0626
Sub-Second GRASP-LLR DCE: Locally Low-Rank Subspace Constraint aided by Deep Learning1Radiology, Weill Cornell Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University, New York, NY, United States
Synopsis
Keywords: Quantitative Imaging, Breast, DCE
Motivation: We hope to advance the assessment of breast dynamic contrast-enhanced MRI (DCE-MRI) by enhancing image quality, temporal resolution, and temporal fidelity.
Goal(s): Propose a new radial GRASP reconstruction pipeline for DCE-MRI, which enables reliable spatially localized dynamics at a sub-second temporal resolution.
Approach: Presenting globally and locally low-rank reconstruction approaches for GRASP DCE-MRI aided by Residual Network (ResNet) architecture.
Results: Our results suggest that GRASP-LLR offers not only enhanced tumor lesion delineation with reduced background noise but also good separation between healthy, benign, and malignant cases.
Impact: We propose a new radial reconstruction pipeline for DCE-MRI which leverages a locally low-rank (LLR) subspace model in combination with deep learning approach, resulting in reliable spatially localized dynamics at a sub-second temporal resolution.
Introduction
Recently, it has been shown that dynamic-contrast-enhanced (DCE)-MRI can be improved by combining globally low‐rank (GLR) modeling with sparsity constraints (1-3). While GLR model has been shown to be effective in representing global contrast change, it is expected to be less effective in representing spatially localized signal dynamics while maintaining high temporal fidelity. Here, we propose a new radial reconstruction pipeline, which leverages a locally low-rank (LLR) subspace model (3,4) to represent spatially localized dynamics based on either block (LLR-Block) or tissue segment-based (LLR-Seg) reconstruction. By learning a temporal basis for each block/segment, a subspace representation is generated by enforcing an explicit LLR subspace constraint. A Residual Network was designed with two main goals in mind: a) to generate GRASP-LLR-Seg with sub-second temporal resolution (0.8 sec) while maintaining high temporal fidelity and, b) to overcome undersampling penalty.Methods
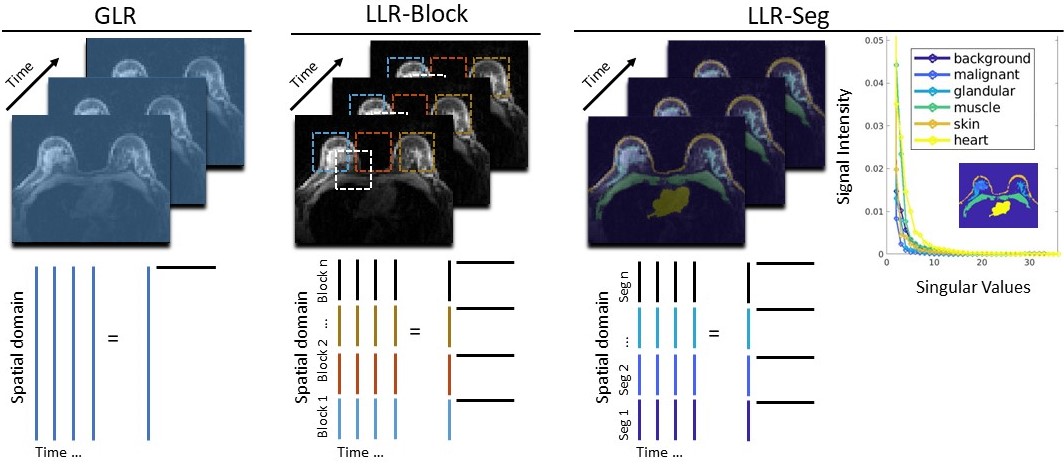
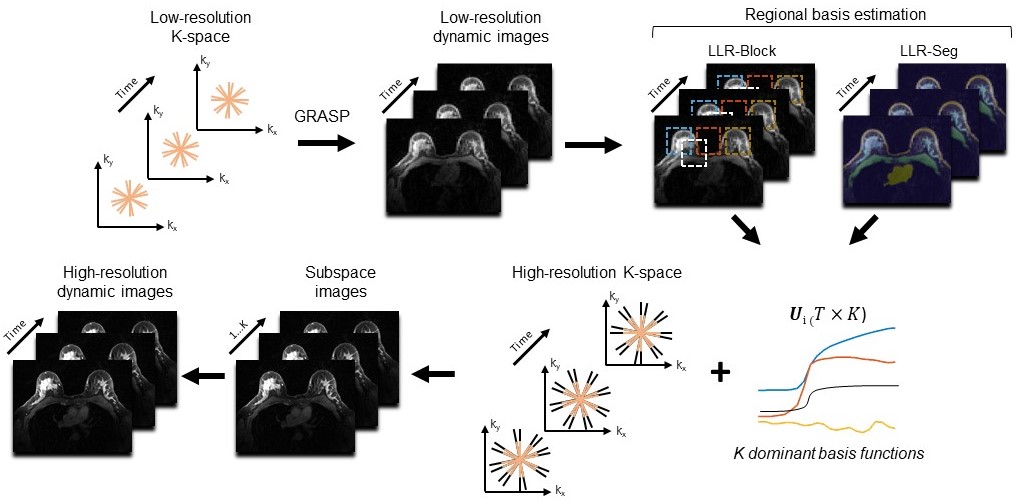
Data acquisition: Fifty-seven breast cancer patients were scanned on a 3T scanner (Siemens,Germany). Data included radial acquisition (GRASP) with a golden-angle,192 slices with partial-Fourier,288 radial-views (~0.4 sec each) and 1.0×1.0×1.1mm3 resolution.Image reconstruction: The GLR model enforces that an image-series with a low-rank condition can be represented as a product of two matrices containing relatively few basis functions and their corresponding coefficients (Fig.1,left). Alternatively, with LLR approach, the image can be divided either into blocks (Fig.1,middle) or tissue-segments (Fig.1,right) where each region can be decomposed into a product of two matrices containing spatial and temporal basis functions. Following this approach, singular values of each tissue-segment (Fig.1,right) show a unique curve shape which can be represented by K dominant basis components. Our proposed reconstruction (Fig.2) pipeline is the following: Step-1) reconstruct GRASP low-resolution (\(L \times L)\) image-series (\(M_{L}\)) by solving the optimization problem: \(\underset{M_{L}}{argmin}{{\frac{1}{2}\left\| y_{L}\left. \ - EM_{L} \right\| \right.\ }_{2}^{2} + \lambda\left\| \left. \ SM_{L} \right\| \right.\ _{1}}\) where \(y_{L}\ \) is the k‐space data shifted to a Cartesian grid (5), which includes the corresponding weighting (\(w_{L}\)) to compensating for the varying sampling density. \(E = \sqrt{w_{L}}\ \Phi F\ C_{L}\ \) is the encoding operator incorporating coil sensitivities (\(C_{L}\)), Fourier transform (\(F\)) and undersampling operator(\(\Phi)\). \(S\) is the sparsifying transform along the temporal dimension with \(\lambda\) regularizer. Step-2) LLR basis functions are estimated from low-resolution image-series using principal-component-analysis (PCA) for \(n\) number blocks or tissue-segments, representing the image (\(M_{L} = \sum_{i = 1}^{n}{U_{i}V_{ki}}\)) where \(U_{i}\) is the temporal basis of the i-th region and \(V_{ki}\) represents the number of \(K\) associated coefficients. The number of \(K\) principal components (PC) for each block/segment was fixed to six. Step-3) A full‐resolution image‐series is compressed to a low‐dimensional subspace image-series. Step-4) Finally, the full-resolution time-series is reconstructed by multiplying the set of coefficients by the subspace image-series and solving the optimization problem: \(\underset{V_{k}}{argmin}{{\frac{1}{2}\left\| y\left. \ - E\sum_{i = 1}^{n}{U_{i}V_{ki}}\ \right\| \right.\ }_{2}^{2} + \lambda\left\| \left. \ S\sum_{i = 1}^{n}{U_{i}V_{ki}} \right\| \right.\ _{1}}\)
Network architecture and simulation: A 2D Residual Network (ResNet) was implemented in Pytorch and trained using the Adam optimizer. The network was trained in a supervised fashion using a L2-norm loss function between undersampled images and fully-sampled references. The training included 20 datasets and another 2 datasets for validation, generated by a breast Digital Reference Object (DRO) simulation platform (6) that creates realistic morphology and contrast kinetic lesion and tissues. Once trained, ResNet was tested on undersampled low-resolution real images which was then plugged into our reconstruction pipeline (Fig.2) for estimation of the basis (Step-2).
