0668
Brain arterial remodeling and incident dementia: the Atherosclerosis Risk in Communities (ARIC) Study1Deptartment of Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Deptartment of Biomedical Engineering, University of North Carolina & North Carolina State University, Chapel Hill, NC, United States
Synopsis
Keywords: Dementia, Blood vessels, MRA
Motivation: We aimed to address the gap in understanding the neurovascular contributions to dementia risk in a US community-based study, recognizing the need to consider arterial geometry factors and cerebral small vessel disease (CSVD).
Goal(s): Our study sought to investigate the relationship between brain arterial remodeling and incident dementia risk, focusing on how arterial geometry and CSVD factor into this complex equation.
Approach: Our approaches involved analyzing data from a US community-based study to assess the impact of arterial remodeling, arterial geometry, and CSVD on dementia risk.
Results: Our study's core findings indicate an increased risk of incident dementia associated with brain arterial remodeling.
Impact: Our model is promising for the prediction of cognitive decline and dementia diagnosis based on the MRA measurements.
Introduction
Vascular aging in intracranial arteries is associated with medial fragmentation and collagen deposition and may present as either outward or tortuous arterial remodeling, both of which may occur in the absence of atherosclerosis1,2. Brain arterial outward remodeling (i.e, larger diameters) has been reported as a marker of poor cognitive outcomes3.4, but the role of tortuous remodeling and their combined effects remains unknown, in particular in the general population. We sought to determine the risk of incident dementia from brain arterial remodeling in a US community-based cohort, the Atherosclerosis Risk in Communities (ARIC) study.Methods
Intracranial arterial size (area and diameter) and tortuosity (angle metric AM, distance metric DM, and distance-to-axis metric DTA) were measured for eight standard vessel segments on brain TOF MRA (acquired resolution, 0.50×0.50 mm2; slice thickness 0.55 mm) acquired in 1,980 ARIC participants from 2011 through 20135. Participants free of dementia and without missing covariates were followed through 2019 until the development of dementia (incident dementia, adjudicated by experts6). The globle geometry measurments (sum from eight vessel segments) were used for the participant-based analysis. Associations between arterial size/tortuosity and incident dementia were assessed using Cox proportional hazard ratios (HR) adjusted for cerebral small vessel disease (CSVD) (characterized by white matter hyperintensities, lacunar infarctions, and microhemorrhages), prevalent stroke, APOE4 genotype, and cardiovascular risk factors. Additionally, multivariable linear regression was used to estimate average differences in arterial size and tortuosity as a function of follow-up cognitive performance (measured as cognitive factor scores).Results and Discussion
