0632
High-Resolution Oblique Coronal MRI with Optimal Flexed-Knee Angle for Anterior Cruciate Ligament Tear Diagnosis1Department of Radiology, The Third Xiangya Hospital, Central South University, Changsha, China, 2Clinical & Technical Support, Philips Healthcare, Shanghai, China
Synopsis
Keywords: Whole Joint, MSK
Motivation: Anterior cruciate ligament (ACL) injuries are prevalent in the realm of knee injuries. Conventional MRI methodologies employed for diagnosing ACL tears exhibit low accuracy.
Goal(s): Evaluate the diagnostic efficacy of high-resolution coronal MRI performed at an optimal flexion angle specifically for ACL tears.
Approach: Healthy volunteers and patients are scanned to find the optimal flexion angle and compare the image quality with traditional extended-knee positioning approach.
Results: The implementation of high-resolution coronal imaging at the ideal flexion angle (30 degrees) has the potential to enhance ACL visualization and improve diagnostic accuracy when compared with conventional techniques.
Impact: The utilization of high-resolution coronal imaging at the optimal flexion angle (30 degrees) demonstrated a substantial enhancement in the visualization of the anterior cruciate ligament (ACL), resulting in a notable improvement in diagnostic accuracy as compared to conventional techniques.
Introduction
The anterior cruciate ligament (ACL) serves a crucial role in maintaining the anterior stability of the knee joint. Rupture of the ACL can significantly impact knee joint stability. While MRI offers a convenient and noninvasive approach for evaluating ACL tears, the diagnostic accuracy can be as low as 57.1% for partial ACL tears [1].Previous studies have predominantly employed the extended-knee position for knee joint scans, which may not be optimal for displaying the ACL [2-3].
The objective of this study was to identify the optimal flexion angle that provides optimal visualization of the ACL. Furthermore, the study aimed to assess the imaging improvement and diagnostic performance of high-resolution coronal imaging with optimal flexion angle in comparison to conventional extended-knee sagittal imaging techniques.
Methods
Optimal flexion angle measurementA cohort of 50 healthy volunteers was recruited to investigate the optimal flexion angle. All participants underwent MRI scans using a 3.0T MRI scanner (Ingenia, Philips Healthcare, Best, the Netherlands) equipped with a 4-channel FLEX M coil. A specialized knee joint dynamic scanning device [4] was employed. The knee joint angles were precisely adjusted using the straps on the traction device (Figure 1A). Detailed imaging parameters could be found in Table 1.
Patient scanning
A cohort of 92 patients with trauma-related injury were scanned on the same MRI scanner as for the volunteers but with an 8-channel knee joint coil. Initially, conventional knee scans were performed in an extended position (control group). High-resolution coronal scans then were performed based on the previously determined optimal flexion angle (experimental group). Figure 2 illustrates the positioning for coronal scanning. Detailed imaging parameters are shown in Table 1. All patients underwent arthroscopy later on.
Image Analysis
Two physicians independently reviewed the images. Any disagreements were resolved by a senior physician.
The imaging quality of the ACL in the experimental and control groups was rated on a 5-point scale (Table 2).Diagnostic outcomes were categorized as either an ACL tear (both complete and partial tears) or not. Arthroscopy is considered the “gold standard” for joint diagnosis.
Statistical analysis was performed with SPSS version 22.0 (IBM Corp, IL, USA). Ordinal data comparison between the groups was performed with the Mann–Whitney U test. We derived diagnostic performance values with the receiver operating characteristic (ROC) curve, and the DeLong test ascertained the statistical variance between the area under curve (AUC) of the 2 groups. Results with a P value < 0.05 were considered statistically significant.
Results
The ideal flexion angle for 50 volunteers was 19°-39°, averaging (30.3° ± 4.97°). In MRI oblique coronal scans with optimal flexion, the ACL had a nearly straight course with moderate tension, and both anterior-medial and posterior-lateral bundles were clearer in the same plane than that in the conventional extended-knee position (Figure 3).The entire ACL was visualized on ≥3 layers in 96.7% (89/92) of images in the experimental group compared with 12.0% (11/92), the difference was significant (Z=11.266, P<0.001) (Table 2).
