0679
Imaging pressure gradients and stress fields driving ISF flow in the brain by assimilating DENSE pulsatile motion data into a poroelastic model.1Dartmouth College, Hanover, NH, United States, 2University Medical Center Utrecht, Utrecht, Netherlands, 3Dartmouth-Hitchcock Medical Center, Lebanon, NH, United States
Synopsis
Keywords: Neurofluids, Neurofluids
Motivation: Interstitial fluid (ISF) flow in the brain is important for brain function and therapies. Very slow ISF flow is difficult to directly measure, however, the driving forces can be estimated from pulsatile motion fields.
Goal(s): We assimilate pulsatile motions from DENSE sequences into a poroelastic computational model which allows fluid pressure gradient and solid stress fields to be extracted.
Approach: Generalized least squares and Galerkin weighted residual methods were used to fit a pulsatile blood pressure field to the data and compute stresses/pressure gradients.
Results: Stress and pressure images show good symmetry and distributions are as expected from anatomical considerations.
Impact: Imaging the pulsatile fluid pressure gradients and solid stress fields provides new insights into the forces which drive flow of interstitial fluid in the brain, which is of critical importance in Alzheimer’s disease and currently very difficult to directly measure.
INTRODUCTION
Movement of fluids through brain tissue is vital for brain function and disease processes. The glymphatic hypothesis suggests that disruption of the of interstitial fluid movement is a causative pathway for Alzheimer’s disease.Brain tissue can be described as a fluid-saturated porous matrix where the hydromechanical behavior is governed by a poroelastic continuum model consisting of a porous elastic solid matrix with one or more compartments of infiltrating pore fluid. Three major compartments can be defined based on fluid mobility: Solid tissue and non-mobile intracellular fluid fits the description of the porous elastic matrix. The highly mobile blood is driven by the heart and provides the primary source of pressure-induced pulsation in the other components. Finally, interstitial fluid (ISF) which permeates the intercellular space is substantially less mobile than blood and is pushed around by pressure gradients and stress fields as the brain deforms and thought to provide the primary mechanism of waste clearance central to the development of dementia.
MRI has been used to measure movement of neurofluids; however, many of the techniques neglect the pulsatile elastic deformation of the brain tissue which is an important contributor to the movement of fluids. A simple analogy is a dirty sponge under running water – squeezing the sponge cycles the water much more quickly than constant flow. Measurements of the pulsatile motion of brain tissue have been made using DENSE MRI sequences which allows whole brain imaging of pulsatile motion.
In this work, we estimate a driving blood pressure field which reproduces the measured pulsatile motion fields in a poroelastic finite element model. This process assimilates the measured motions into a numerical model of the pulsatile hydrodynamics from which a range of other unmeasurable biologically relevant quantities can be calculated and is amenable to extensions into multi-fluid models which separately model blood and ISF.
Methods
MRI pulsatile motion imaging: A DENSE sequence[1,2] was used to image pulsatile motion fields in 8 healthy subjects with test-retest reliability evaluated through repeated scans.Poroelastic modeling: Brain tissue is modeled as a poroelastic continuum, with a porous elastic matrix fully saturated an infiltrating pore fluid. The steady-state harmonic equations representing pulsatile dynamics[3] is given by
$$\nabla \cdot (\mu (\nabla u +\nabla u^T)) +\nabla (\lambda \nabla \cdot u) - (1-\beta)\nabla P = -\omega^2(\rho-\beta\rho_f)u$$
$$\nabla \cdot \beta \nabla P + \rho_f \omega^2 \nabla \cdot ((1-\beta)u)=i\omega \rho_f \gamma$$
$$\beta= \frac{\omega \phi^2 \rho_f \kappa}{i \phi^2 +\kappa \omega (\rho_a +\phi \rho_f)}$$
Here, the shear modulus, μ , Lame parameter, λ , and solid displacement field, u, are properties of the porous solid phase, and $$$\rho, \rho_f$$$ and $$$\rho_a$$$ are the bulk, fluid and apparent densities, and the coupling of the solid and fluid phases are described by hydrodynamic parameters including pore fluid pressure field, P, porosity, φ , hydraulic conductivity, κ , and fluid source, γ .
