0639
Can MR only IR-UTE based BoneView imaging, along with routine MRI, be used to exclude sacroiliac joint (SIJ) pathologies without the need for X-Ray?1National Hospitals of Sri Lanka, Colombo, Sri Lanka, 2Philips, Bangalore, India, 3Philips, Gurugram, India
Synopsis
Keywords: Bone, Bone, UTE, MSK
Motivation: For a comprehensive diagnostic imaging investigation of SIJ, neither plain radiographs alone nor MRI alone provide sufficient specificity and sensitivity for accurate diagnosis of traumatic and/or non-traumatic sources of SIJ dysfunction.
Goal(s): Our goal is to show that using UTE based BoneView imaging technique, we can sufficiently detect enough structural radiological features of SIJ in non-pathological cases.
Approach: 24 patients with non-pathological SIJ were recruited for this study and inter-reader as well as inter modality agreement was computed based on a likert scale by two radiologists.
Results: There was high inter reader agreement as well as inter modality agreement.
Impact: MR only (IR-UTE based BoneView + routine MR) can be used to exclude patients with pathological SIJs and further investigation is necessary to extend the findings further to pathological cases as well.
Background
Sacroiliac joint (SIJ) pain is caused either due to pathologic changes or trauma to the SIJ complex and is a major cause of low back pain[1]. Sacroiliac joint pain mimics other pathologies resulting in a broad differential making accurate diagnosis more difficult[1][2]. While intraarticular SIJ blocks using local anesthetic injection are a diagnostic standard and are specific, these also tend to be less sensitive especially with the use of multiple injections[3]. Diagnostic imaging of SIJ is performed to rule out “red flags” such as fractures, malignancy, or infection. Typically, X-Ray is a first line of imaging for detection of structural lesions whereas MRI is the modality of choice for detection of active infectious and inflammatory lesions [4][5]. However, X-Rays expose the patients to ionizing radiation and have very low sensitivity [3]. Moreover, MRI is necessitated to rule out all the “red flags”, for prognostication and follow ups, making the diagnostic imaging process very cumbersome. In this study we explore whether Inversion Recovery UltraShort TE based BoneView (IR-UTE BoneView) MR[6] imaging can depict non-pathological SIJ structural radiological features as well as plain radiographs.Materials and Methods
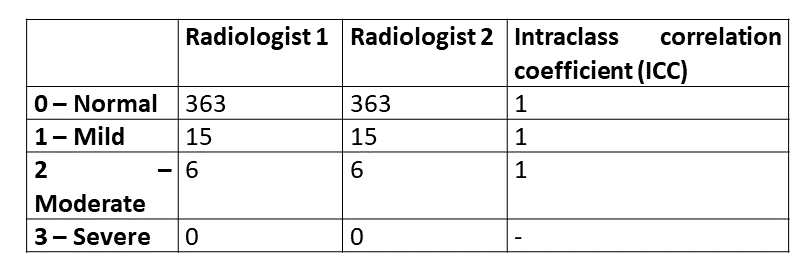