Results and Discussion
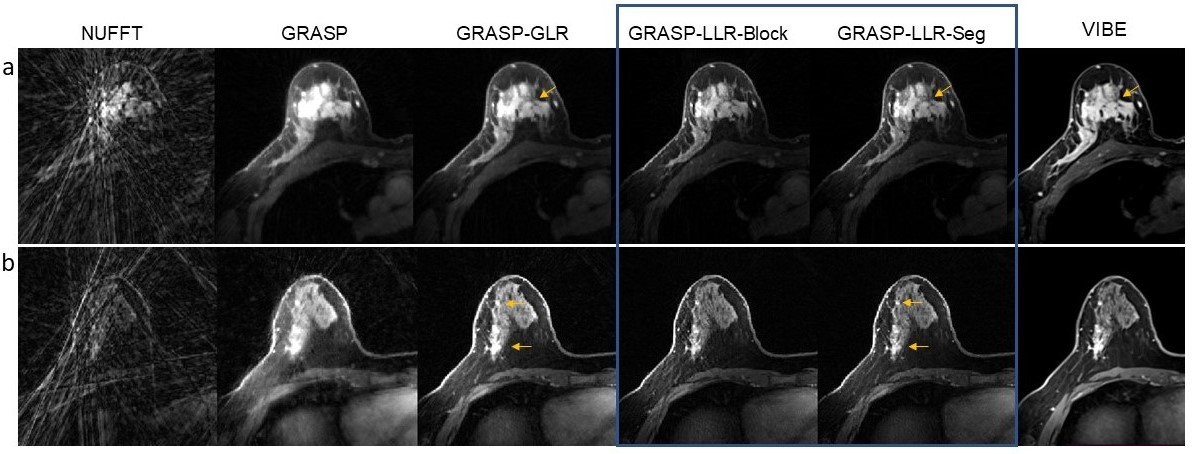
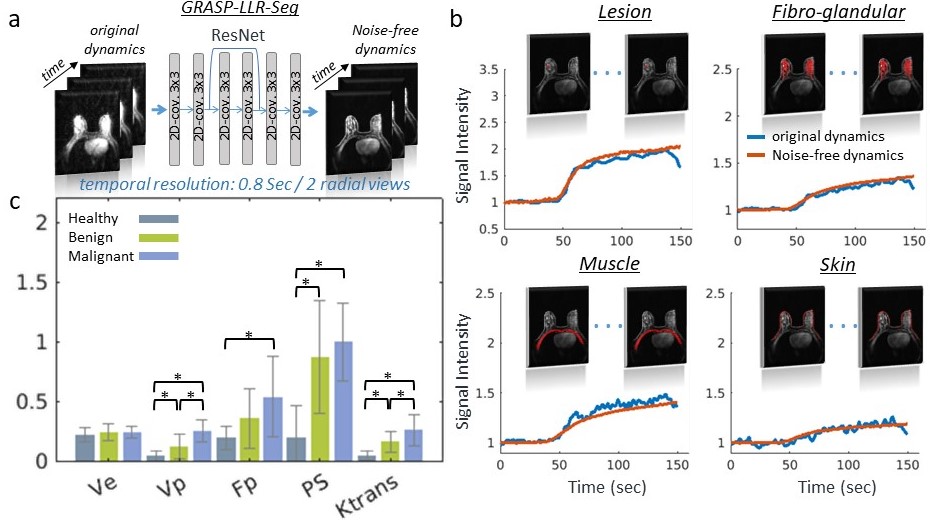
GRASP-LLR reconstruction showed enhanced conspicuity of the lesions with reduced background noise (Fig.3). This improvement by GRASP-LLR-Seg stems from the fact that each tissue and lesion is represented by a unique set of PCs for each segment. Inspired by these results, highly undersampled GRASP-LLR-Seg low-resolution image-series with sub-second temporal resolution (0.8 sec) was then implemented using ResNet (Fig. 4a), yielding reliable noise-free images while faithfully sustaining DCE temporal fidelity confirmed for each tissue individually (Fig.4b). To further validate that sub-second DCE can provide adequate temporal information, pharmacokinetic model (PKM) analysis was performed (Fig.4c) using the two-compartment exchange model across three distinct groups: 14 malignant, 21 benign and 21 normal-appearing fibroglandular tissues (sampled from contralateral healthy breast). The mean values of extracellular-extravascular space volume fraction (ve) showed no significant difference between healthy, benign and malignant cases, while the blood flow (Fp), permeability-surface-product (PS) and transfer rate constant (Ktrans), showed good separation between groups.Conclusion
GRASP-LLR reconstruction enables to utilize spatially localized dynamic patterns by using either block or segment-based reconstruction. Our results suggest that this approach offers not only improved image quality but also reliable DCE temporal information, even at sub-second temporal resolution.Acknowledgements
RSNA Research Seed Grant RSD1830, NIH R01CA160620, R01CA219964, UH3CA228699, and R01EB030549.References
- Feng L, Wen QT, Huang CC, Tong A, Liu F, Chandarana H. GRASP-Pro: imProving GRASP DCE-MRI through self-calibrating subspace-modeling and contrast phase automation. Magnetic Resonance in Medicine 2019.
- Otazo R, Candes E, Sodickson DK. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn Reson Med 2015;73(3):1125-1136. 3.
- Zhao B, Haldar JP, Christodoulou AG, Liang ZP. Image Reconstruction From Highly Undersampled (k, )-Space Data With Joint Partial Separability and Sparsity Constraints. Ieee T Med Imaging 2012;31(9):1809-1820.
- Kafali SG, Shih SF, Ruan D, Wu HH. Adaptive Locally Low Rank and Sparsity Constrained Reconstruction for Accelerated Dynamic Mri. I S Biomed Imaging 2020:930-934.
- Seiberlich N, Breuer F, Blaimer M, Jakob P, Griswold M. Self-calibrating GRAPPA operator gridding for radial and spiral trajectories. Magn Reson Med 2008;59(4):930-935.
- Bae J, Tan Z, Huang Z, Heacock L, Moy L, Knoll F, Kim S. Realistic Digital Reference Object (DRO) toolkit for quantitative breast Ultra-Fast Dynamic Contrast-Enhanced (UF-DCE) MRI. ISMRM proceedings 2023.
Figures