0640
Quantitative 3D T2* Mapping of Meniscus Before and After Meniscal Root Repair at 7 Tesla1Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, 2Department of Radiology, University of Minnesota, Minneapolis, MN, United States, 3Department of Biomedical Engineering, Cleveland Clinic, Cleveland, OH, United States, 4Diagnostic Radiology, Oregon Health & Science University, Portland, OR, United States, 5Twin Cities Orthopedics, Minneapolis, MN, United States
Synopsis
Keywords: Other Musculoskeletal, MSK, Meniscus
Motivation: Meniscal tears are a significant cause of osteoarthritis, and failure rate of meniscal repair remains high. MRI assessment of meniscus at 7T provides high signal-to-noise ratio and allows 3D evaluation of the tissue.
Goal(s): Investigate and follow-up meniscal tissue integrity in pre- and post-repair patients.
Approach: Quantitative 3D T2* mapping of the lateral and medial menisci in patients with posterior horn root tears in the medial meniscus and compare against matched controls.
Results: Significantly increased T2* values were identified beyond the tear in both lateral and medial menisci of pre-repair patients and the values remained significantly elevated six months post-repair.
Impact: Utilizing high-resolution 7 Tesla 3D T2* mapping, this study quantitatively and longitudinally assesses meniscal tissue integrity of patients who underwent medial meniscal posterior root tear repair, which has significant impact on management and standard of care for the patients.
Introduction
