0655
Accelerating DT-CMR with Deep Learning-based Tensor De-noising and Breath Hold Reduction1Imperial College London, London, United Kingdom, 2Royal Brompton Hospital, London, United Kingdom, 3Technische Universität München, Munich, Germany
Synopsis
Keywords: Analysis/Processing, Machine Learning/Artificial Intelligence
Motivation: DT-CMR can revolutionise diagnosis and treatment of heart conditions by non-invasively imaging cardiomyocyte microstructure, but currently long acquisition times prevent clinical use.
Goal(s): Reduce the number of breath-holds required for in-vivo DT-CMR acquisitions, resulting in significantly reduced scan times with minimal image quality loss.
Approach: We developed a deep learning model based on Generative Adversarial Networks, Vision Transformers, and Ensemble Learning to de-noise diffusion tensors computed from reduced-repetition DT-CMR data. We compared model performance to conventional linear fitting methods and a baseline deep learning approach.
Results: Our model reduced noise over 20% compared to previous state-of-the-art approaches while retaining known clinically-relevant myocardial properties.
Impact: This breakthrough in DT-CMR acquisition efficiency could enable rapid microstructural phenotyping of the myocardium in the clinic for the first time, revolutionising personalised diagnosis and treatment by unlocking DT-CMR’s ability to non-invasively characterise heart muscle organisation at the cellular level.
Background
Diffusion Tensor Cardiac Magnetic Resonance (DT-CMR) non-invasively provides unique insights into 3D myocardial microstructural organisation of cardiomyocytes underlying healthy and pathological hearts. However, acquiring whole-heart DT-CMR currently requires approximately 60 minutes of scanning time due to the necessity to repeat each slice acquisition multiple times over separate breath-holds to boost the inherently low signal-to-noise ratio (SNR). This prevents clinical translation of this promising technique that has demonstrated substantial value for phenotyping hypertrophic cardiomyopathies, acute myocardial infarction, dilated cardiomyopathies and other conditions in research studies [1,2].The lengthy acquisition duration stems from the intrinsically low SNR of diffusion MRI, which measures signal loss produced by diffusion motion. Cardiac motion artefacts and bulk respiratory motion compounds the challenge. As a result, DT-CMR research protocols typically involve around 12 breath-hold repetitions of each slice position, requiring approximately 60 breath-holds in total for whole-heart coverage (5 slices).
Recent studies have proposed using deep learning to denoise DT-CMR derived parameter maps after reconstruction from reduced repetition data as one approach to accelerate acquisitions [3,4]. However, maps directly optimised from sparse noisy data can still contain artefacts and underestimate abnormalities.
We propose an alternative paradigm where deep learning models directly denoise diffusion tensors prior to map calculation. This allows leveraging the latest advancements in deep image restoration techniques, which we adapt to operate on diffusion tensors rather than conventional images.
Methods
We retrospectively analysed 744 cardiac DT-CMR datasets including 197 healthy volunteers and 547 patients exhibiting pathologies like hypertrophic cardiomyopathy and myocardial infarction. Diffusion weighted images were acquired with 12±2 total breath-hold repetitions.The images were acquired with a diffusion weighted stimulated echo acquisition mode (STEAM) single shot echo planar imaging (EPI) sequence with reduced phase field-of-view and fat saturation at a spatial resolution of 2.8 x 2.8 x 8.0 mm^3. Diffusion was encoded in six directions with diffusion-weightings of b=150 and 600 s/mm^2 in a short-axis mid-ventricular slice. Additionally, reference images were also acquired with minimal diffusion weighting, named here as “b0" images.
We emulated prospective accelerated scans by extracting data from only the first 1, 3, or 5 breath-holds (1BH, 3BH, 5BH) using different sampling strategies. The training was performed on 80% of the available datasets, 10% were used as validation and 10% were used for the final testing of the model.
