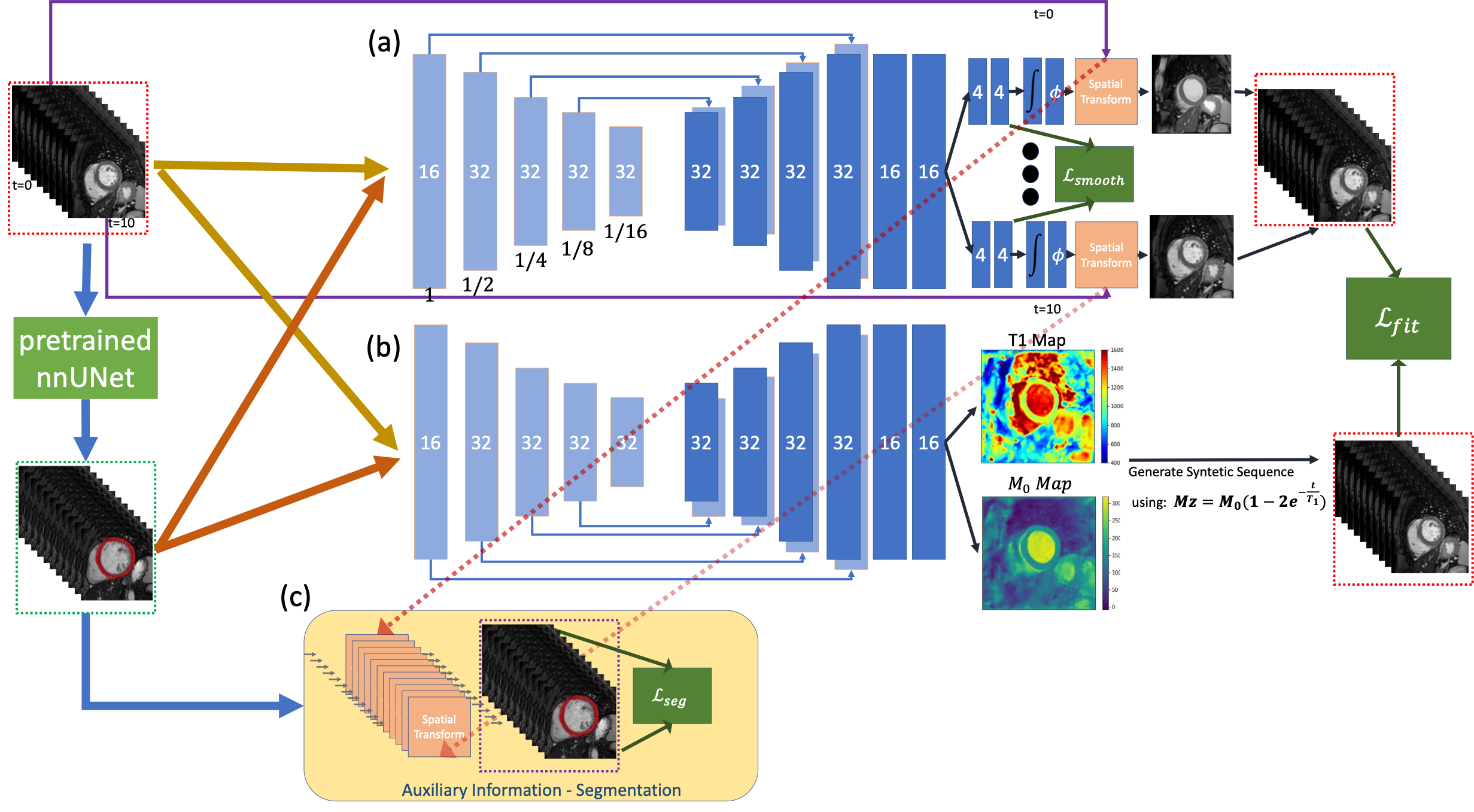
We present a self-supervised deep learning framework that simultaneously corrects for motion and computes T1 maps from free-breathing MRI acquisitions. This model (Fig.2) melds a refined version of the Voxelmorph model for image registration8, which now features multiple registration heads, with a module for fitting an exponential T1 signal decay model that utilizes an encoder-decoder structure to yield T1 and M0—the parameters representing exponential signal relaxation. Additionally, a pre-trained nnUNet designed for myocardial segmentation is integrated. This synergy between the signal decay fitting and myocardial segmentation ensures the model promotes deformations that are both physically and anatomically credible along the T1 relaxation trajectory.We encourage the generation of deformations that are both physically and anatomically feasible by implementing a composite loss function. This function advances physical fidelity by applying Mean-squared Error loss to compare the deformed images with the anticipated T1 relaxation mode, and anatomical accuracy using Dice loss between the deformed segmentation. We also ensure the smoothness of the deformation fields through the L2 norm on their gradients.