The menisci play a crucial role for the long-term maintenance and functional integrity of the knee joint. They provide joint stability and shock absorption. Strong forces that exceed the maximum tensile strength of the menisci, such as knee twisting or sudden forces, can lead to meniscal tears. In particular, medial meniscus posterior horn root tears (MMPRT) are a significant source of pain and dysfunction and are associated with meniscal extrusion and development of osteoarthritis (OA)1. Quantitative MRI T2 and T2* relaxation time mapping have been associated with histologically verified meniscal degeneration, specifically collagen fiber organization2, 3. Previous studies have reported elevated T2* in the menisci of patients with knee OA and anterior cruciate ligament (ACL) injuires4, 5. The goal of this study is to assess the meniscal tissue integrity with quantitative 3D T2* mapping in patients with MMPRT before and six months after the meniscal root repair. We hypothesize that disorganization of the collagen fiber in the menisci of the patients caused by MMPRT will increase the T2* values before and after the meniscal repair.Methods
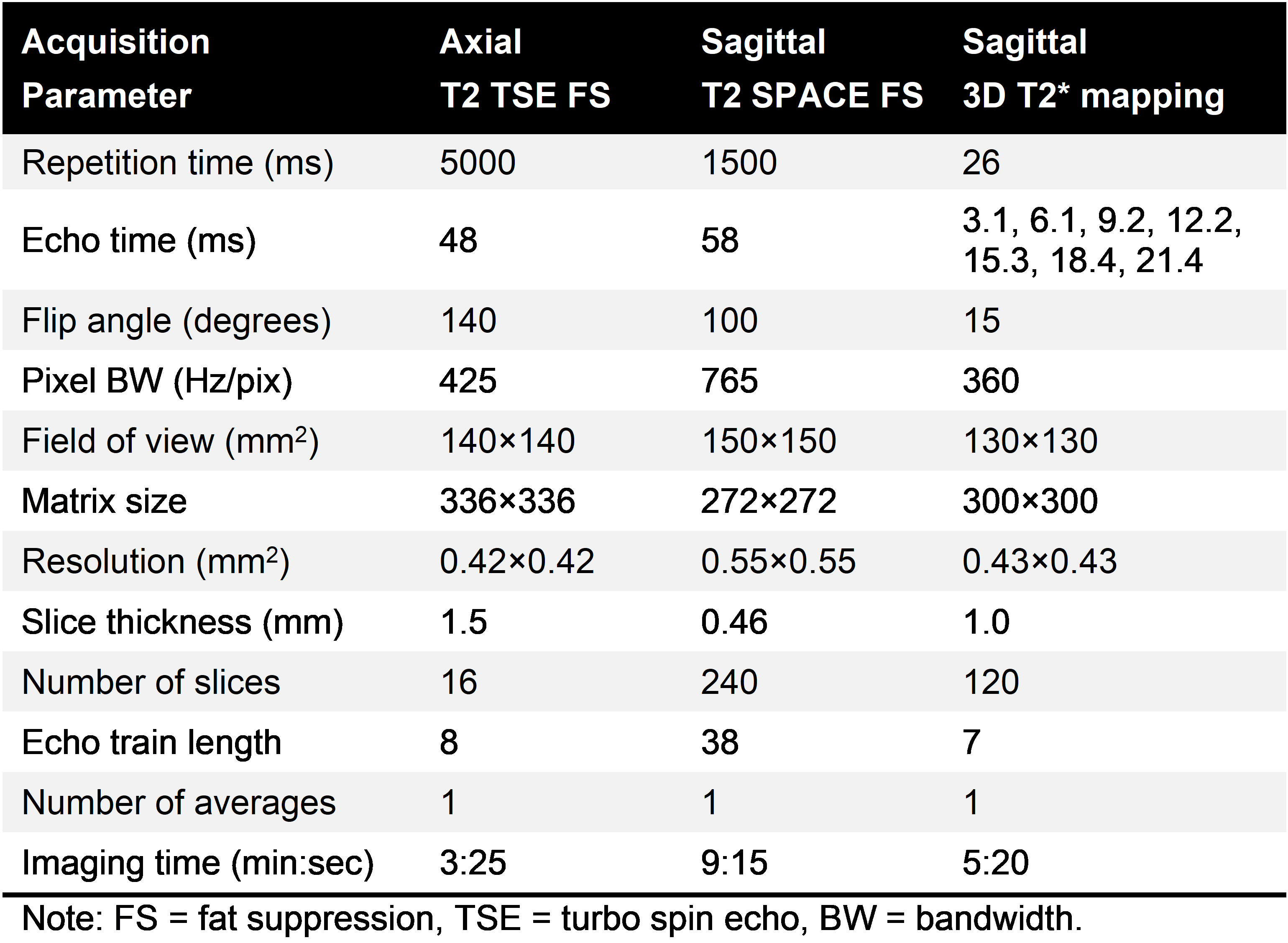
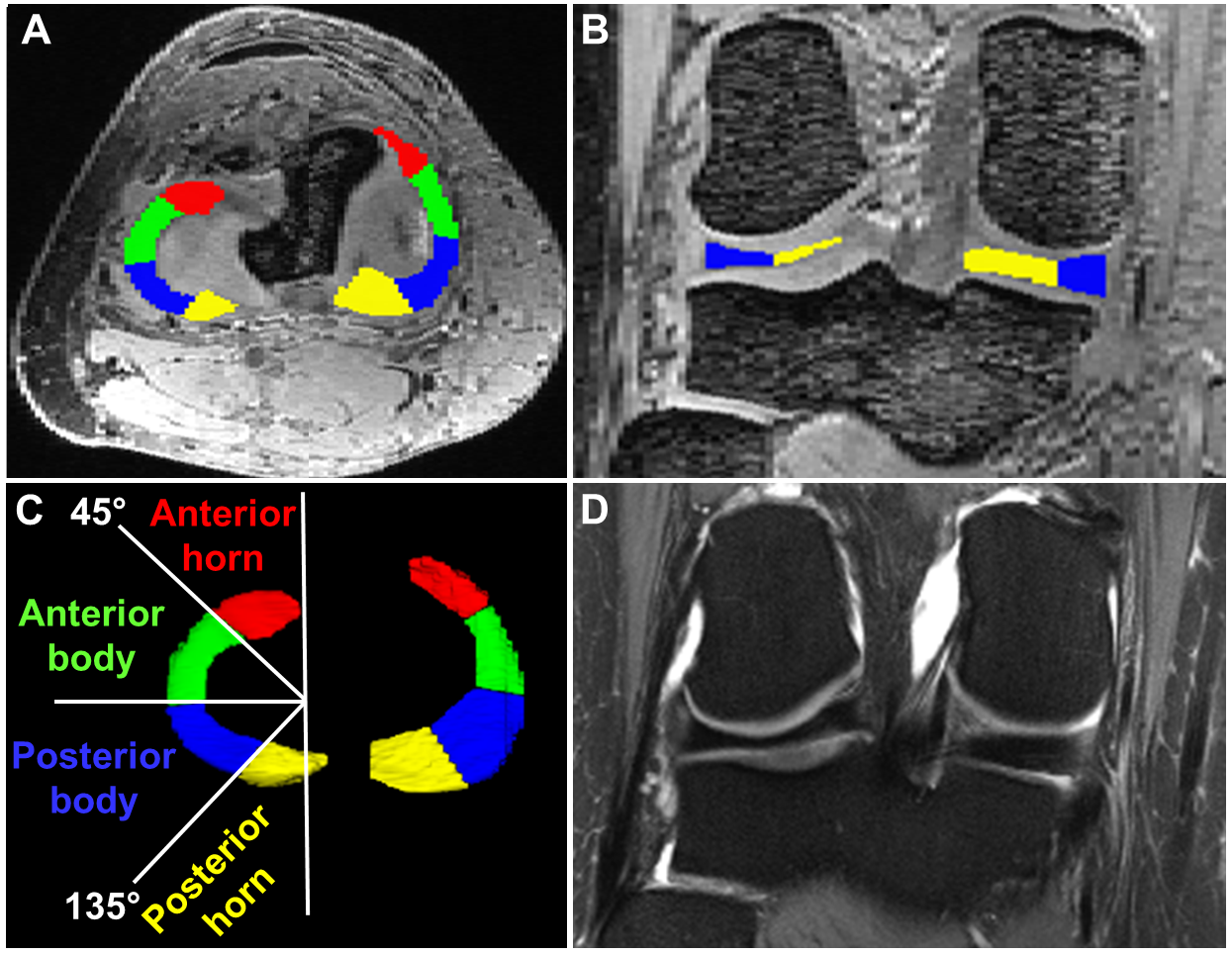
This is an IRB approved and HIPPA compliant longitudinal study. Ten patients (mean age: 51 years; age range: 34-62 years; mean body mass index (BMI): 30 kg/m2, 9 females) with a unilateral MMPRT and nine asymptomatic controls (mean age: 51 years; age range: 34-67 years; mean BMI: 26 kg/m2, 7 females) underwent 7T MRI. The same MRI protocol was repeated on the patients at 7T six months after the repair. The MRI protocol included morphological sequences (Fig. 1) and a quantitative 3D multi-echo gradient recalled echo (GRE) sequence with seven echo times (TE) between 3.1 and 21.4 