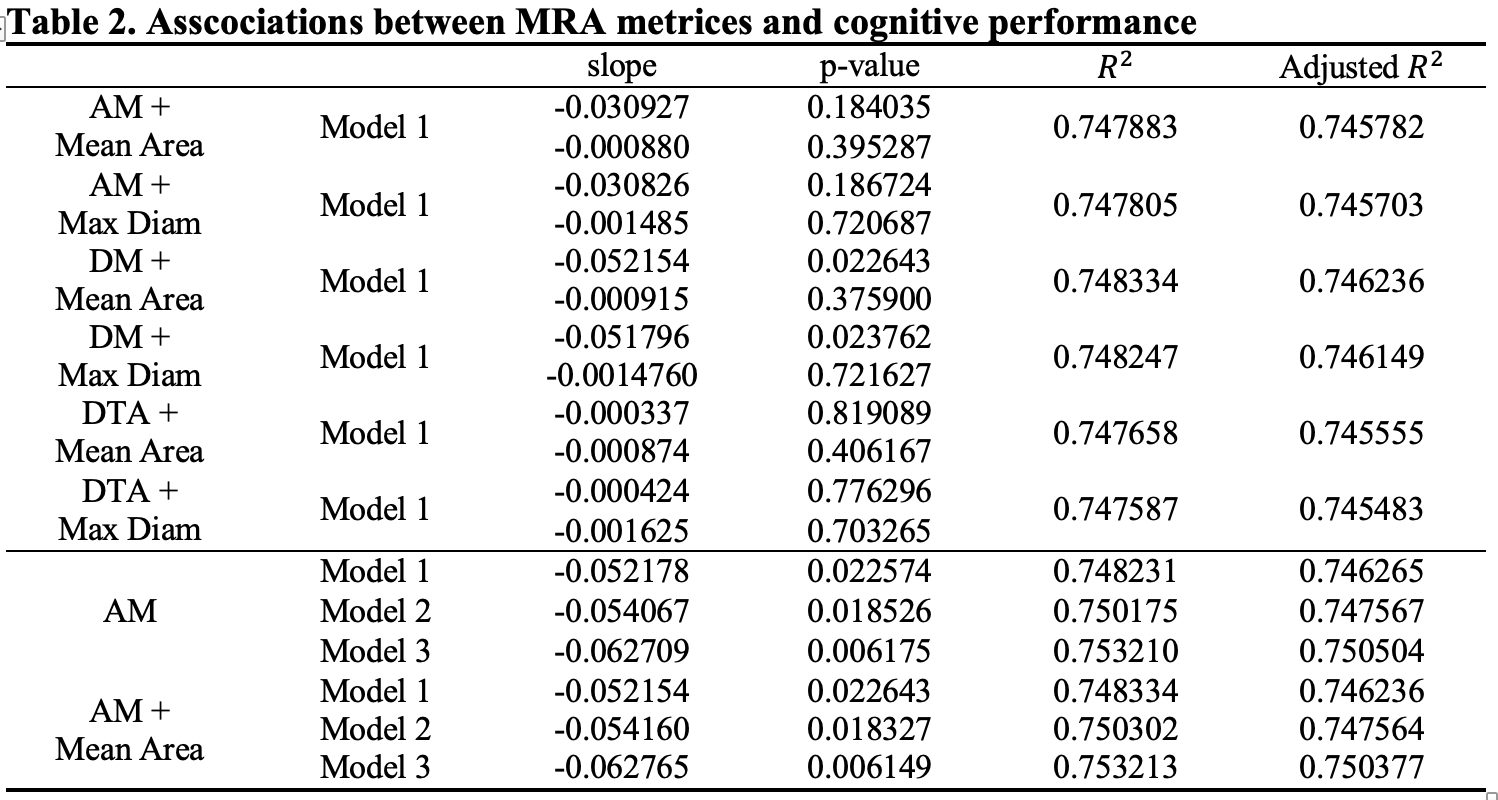
A total of 1,908 participants (age 67-90 years; 1130 women; 554 black) were included in this cross-sectional study. During a median follow-up of 5.6 years (maximum 8.0 years), we identified 100 cases of incident dementia among 916 non-dementia case at the beginning. In fully adjusted models that included markers of CSVD, the HR (95% CI) for incident dementia was 1.56 (1.16, 2.10) (Table 1) with one unit change of DM-calculated total tortuosity. The first model performed relatively good with adjustment to age, gender, race and APOE4 genotype. Both the HR value larger than 1 and the p-value smaller than 0.05 showed that the tortuosity metrics, especially DM-calculated total in this case, could be used for predicting the dementia incident. In the second model, when adjusted to both demographic factors and cardiovascular risk factors, the adding risk factors caused the changes in predictor’s asscocitation with the dementia diagnosis, which was reflected in the p-value larger than 0.05.When the global function score was considered as primay outcome, AM-calculated total tortuosity was a good predictor of cognitive function score for all three adjusted models (p-value < 0.05 for model 1 and model 2, p-value < 0.01 for model 3, R2 around 0.75), with slight model performance improving with the addition of lumen area or maximum diameter (Table 2). The combination of AM tortuosity and maximum diameter with model 3 adjusted to all factors outperformed than the other predictiors (p-value_tor=0.0055 and R2=0.7504).
Conclusion
In conclusion, brain arterial tortuosity remodeling was associated with an increased risk of incident dementia independent of CSVD, prevalent stroke, APOE4 genotype, and cardiovascular risk factors. Our results indicate that arterial geometry factors, including both arterial diameter and tortuosity, may play a role in vascular contribute to cognitive decline.Acknowledgements
No acknowledgement found.References
1. Shirwany NA, Zou MH. Arterial stiffness: a brief review. Acta Pharmacol Sin. 2010; 31: 1267-1276.
2. Duca L, Blaise S, Romier B, Laffargue M, Gayral S, El Btaouri H, Kawecki C, Guillot A, Martiny L, Debelle L, Maurice P. Matrix ageing and vascular impacts: focus on elastin fragmentation. Cardiovasc Res. 2016; 110: 298-308.
3. Gutierrez,Jose, Cheung,Ken, Bagci,Ahmet, Rundek,Tatjana, Alperin,Noam, Sacco,Ralph, Elkind,Mitchell, Wright,Clinton. Brain Arterial Diameters as Biomarkers of Cognitive Performance: Results from the Northern Manhattan Study (P2.246). Neurology. 2016; 16: Supplement.