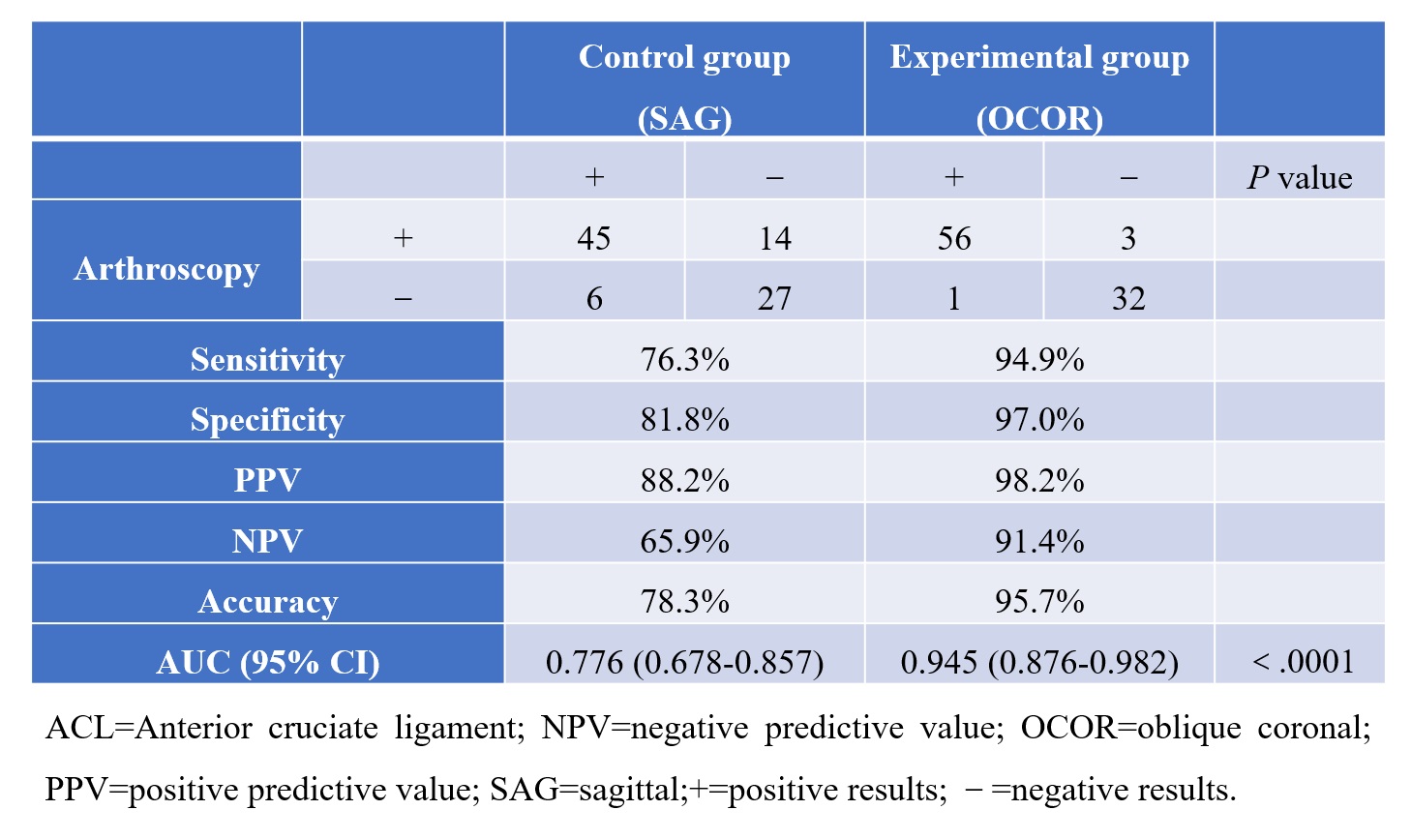
With arthroscopy as a benchmark, the experiment group has a better diagnostic value compared with the control group, regarding the sensitivity (94.9% v.s. 76.3%), specificity (97.0% v.s. 81.8%), PPV (98.2% v.s. 88.2%), NPV (91.4% v.s. 65.9%) and accuracy (95.7% v.s. 78.3%).