Experimental methodology
We implemented a 5-fold cross-validation scheme with 210 participants to refine an nnUNet network dedicated to myocardial segmentation. Leveraging this network in a self-supervised fashion, we input the T1-weighted (T1W) images and their associated nnUNet-derived segmentations into our newly constructed network, which was uniquely tailored and fine-tuned for each participant's data. Our method was benchmarked against two cutting-edge deep learning medical image registration models: the pair-based probabilistic diffeomorphic VoxelMorph with a mutual-information loss function8, and SynthMorph9 , along with REG-MI10,13 and PCMC-T111, which are specially crafted for motion correction during T1 mapping. It is essential to highlight that SynthMorph is the sole exception among these models as being self-supervised; the others demand extensive training for each protocol.Additionally, we contrasted our results with T1 maps calculated directly from raw images without applying motion correction. The evaluation of our approach incorporated the determination of the R2 value reflecting the model's fit to actual myocardial data, the Dice coefficient, and the Hausdorff distance measures for myocardium segmentation accuracy.
Results
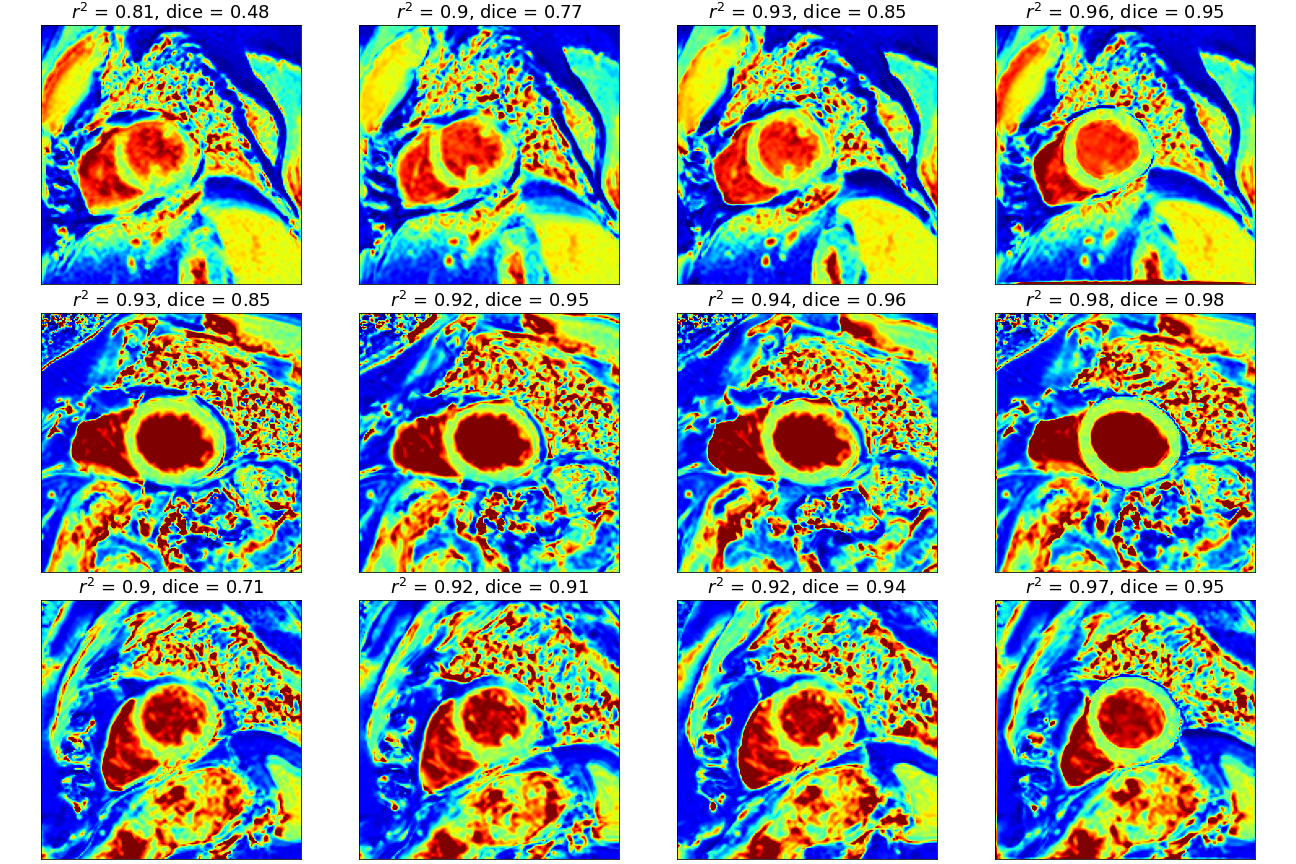
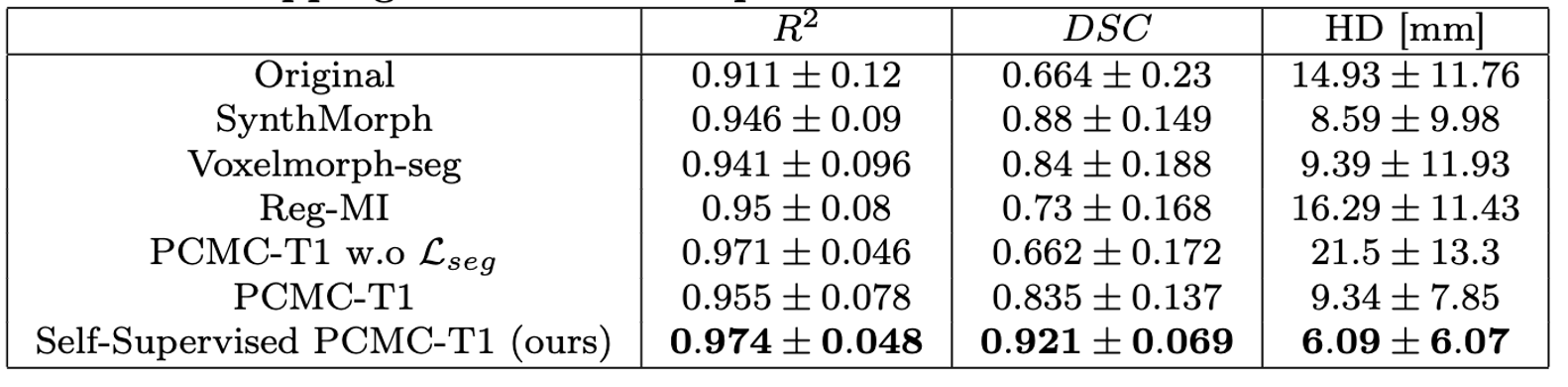