ms. The sequence parameters are provided in figure 1. The T2* maps were calculated by fitting a mono-exponential signal decay of the multi-echo T2* data with a two-parametric least-square fitting routine in Matlab. The fitting accuracy was evaluated by calculating the root mean square error (RMSE) normalized to the estimated signal intensity at the echo time of 0 ms. The 3D segmentation of the medial and the lateral menisci was manually performed on the T2*-weighted images using ITK-SNAP (Fig. 2). Each meniscus was divided into four regions, including anterior horn (0°- 45°), anterior body (45°- 90°), posterior body (90°- 135°), and posterior horn (135°-180°) (Fig. 2). The median T2* values and the corresponding RMSE were measured in the four meniscal regions. A linear mixed effect model was used to compare the T2* values of the meniscal regions between the controls, pre-repair and post-repair patients. The p-values were adjusted for the pairwise comparisons between the four regions using Dunn-Bonferroni methods.Results
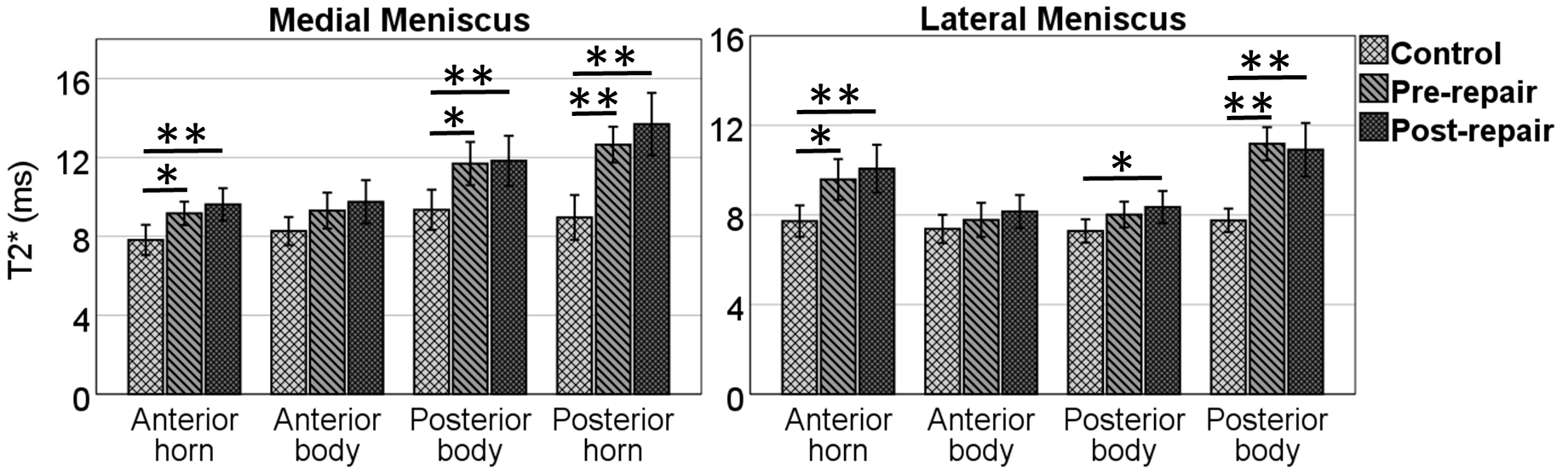
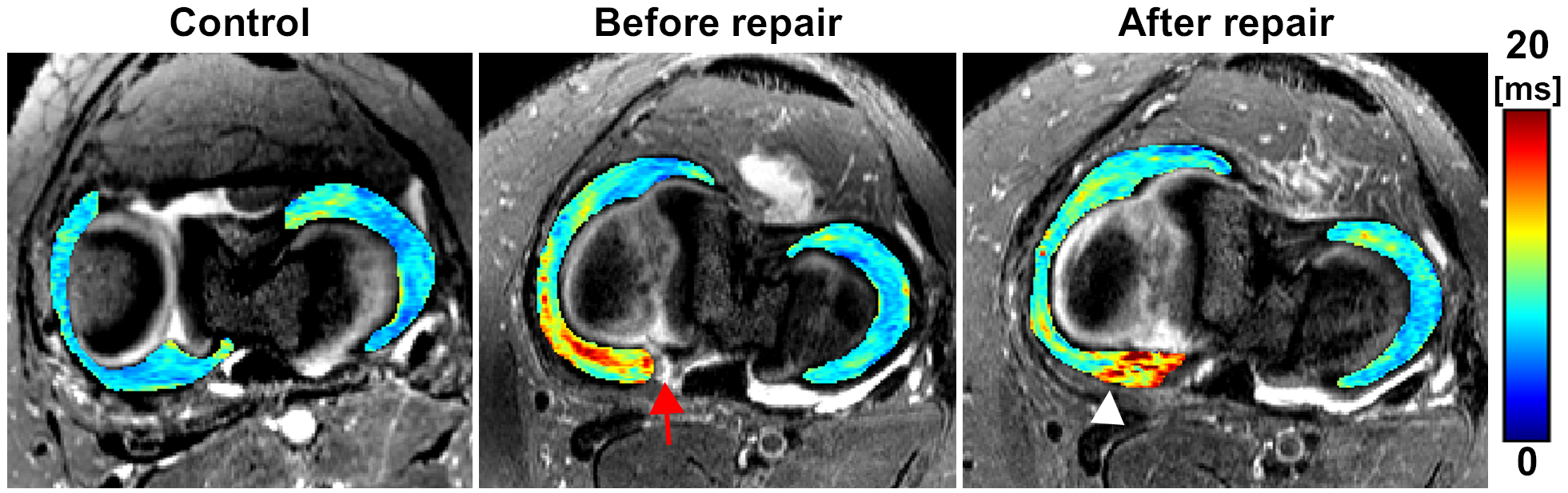
Significantly longer T2* relaxation times (p<0.05) were found in the anterior and posterior horn of both the lateral and medial menisci of the patient before and after the repair when compared to the same regions in the controls (Fig. 3). The highest differences in T2* values between controls, pre-repair and post-repair were found in the posterior horn of the medial meniscus where the tears were located, and the repair was performed (Figs. 3-4). Moreover, statistically significantly higher T2* values were also found in the posterior body of the medial