The ROC curve revealed higher AUC for the experimental group (0.945, 95% CI: 0.876-0.982) than for the control group (0.776, 95% CI: 0.678-0.857) (P <0.0001) (Table 3).
Discussion
The 30-degree knee flexion angle made the anatomical path of the 2 bundles of ACL straight and parallel. The 30º angle also was reasonably comfortable for trauma patients.In this study, the imaging of the ACL in its entirety was better in the experimental group than in the control group. Such results align with earlier research findings. Nenezić and Kocijancic [5] reported that oblique sagittal imaging improved detection of ACL tear from 33% to 87%; Przeworski et al. [6] affirmed the value of oblique planes with 3D sequences in their MRI research on dogs; and Ng et al. [7] demonstrated the efficacy of oblique imaging in visualizing the ACL, with sensitivities up to 71%. However, most of these studies used extended-knee positioning. In the present study, the ROC curve analysis revealed superior optimal knee flexion angle imaging in the experimental group with an AUC of 0.945 compared with 0.776 for the control group.
Conclusion
Oblique coronal imaging performed at an optimized flexed-knee angle of 30° provides superior visualization of the complete ACL and demonstrates enhanced diagnostic accuracy for the detection of ACL tears in comparison to conventional sagittal imaging performed with the knee in an extended position.Acknowledgements
No acknowledgement found.References
[1] Moore SL. Imaging the anterior cruciate ligament. Orthop Clin North Am 2002;33(4):663-674.