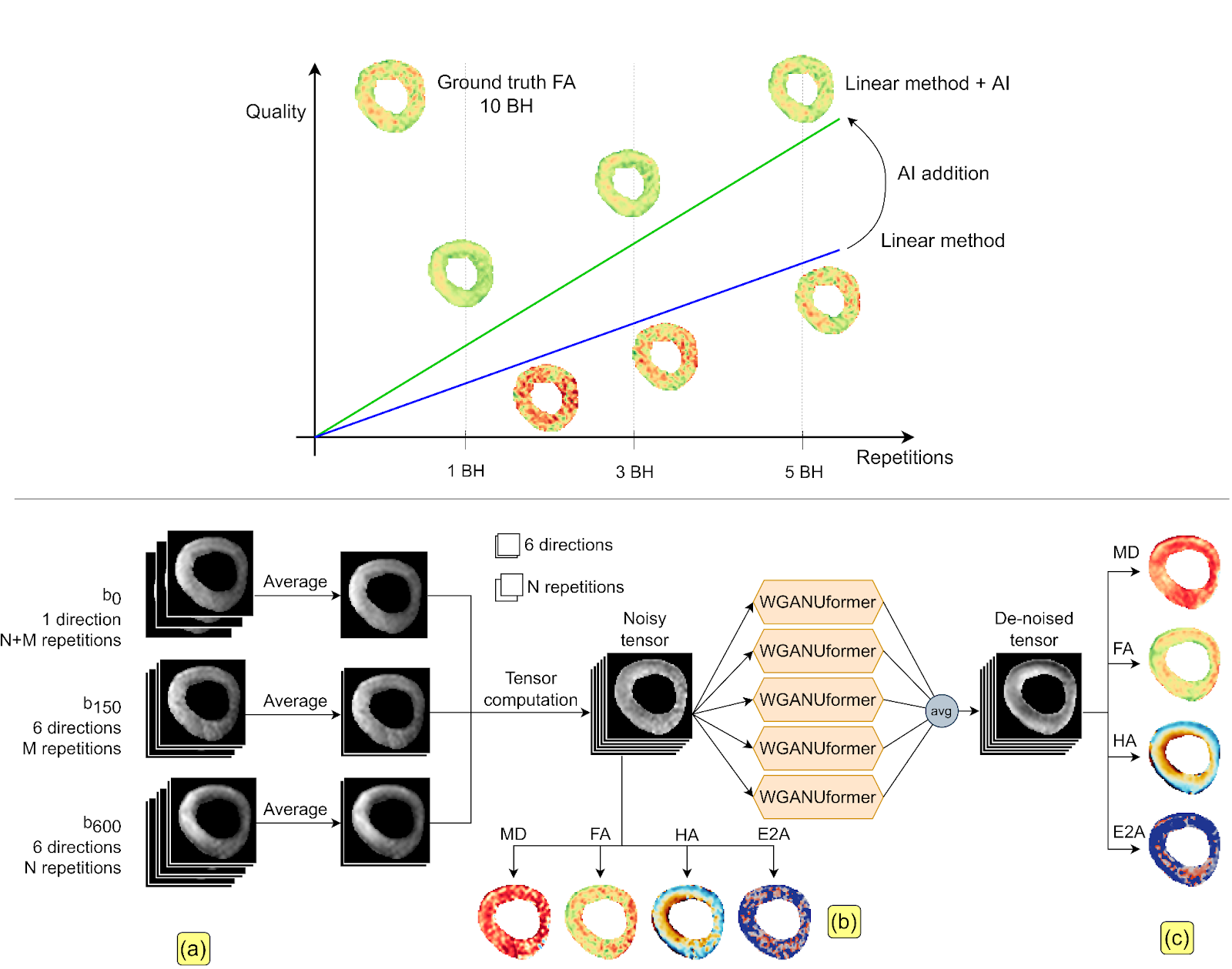
A Generative Adversarial Network (GAN) framework was developed, wherein the generator employed a U-Former architecture [5], while the discriminator followed a PatchGAN design (refer to Figure 1). The U-Former incorporated a U-shaped encoder-decoder with a local attention mechanism, enabling memory-efficient image restoration while leveraging the strengths of transformers. We trained five distinct models on paired noisy and reference tensors, subsequently ensembling them to yield robust predictions. Additionally, we implemented several enhancements, including tensor-to-tensor training, channel normalisation, and data augmentation utilising multiple random subsets of repetitions during training. Our proposed method, denoted as WGUFx5, underwent a comparative analysis with classical tensor fitting (i.e., Linear Least Squares or LLS) and a U-Net based model [3], which computed de-noised diffusion tensors from reduced-repetition images.