meniscus of both pre- and post-repair patients compared to the controls. In the lateral meniscus, only post-repair patients had significantly higher T2* values in the posterior body. The mean normalized RMSE was below 4.1% for all regions, which demonstrates a good reliability of the fitting results.Discussion
Elevated T2* values in the anterior and posterior horns of patients’ menisci reflect the altered collagen fiber organization caused by the posterior root tears in the medial meniscus3, 4. These degenerative alterations are more pronounced in the posterior horn of the medial meniscus, where the MMPRT is located. The tears not only affected the medial but also the lateral meniscus, which had remained functionally intact. Despite some patients reporting improved knee function after the repair and during clinical examinations, the T2* values remained elevated indicating that the meniscus, once altered, takes longer than 6 months to regain its normal tissue integrity.Conclusion
Our findings are highly significant for patient treatment and management strategies since the success of surgical root repair relies on the longitudinal assessment of the menisci and the presence of healthy tissue at the repair site. The findings also suggest that more than six months are needed post-repair to allow the tissue to fully heal. Quantitative follow-up of meniscal composition with T2* mapping might therefore be useful indicator of the healing progression in the repaired meniscus root.Acknowledgements
National Institute of Biomedical Imaging and Bioengineering (P41 EB027061: Technology to Realize the Full Potential of UHF MRI), S10 OD025256 (7 Tesla Terra Instrument) and R01EB034575.References