[2] Taljanovic MS, Graham AR, Benjamin JB, et al. Bone marrow edema pattern in advanced hip osteoarthritis: quantitative assessment with magnetic resonance imaging and correlation with clinical examination, radiographic findings, and histopathology. Skeletal Radiol 2008;37(5):423-431.
[3] Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 2006;14(3):204-213.
[4] Chinese National Invention Patent, No. ZL201610430464.5
[5] Nenezic D, Kocijancic I. The value of the sagittal-oblique MRI technique for injuries of the anterior cruciate ligament in the knee. Radiol Oncol 2013;47(1):19-25.
[6] Przeworski A, Adamiak Z, Nowicki M, Mieszkowska M, Tobolska A, Głodek J. Assessment of the Usefulness of Image Reconstruction in the Oblique and Double-oblique Sagittal Planes for Magnetic Resonance Imaging of the Canine Cranial Cruciate Ligament. J Vet Res 2021;65(2):209-216.
[7] Ng AW, Griffith JF, Law KY, et al. Oblique axial MR imaging of the normal anterior cruciate ligament bundles. Skeletal Radiol 2011;40(12):1587-1594.
Figures
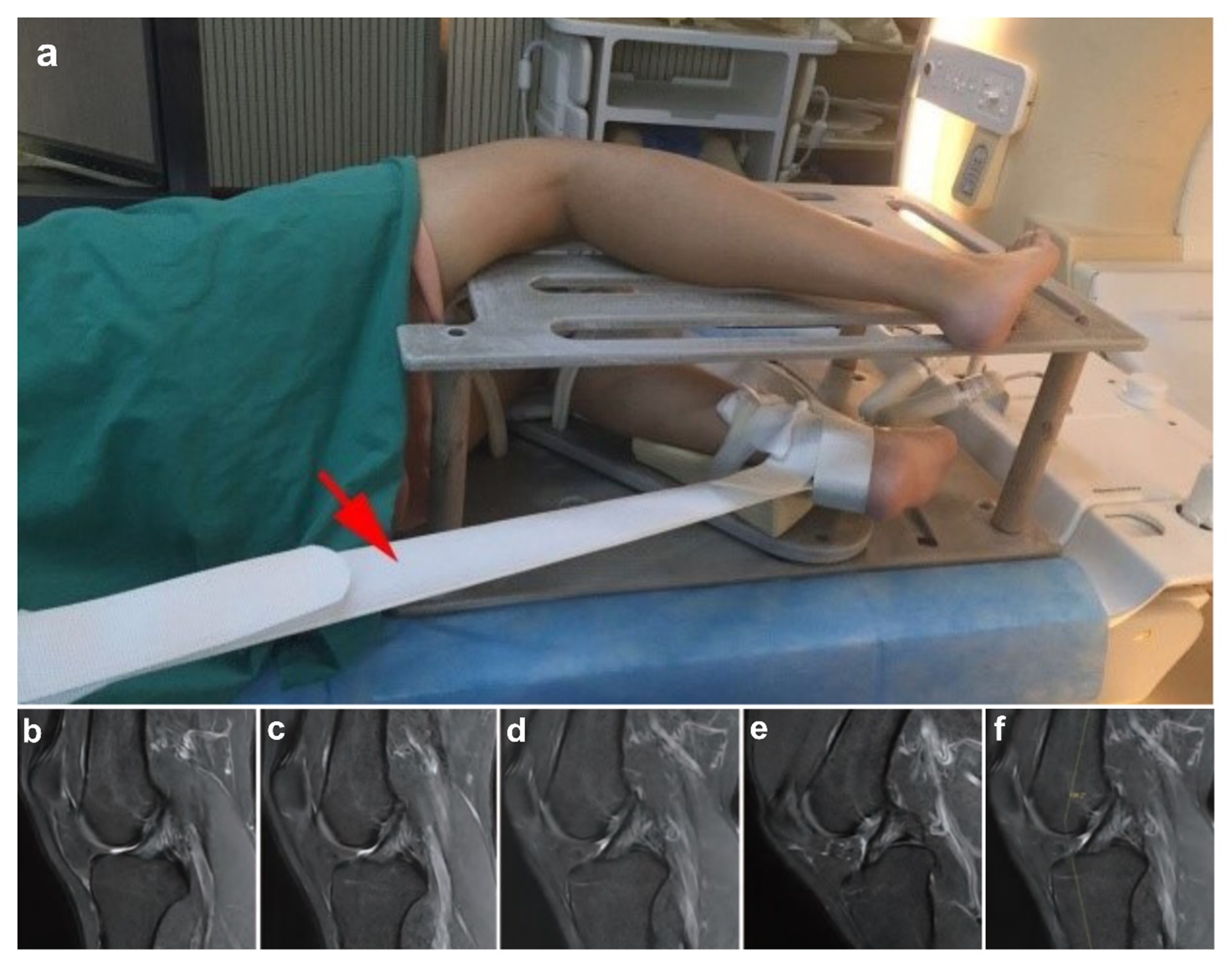
Figure 1. Knee joint dynamic scanning positioning and measurement of the optimal flexion angle. (a) Volunteer in the lateral position, with knee joint angle adjusted using the traction straps on the self-made knee joint dynamic imaging assistive device (red arrow). (b-e) Sagittal scans using the T2WI-TSE-SPAIR fast dynamic sequence. (f) Measurement of the flexion angle at the level where the ACL runs nearly straight and is moderately tense (i.e., the individualized optimal flexion angle).