Assimilation of MRI data into computational model: The driving source of pulsatile motion is primarily the movement of pressurized blood. Accurate modeling of blood through a full arterial tree at brain scale is currently not possible. To circumvent these limitations we opt to fit local values of the fluid source term, γ , to reproduce the observed pulsatile motions in a physiologically relevant way. Generalized least squares (GLS) is used with careful selection of the GLS weighting matrix to ensure that the only forcing in the system comes from the local blood pulsatile pressure[4].
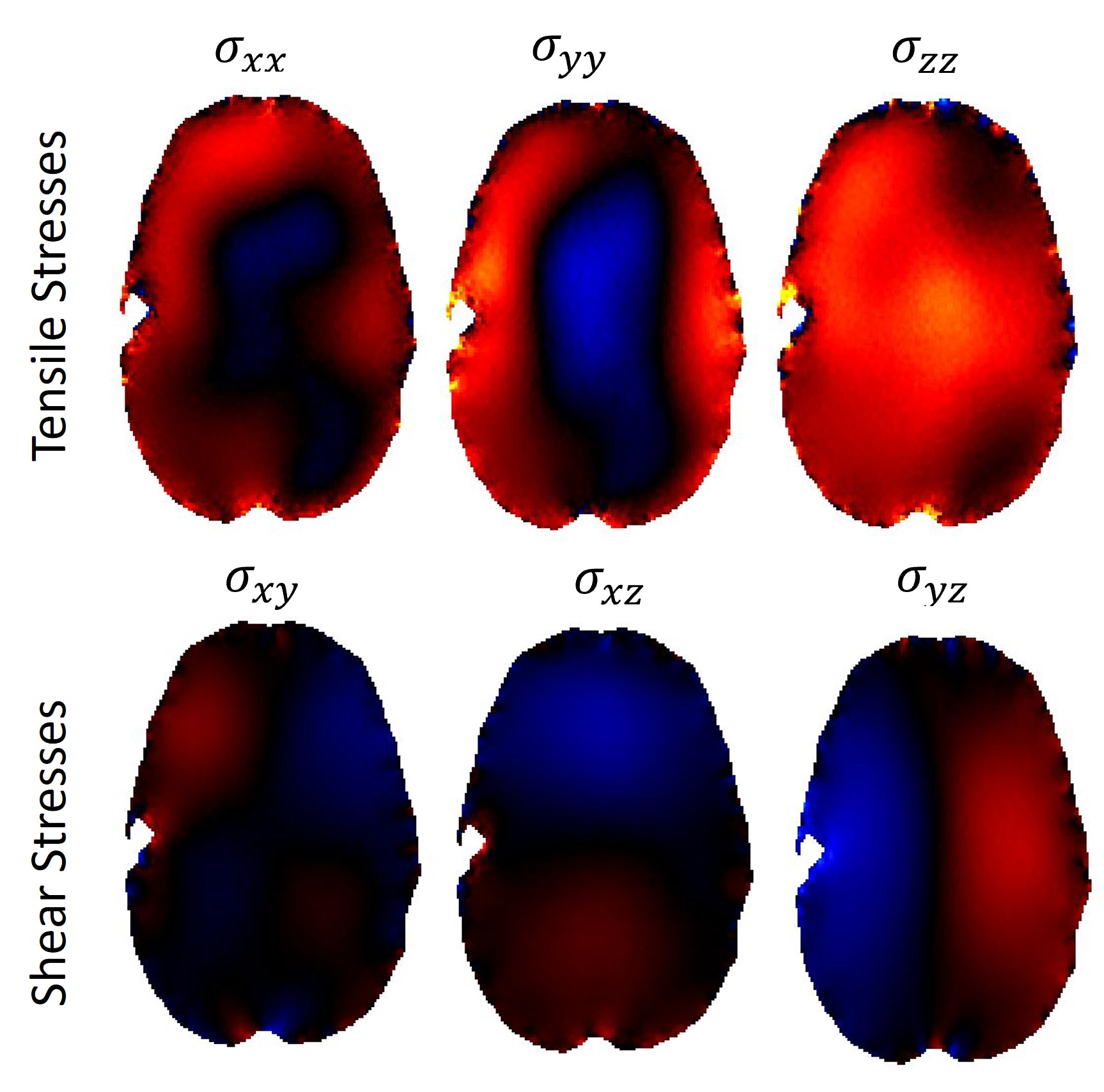
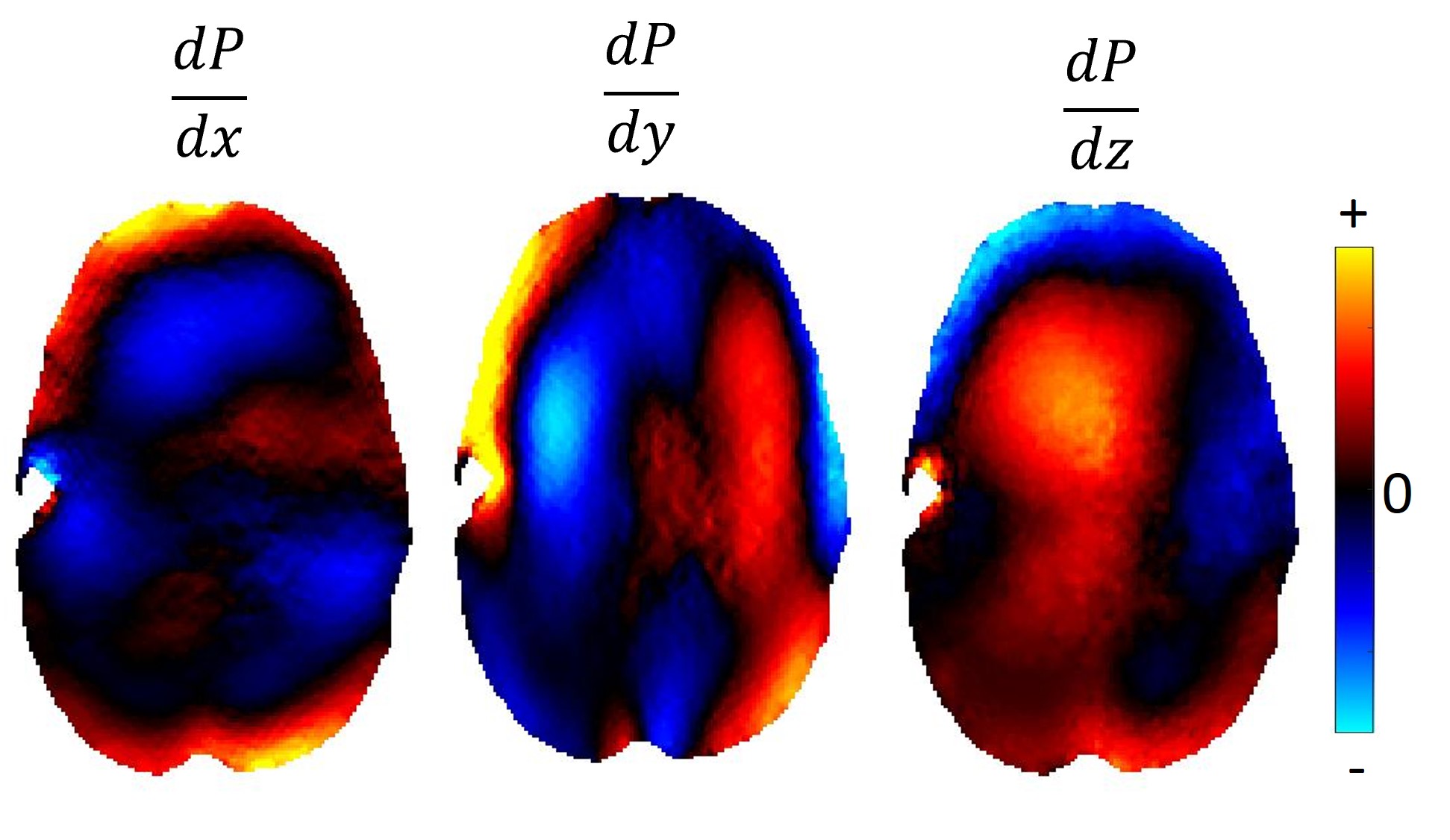