4. Gutierrez J, Kulick E, Park Moon Y, Dong C, Cheung K, Ahmet B, Stern Y, Alperin N, Rundek T, Sacco RL, Wright CB, Elkind MSV. Brain Arterial Diameters and Cognitive Performance: The Northern Manhattan Study. J Int Neuropsychol Soc. 2017; 1-12.
5. Zhou S, Qiao Y, Zhou X, Wasserman BA, Caughey MC. Detection of Dolichoectasia and Atherosclerosis by Automated MRA Tortuosity Metrics in a Population-Based Study. J Magn Reson Imaging. 2023 Jul 28. doi: 10.1002/jmri.28923. Epub ahead of print. PMID: 37515312.
6. Schneider AL, Sharrett AR, Gottesman RF, Coresh J, Coker L, Wruck L, Selnes OA, Deal J, Knopman D, Mosley TH. Normative data for 8 neuropsychological tests in older blacks and whites from the atherosclerosis risk in communities (ARIC) study. Alzheimer Dis Assoc Disord. 2015;29:32-44.Figures
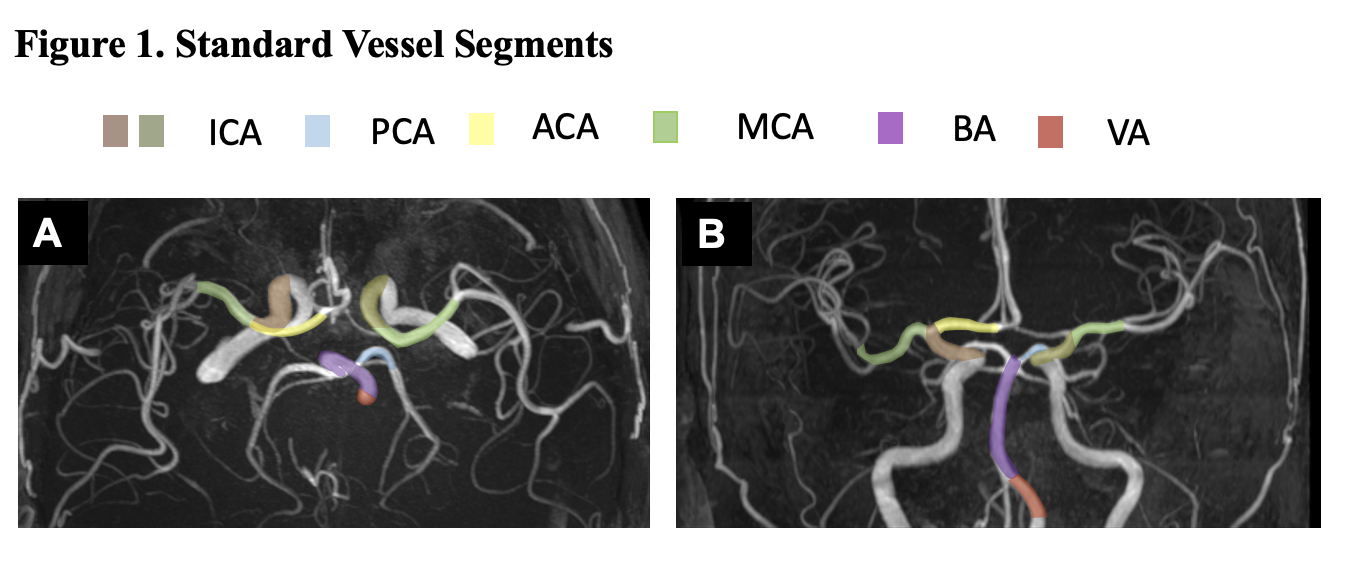
Standard vessel segments:
Supraclinoid internal carotid artery (ICA),
M1 segment of the middle cerebral artery (MCA),
Dominant A1 segment of the anterior cerebral artery (ACA)
P1 segment of the posterior cerebral artery (PCA),
Basilar artery (BA)
Dominant V4 segment of the vertebral artery (VA)
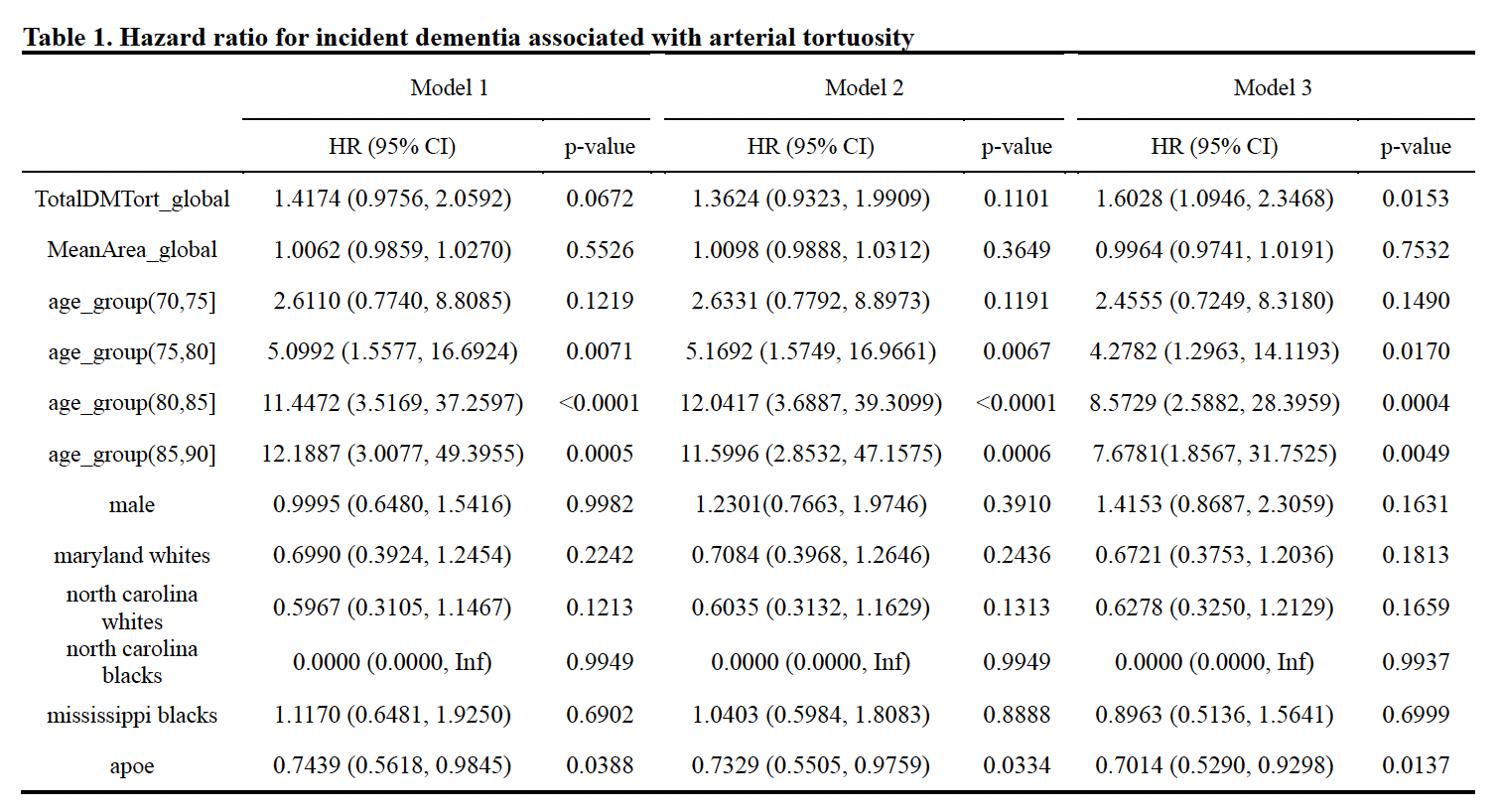
Model 1 adjusted for demographic risk factors including age, sex, race/center (Minnesota Whites, Maryland Whites, North Carolina Whites/Blacks, Mississippi Blacks), education (<high school, high school, >high school), and APOE4 status (yes, no).
Model 2 additionally adjusted for ever smoking (yes, no), BMI, systolic blood pressure, HDL, LDL, history of diabetes (yes, no), CHD (yes, no), stroke (yes, no), and total intracranial volume.
Model 3 additionally adjusted for white matter hyperintensity percentage, number of subcortical infarcts and number of microhemorrhages.
Model 1 adjusted for demographic risk factors including age, sex, race/center (Minnesota Whites, Maryland Whites, North Carolina Whites/Blacks, Mississippi Blacks), education (<high school, high school, >high school), and APOE4 status (yes, no).
Model 2 additionally adjusted for ever smoking (yes, no), BMI, systolic blood pressure, HDL, LDL, history of diabetes (yes, no), CHD (yes, no), stroke (yes, no), and total intracranial volume.
Model 3 additionally adjusted for white matter hyperintensity percentage, number of subcortical infarcts and number of microhemorrhages.