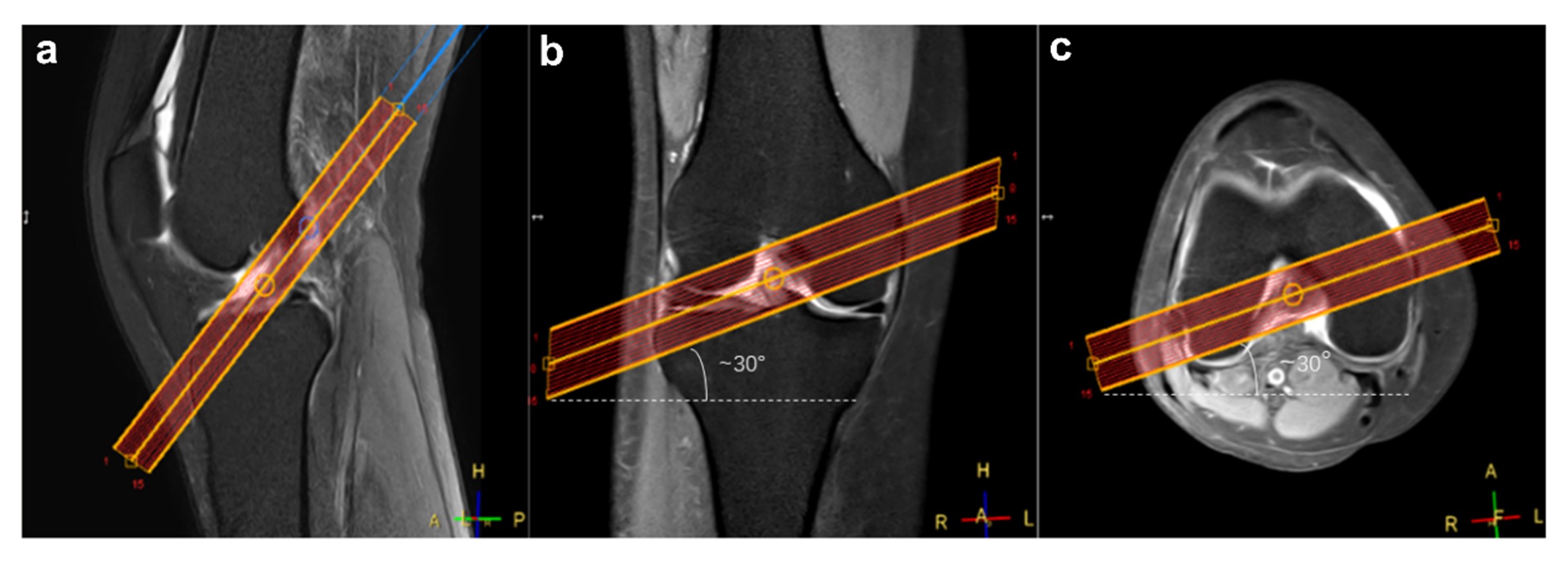
Figure 2. Scanning positioning in the coronal plane. (a) Sagittal scanning orientation parallel to the course of the ACL. (b) Coronal plane aligned at approximately 30° to the joint surface, with a higher inner aspect and a lower outer aspect. (c) Transverse plane set at an angle of approximately 30° to the line connecting the inner and outer edges of the femoral condyles, also with a higher inner