Table 1 provides a summary of our findings. Our Self-Supervised PCMC-T1 method demonstrated the highest performance in terms of R2, DICE, and Hausdorff distance. These results suggest that our approach enhances the physical plausibility of deformations through signal relaxation and anatomical consistency. Our results are particularly noteworthy considering that we made comparisons with methods requiring a full training process and the use of manually annotated segmentations.Conclusion
We introduce a pioneering Self-Supervised method that fuses physical and anatomical insights for correcting motion in T1 mapping. Our breakthrough is the application of Self-Supervised learning and a pre-existing nnUNet framework, enriched with a signal decay model within the network's architecture. This allows for generating corrected T1 maps across various imaging protocols, eliminating the necessity for protocol-specific data collection and extensive training. Our findings show a significant improvement in fit quality, Dice score, and Hausdorff distance. The proposed model promises to widen the scope of quantitative cardiac T1 mapping to include patients who cannot perform breath-hold during MRI scans, ensuring precise T1 estimation despite motion.Acknowledgements
This work was supported in part by research grants from the Israel-US Binational Science Foundation, the Israeli Ministry of Science and Technology, the Israel Innovation Authority, and the joint Microsoft Education and the Israel Inter-university Computation Center (IUCC) program.References
[1] Andrew J Taylor et al. “T1 mapping: basic techniques and clinical applications”. In: JACC: Cardiovascular Imaging 9.1 (2016),pp. 67–81.