Stress and pressure gradient computation: After the GLS process, we have a poroelastic model which has been fitted to patient-specific data, and we can use this model to compute parameters which are not directly measurable. The two important factors which drive the ISF flow are the solid stress tensor, $$$\sigma$$$, and the fluid pressure gradient, $$$\nabla P$$$. A Galerkin weighted residual method was used to smooth out discontinuities in the finite element representation to compute $$$\nabla P$$$, and the material strain, $$$\epsilon_{ij}$$$. The stress in the porous isotropic solid was calculated by
$$\sigma_{ij}=2\mu \epsilon_{ij} + \lambda \delta_{ij} \epsilon_{kk}$$
RESULTS AND DISCUSSION
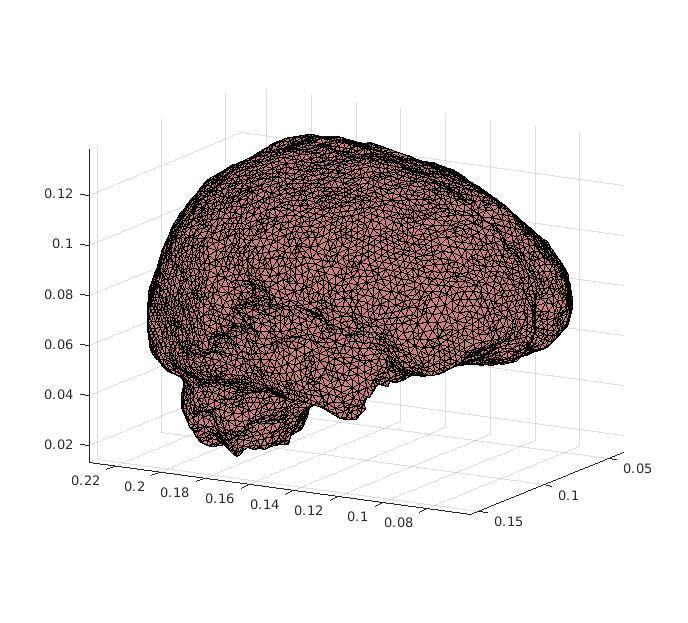
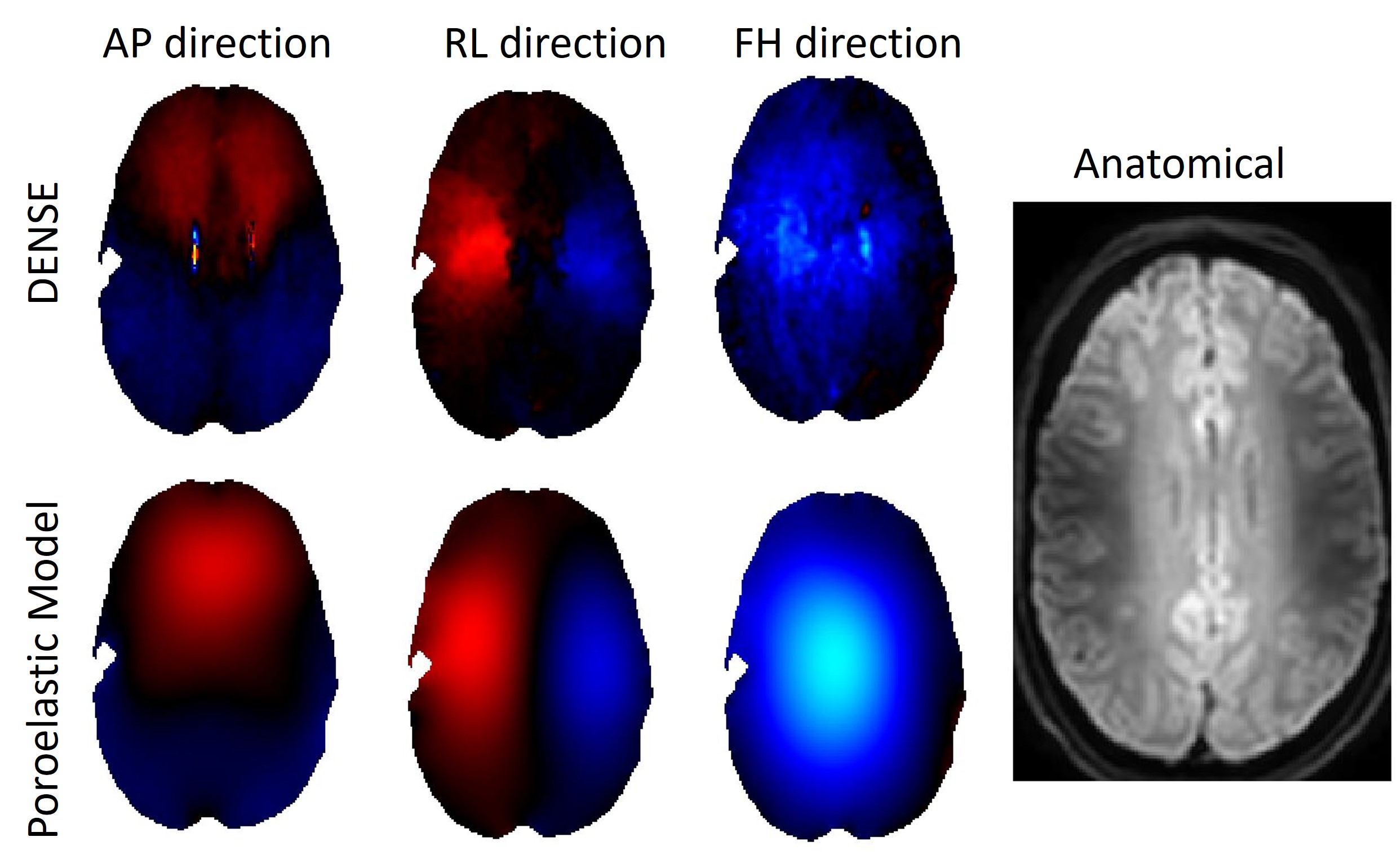