All MR imaging was performed on a Philips Ingenia 3.0T system (Best, NL) whereas X-Ray imaging was performed on Shimadzu 0.6/1.2P18DE-85 X-Ray system 2008 (Kyoto, Japan). Patients referred for imaging by the clinicians for low back pain were considered for this study. Patients with severe pathologies and prior surgical intervention for low back pain were excluded. Of these, patients whose SIJ images were severely corrupted by artifacts in IR-UTE BoneView images and/or plain radiograph were excluded. Written informed consent was obtained from all the patients. Patients underwent routine MR imaging protocol for SIJ in addition to the IR-UTE Boneview exam. The images were randomized and anonymized before independent and blinded examination by two experienced radiologists (25 years’ and 4 years’ experience) based on a 4-point likert scale (0-normal, 1-mild, 2-moderate, and 3-severe) for qualitative assessment. The parameters assessed on the likert scale were visualization of the left & right Anterior joint, left & right posterior joint, left & right lateral sub-articular region, and left & right medial sub-articular region.Results
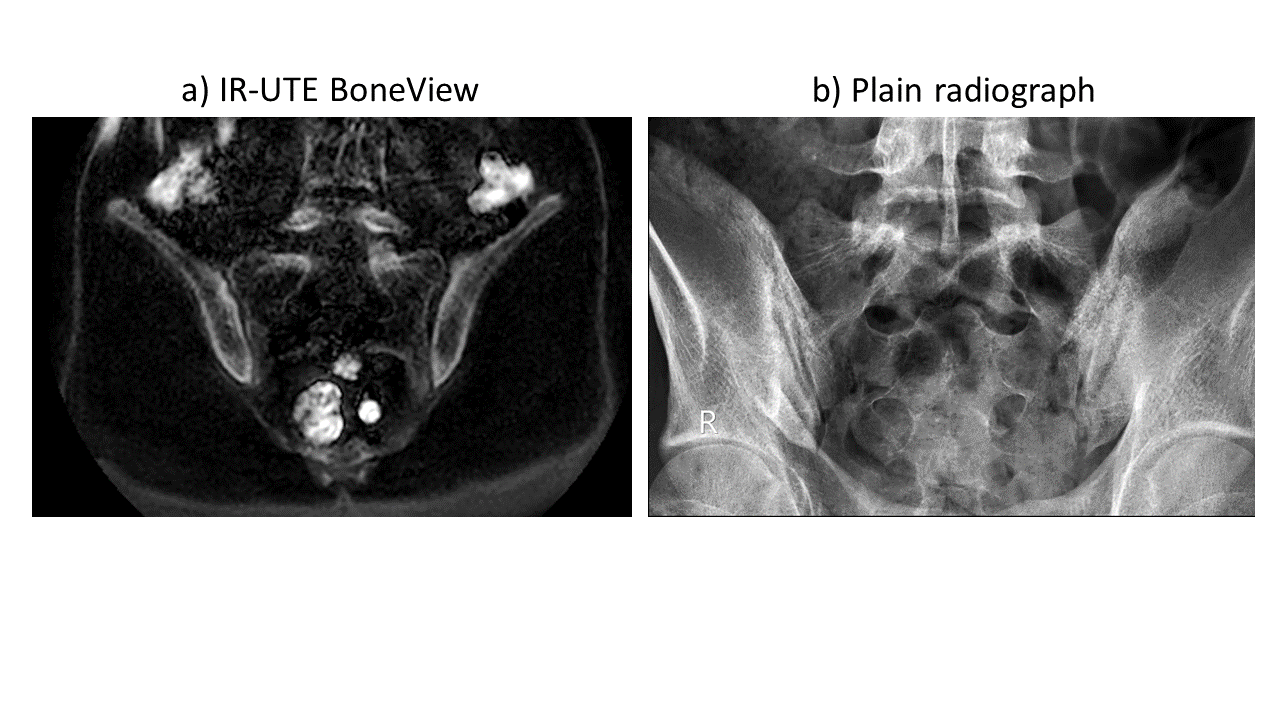
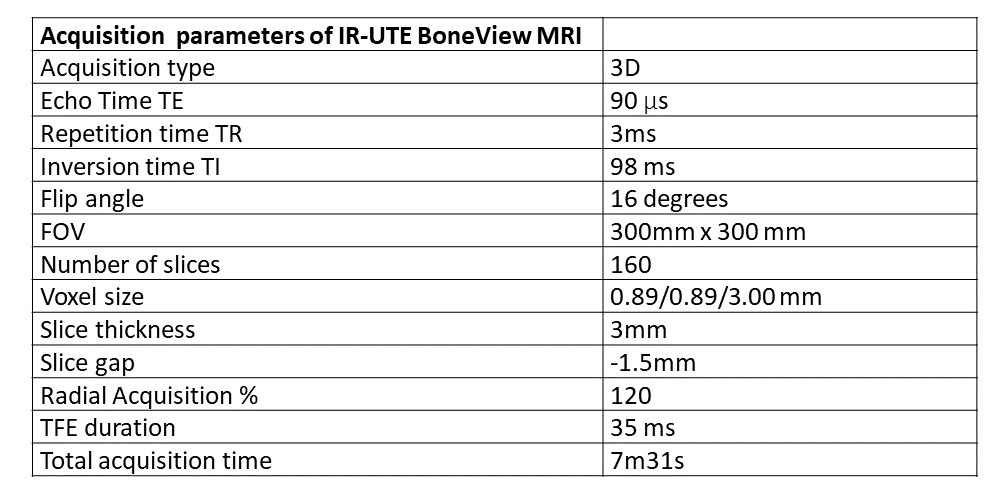
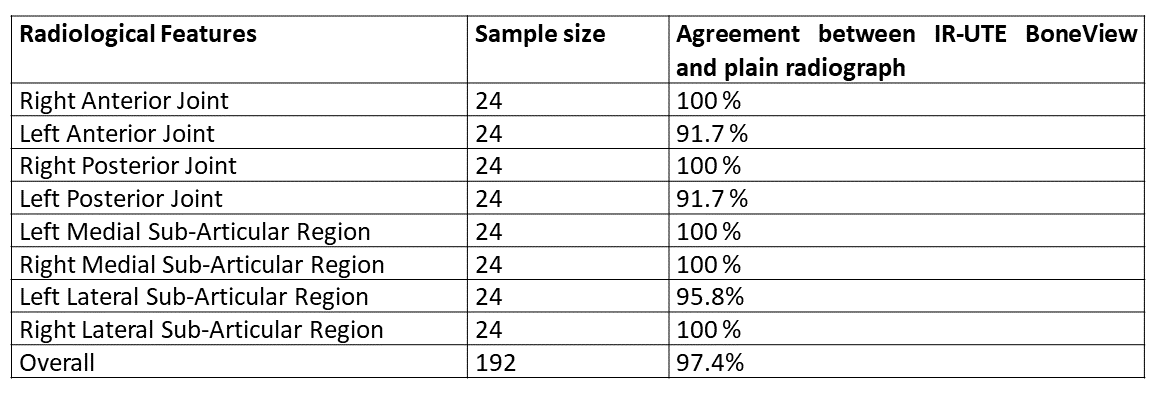
A total of 30 patients were selected for this study based on selection criteria, out of which 6 were excluded due to image artifacts. Thus, 24 patients were included for this study. 192 radiological features were evaluated by two radiologists for each X-Ray and IR-UTE BoneView technique i.e., a total of 384 radiological features evaluated. Table 1 shows the parameters used for acquiring IR-UTE BoneView images. Table 2 shows that Radiologist 1 and Radiologist 2 assessments matched 100% with an Intraclass Correlation Coefficient (ICC) score of 1. Table 3 shows that there is 97.7% agreement in the findings between X-Ray and IR-UTE BoneView images across all the evaluated radiological features. As shown in Figure 1, the normal SIJ is clearly visible in IR-UTE BoneView images and is comparable with the plain radiograph.Conclusion and Discussion
We have demonstrated that IR-UTE BoneView images depict sufficient SIJ structural radiological features in non-pathological cases in comparison with plain radiographs. The inter reader agreement of 100% shows that the conclusion is reader independent. Additionally, we have quantitatively demonstrated that there is 97.4% agreement between the findings in plain radiographs and IR-UTE