Results
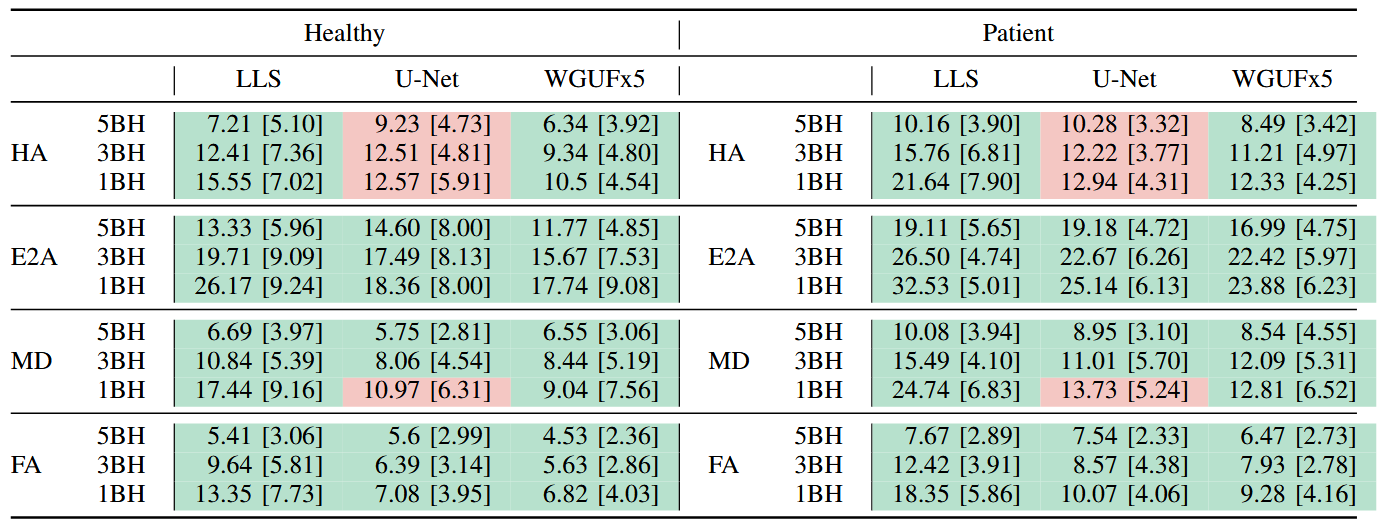
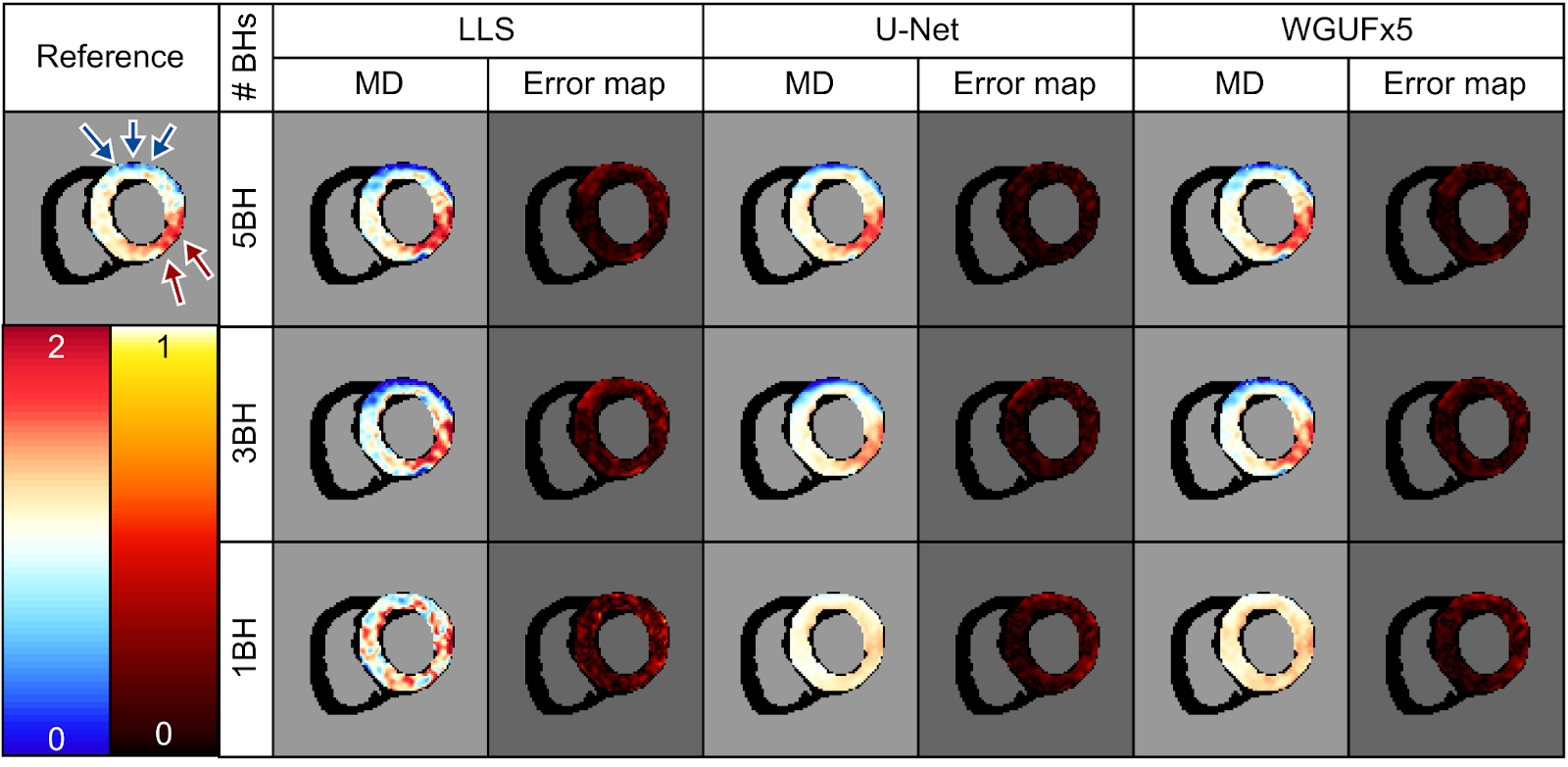
Our proposed technique substantially decreased noise and improved accuracy of DT-CMR parameter maps compared to conventional fitting and prior deep learning methods, especially for very low repetition data.Median errors reduced by up to 17% for Mean Diffusivity (MD), 16% for Fractional Anisotropy (FA), 21% for Helix Angle (HA), and 12% for transverse angle (E2A) compared to the previous state-of-the-art (Fig. 2, Fig. 3). Known diffusion DT-CMR properties were preserved, including transmural helix angle progression and elevated FA in the mesocardium. Remote and infarcted regions remained differentiable by higher MD in the infarct (Fig. 4).
On prospective validation data from 25 additional scans, median errors reduced by 29-53% versus standard fitting. The model performed well even in patients with cardiac abnormalities, although errors were slightly higher compared to healthy volunteers.
Conclusion
Directly denoising diffusion tensors enables better data augmentation procedures and leverages extensive image denoising literature. Our proposed improvements to model architecture, training procedure, and pre-processing demonstrate the capability to substantially accelerate DT-CMR acquisitions. However, errors were still higher for clinical patients compared to volunteers, especially from highly accelerated 1 breath-hold acquisitions.This highlights the need for expanding dataset diversity and modifying models to improve generalisation to variable pathology manifestations