aspect and a lower outer aspect. ACL= anterior cruciate ligament.
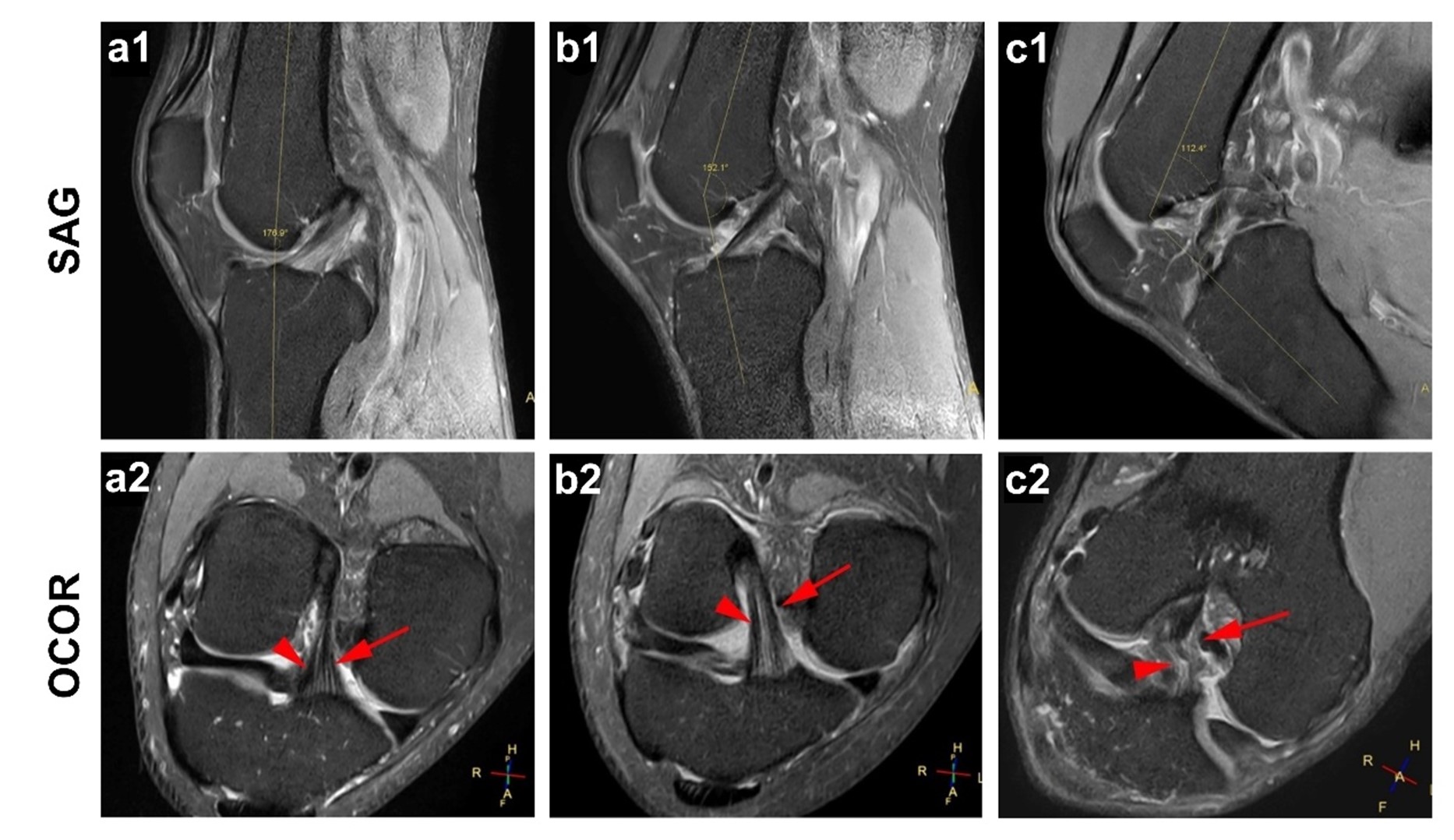
Figure 3. ACL visualization at various knee flexion angles: (a1) Extended knee: sagittal demonstrating ACL with higher tension and slight backward twist. (a2) Oblique Coronal: ACL bundles appear crossed due to twisting. (b1) ~28° knee flexion: sagittal depicting straight ACL with moderate tension. (b2) Oblique Coronal: parallel and