BoneView images. The minor differences in the findings between the two could be attributed to positioning errors in radiographs. While not the goal of this study; it was also observed that there is an agreement (inter-reader as well as inter modality) in detection of minor degenerative changes in non-pathological cases. This suggests that there is a possibility to detect bony lesions with IR-UTE BoneView in pathological cases as well. Although, this needs further investigation in a statistically significant number of pathological SIJ cases with varying degrees of severity. These findings suggest that IR-UTE BoneView together with standard MR protocol for imaging SIJ has the potential to be used for exclusion of patients with pathological SIJ without needing X-ray images. The benefit of this finding could have a great impact on efficient utilization of hospital resources including the staff as well as improved patient outcome.Acknowledgements
No acknowledgement found.References
[1] A. Kiapour, A. Joukar, H. Elgafy, D. U. Erbulut, A. K. Agarwal, and V. K. Goel, “Biomechanics of the Sacroiliac Joint: Anatomy, Function, Biomechanics, Sexual Dimorphism, and Causes of Pain,” Int. J. Spine Surg., vol. 14, no. s1, pp. S3–S13, Feb. 2020, doi: 10.14444/6077.
[2] P. Buchanan et al., “Successful Diagnosis of Sacroiliac Joint Dysfunction,” J. Pain Res., vol. Volume 14, pp. 3135–3143, Oct. 2021, doi: 10.2147/JPR.S327351.
[3] S. P. Cohen, Y. Chen, and N. J. Neufeld, “Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis and treatment,” Expert Rev. Neurother., vol. 13, no. 1, pp. 99–116, Jan. 2013, doi: 10.1586/ern.12.148.
[4] M. Rudwaleit et al., “The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection,” Ann. Rheum. Dis., vol. 68, no. 6, pp. 777–783, Jun. 2009, doi: 10.1136/ard.2009.108233.
[5] I. Möller et al., “The 2017 EULAR standardised procedures for ultrasound imaging in rheumatology,” Ann. Rheum. Dis., vol. 76, no. 12, pp. 1974–1979, Dec. 2017, doi: 10.1136/annrheumdis-2017-211585.
[6] M. Yoneyama, I. Ball, M. Azuma, T. Hirai, and M. Van Cauteren, “3D broadband IR-prepared UTE bone imaging for assessment of ossification of the posterior longitudinal ligament (OPLL) in the cervical spine [abstr],” in Proceedings of the 27th Meeting of the International Society for Magnetic Resonance in Medicine. Berkeley: International Society for Magnetic Resonance in Medicine, 2019. Accessed: Nov. 02, 2023. [Online]. Available: https://archive.ismrm.org/2019/2873.html
Figures