The finite element mesh used for the computations is shown in figure 1. The pulsatile motion fields from experimental DENSE measurements and the fitted model displacements are shown in figure 2. Components of the fluid pressure gradient are shown in figure 3, and the 6 components of the stress tensor for the porous elastic matrix are shown in figure 4. Future work will use these driving forces can be used to estimate the much slower and smaller scale flow of ISF using the equations defining multifluid poroelastic models.Acknowledgements
No acknowledgement found.References
[1] Adams, A.L., Kuijf, H.J., Viergever, M.A., Luijten, P.R. and Zwanenburg, J.J., 2019. Quantifying cardiac‐induced brain tissue expansion using DENSE. NMR in Biomedicine, 32(2), p.e4050.
[2] Adams, A.L., Viergever, M.A., Luijten, P.R. and Zwanenburg, J.J., 2020. Validating faster DENSE measurements of cardiac-induced brain tissue expansion as a potential tool for investigating cerebral microvascular pulsations. Neuroimage, 208, p.116466.
[3] Perriñez, P.R., Kennedy, F.E., Van Houten, E.E., Weaver, J.B. and Paulsen, K.D., 2008. Modeling of soft poroelastic tissue in time-harmonic MR elastography. IEEE transactions on biomedical engineering, 56(3), pp.598-608.
[4] Lynch, D.R., 2004. Numerical partial differential equations for environmental scientists and engineers: a first practical course. Springer Science & Business Media.
Figures