1. Krych AJ, Johnson NR, Mohan R, Hevesi M, Stuart MJ, Littrell LA, Collins MS. Arthritis Progression on Serial MRIs Following Diagnosis of Medial Meniscal Posterior Horn Root Tear. J Knee Surg. 2018;31(7):698-704. Epub 20170926. doi: 10.1055/s-0037-1607038. PubMed PMID: 28950387.2. Eijgenraam SM, Bovendeert FAT, Verschueren J, van Tiel J, Bastiaansen-Jenniskens YM, Wesdorp MA, Nasserinejad K, Meuffels DE, Guenoun J, Klein S, Reijman M, Oei EHG. T(2) mapping of the meniscus is a biomarker for early osteoarthritis. Eur Radiol. 2019;29(10):5664-72. Epub 20190319. doi: 10.1007/s00330-019-06091-1. PubMed PMID: 30888480; PMCID: PMC6719322.
3. Einarsson E, Svensson J, Folkesson E, Kestila I, Tjornstrand J, Peterson P, Finnila MAJ, Hughes HV, Turkiewicz A, Saarakkala S, Englund M. Relating MR relaxation times of ex vivo meniscus to tissue degeneration through comparison with histopathology. Osteoarthr Cartil Open. 2020;2(2). Epub 2021/05/12. doi: 10.1016/j.ocarto.2020.100061. PubMed PMID: 33972933; PMCID: PMC7610736.
4. Olsson E, Folkesson E, Peterson P, Onnerfjord P, Tjornstrand J, Hughes HV, Englund M, Svensson J. Ultra-high field magnetic resonance imaging parameter mapping in the posterior horn of ex vivo human menisci. Osteoarthritis Cartilage. 2019;27(3):476-83. Epub 2018/12/16. doi: 10.1016/j.joca.2018.12.003. PubMed PMID: 30552967; PMCID: PMC7610687.
5. Williams A, Qian Y, Golla S, Chu CR. UTE-T2 * mapping detects sub-clinical meniscus injury after anterior cruciate ligament tear. Osteoarthritis Cartilage. 2012;20(6):486-94. Epub 20120118. doi: 10.1016/j.joca.2012.01.009. PubMed PMID: 22306000; PMCID: PMC5823016.
Figures