before clinical translation. Overall this work represents major progress towards realising the full potential of DT-CMR for phenotyping numerous cardiomyopathies. Further prospective studies on larger cohorts are warranted to prepare this promising technique for deployment in routine clinical practice.
Acknowledgements
This work was supported by the British Heart Foundation (RG/19/1/34160). Guang Yang was supported in part by the ERC IMI (101005122), the H2020 (952172), the MRC (MC/PC/21013), the Royal Society (IEC/NSFC/211235), the NVIDIA Academic Hardware Grant Program, the SABER project supported by Boehringer Ingelheim Ltd, and the UKRI Future Leaders Fellowship (MR/V023799/1). Michael Tänzer was supported by the UKRI CDT in AI for Healthcare (EP/S023283/1).
References
[1] Nielles-Vallespin et al. Assessment of Myocardial Microstructural Dynamics by In Vivo Diffusion Tensor Cardiac Magnetic Resonance. Journal of the American College of Cardiology 2017.
[2] Khalique et al. Diffusion Tensor Cardiovascular Magnetic Resonance Imaging: A Clinical Perspective. JACC. Cardiovascular imaging 2020.
[3] Ferreira et al. Accelerating Cardiac Diffusion Tensor Imaging With a U-Net Based Model: Toward Single Breath-Hold. Journal of Magnetic Resonance Imaging 2022.
[4] Phipps et al. Accelerated in Vivo Cardiac Diffusion-Tensor MRI Using Residual Deep Learning-Based Denoising in Participants with Obesity. Radiology: Cardiothoracic Imaging. 2021.
[5] Wang et al. Uformer: A General U-Shaped Transformer for Image Restoration. arXiv preprint arXiv:2106.03106 2021.
Figures