[2] Sofie Tilborghs et al. “Robust motion correction for cardiac T1 and ECVmapping using a T1 relaxation model approach”. In: Medical Image Analysis 52 (2019), pp. 212–227.
[3] Sébastien Roujol et al. “Accuracy, precision, and reproducibility of fourT1 mapping sequences: a head-to-head comparison of MOLLI, ShMOLLI,SASHA, and SAPPHIRE”. In: Radiology 272.3 (2014), pp. 683–689.
[4] Ricardo A Gonzales et al. “MOCOnet: robust motion correction of cardiovascular magnetic resonance T1 mapping using convolutional neuralnetworks”. In: Frontiers in Cardiovascular Medicine (2021), p. 1689.
[5] Yuze Li et al. “Motion correction for native myocardial T1 mapping using self-supervised deep learning registration with contrast separation”. In:NMR in Biomedicine 35.10 (2022), e4775.
[6] Changchun Yang et al. “DisQ: Disentangling Quantitative MRI Mapping of the Heart”. In: Medical Image Computing and Computer AssistedIntervention–MICCAI 2022: 25th International Conference, Singapore,September 18–22, 2022, Proceedings, Part VI. Springer. 2022, pp. 291–300.4
[7] Sebastian Weingärtner et al. “Free-breathing multislice native myocardial T1 mapping using the slice-interleaved T1 (STONE) sequence”. In:Magnetic resonance in medicine 74.1 (2015), pp. 115–124.
[8] Guha Balakrishnan et al. “VoxelMorph: a learning framework for deformablemedical image registration”. In: IEEE transactions on medical imaging38.8 (2019), pp. 1788–1800.
[9] Malte Hoffmann et al. “SynthMorph: learning contrast-invariant registration without acquired images”. In: IEEE transactions on medical imaging41.3 (2021), pp. 543–558.
[10] Dar Arava et al. “Deep-Learning based Motion Correction for MyocardialT 1 Mapping”. In: 2021 IEEE International Conference on Microwaves,Antennas, Communications and Electronic Systems (COMCAS). IEEE.2021, pp.55–59.
[11] Eyal Hanania et al. “PCMC-T1: Free-Breathing Myocardial T1 Mappingwith Physically-Constrained Motion Correction”. In: International Conference on Medical Image Computing and Computer-Assisted Intervention.Springer. 2023, pp. 226–235.
[12] Hossam El-Rewaidy et al. “Nonrigid active shape model–based registrationframework for motion correction of cardiac T1 mapping”. In: Magneticresonance in medicine 80.2 (2018), pp. 780–791
[13] Eyal Hanania et al. “Deep-learning-based Group-wise Motion Correctionfor Myocardial T1 Mapping”. In: Proceedings of the ISMRM & SMRT Annual Meeting & Exhibition, Toronto, Canada. 2023.Figures