in-plane ACL bundles. (c1) ~68° knee flexion: sagittal revealing low-tensioned and forward-twisted ACL. (c2) Oblique Coronal: twisted ACL bundles, reducing visibility. Red arrows indicate anterior-medial and posterior-lateral bundles of ACL.
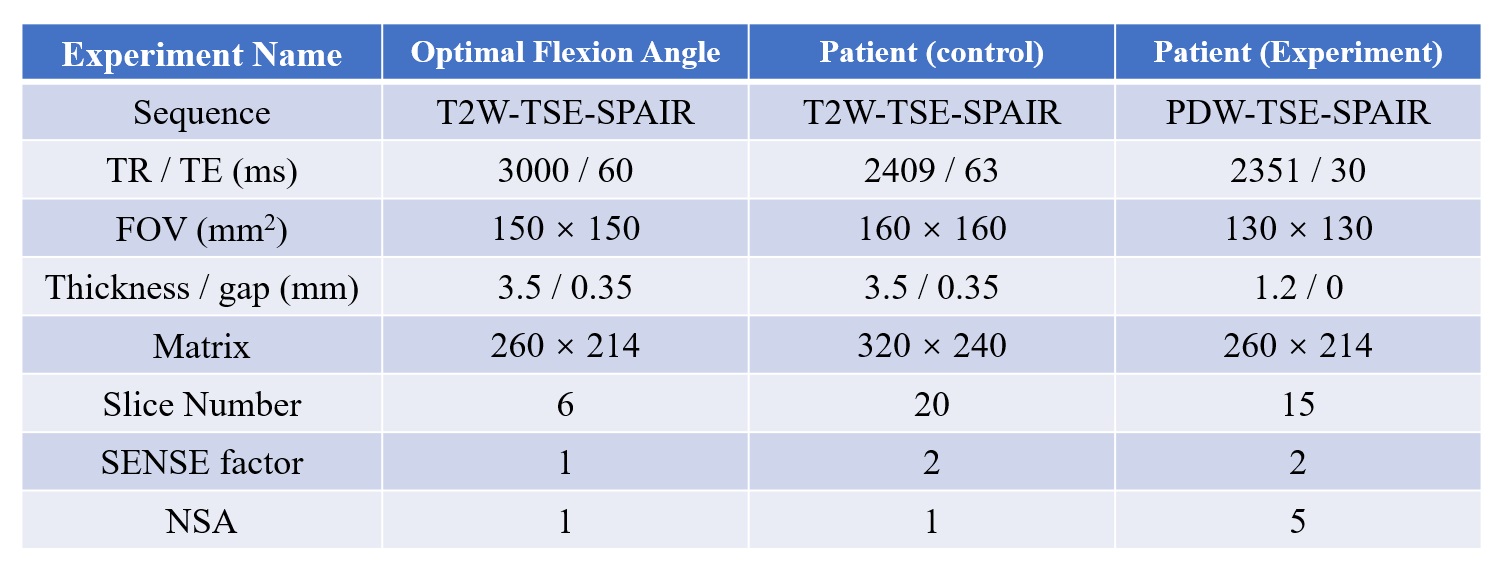
Table 1. Imaging parameters
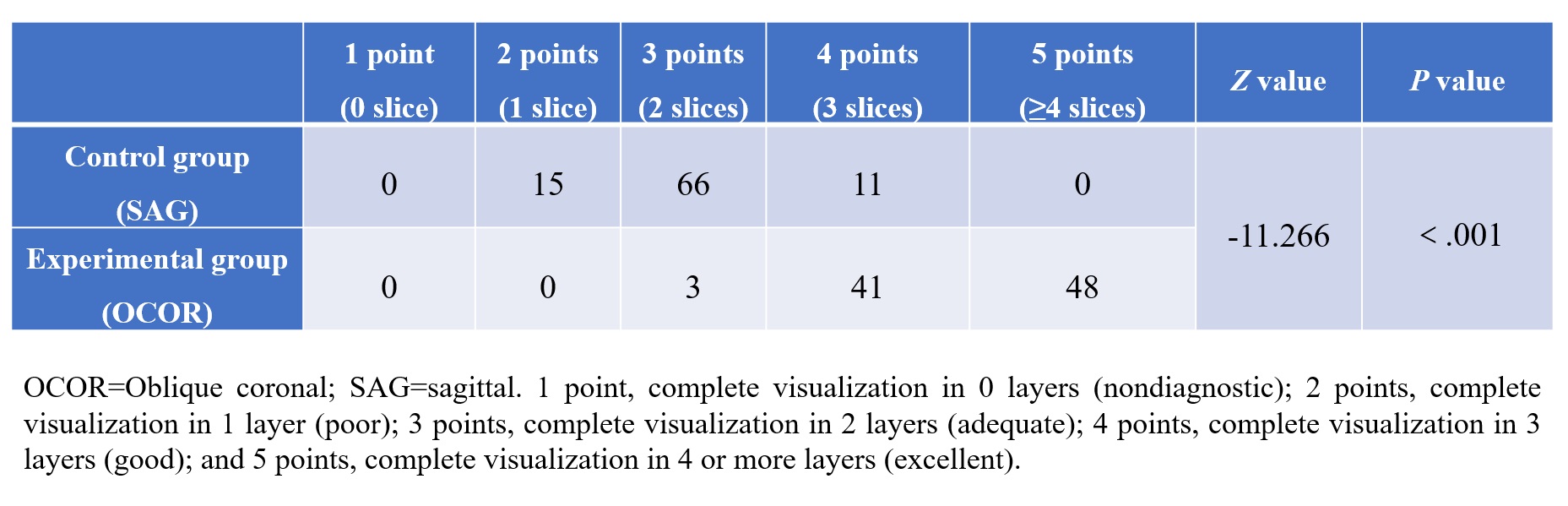
Table 2. Frequency counts for each level of images in the experimental and control groups