0614
Free-running motion-resolved 5D whole-heart anatomical MRI at 3T without contrast agent1Department of Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2CIBM Center for BioMedical Imaging, Lausanne, Switzerland
Synopsis
Keywords: Heart Failure, Heart, Cardiovascular; Acquisition Methods; Analysis/Processing
Motivation: Routine cardiac function assessment uses breath-held 2D cine imaging. Self-gated free-running sequences have recently been proposed to simplify the workflow. However, at 3T, GRE-based sequences require contrast agents to achieve blood-myocardium contrast.
Goal(s): This study introduced a contrast-agent-free acquisition for assessing cardiac anatomy and function at 3T.
Approach: Based on an interrupted free-running sequence, the proposed approach integrates T2 preparation and recovery modules to optimize blood-to-myocardium-contrast. A compressed-sensing-based reconstruction was used to generate 5D images of the whole heart.
Results: The framework was validated in 11 healthy volunteers, where it demonstrated slightly lower contrast but enabled effective left-ventricle segmentation and exhibited high reproducibility.
Impact: The proposed study introduces a contrast-agent-free method for a comprehensive 5D assessment of cardiac anatomy and function at 3T in a 5-minute acquisition. Demonstrating high agreement with the routine method, this approach holds promise for enhancing the overall patient management.
Introduction
Cardiac anatomy and function are routinely assessed using breath-held cine CMR as a reference method.1 Self-gated free-running sequences have recently been proposed to simplify such examinations.2 At 1.5T, 2D functional CMR is usually performed using balanced steady-state free precession (bSSFP)-based sequences. At 3T, gradient-recalled echo (GRE)-based sequences are preferred because they are less sensitive to the increased off-resonance effects caused by increased magnetic field inhomogeneities, and they have lower specific adsorption rate. However, 3D GRE results in poor contrast between the myocardium and the blood pool, leading to a need for contrast agents to improve image quality3, which complicates the acquisition workflow. In this study, we therefore proposed a contrast-agent-free alternative free-running acquisition for anatomy and function quantification at 3T by integrating regularly spaced T2 preparation (T2prep) modules.Methods
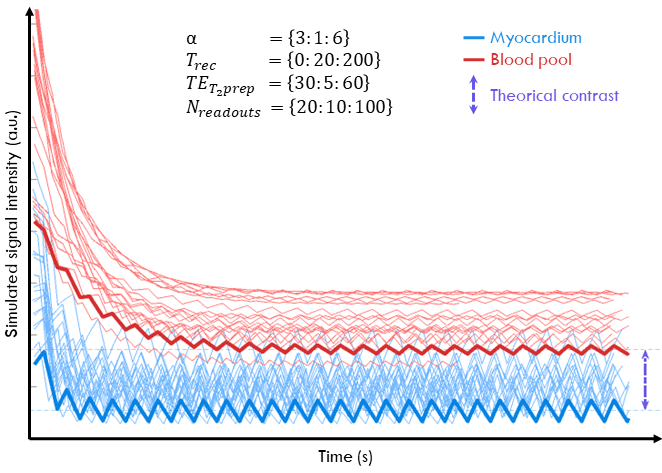
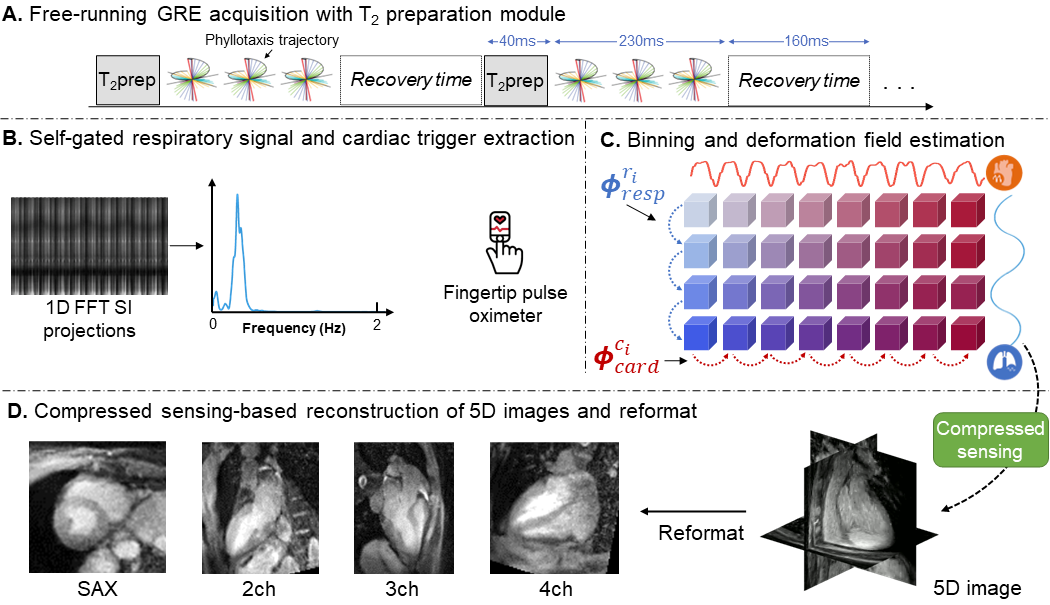
Acquisitions were performed in 11 healthy volunteers on a 3T clinical scanner (Magnetom PrismaFit, Siemens Healthineers, Erlangen, Germany) with a free-running GRE sequence (isotropic voxel size 2mm, field of view=220mm) using a 3D golden-angle spiral phyllotaxis radial trajectory.4 The sequence was interrupted with T2prep and recovery time modules to generate contrast between the blood and the myocardium (Fig.2A). Extended phase graph (EPG) simulations were run with a large array of sequence parameters combinations to optimize the theoretical signal intensity of the tissues throughout the acquisition. The optimal flip angle (α=4°), number of readouts per T2prep (Nreadouts=66), T2prep duration (TET2prep=40ms) and recovery time duration (Trec=160ms) were determined to maximize the absolute blood pool-to-myocardium contrast for an acquisition time of 5 minutes (Fig.1). A water-excitation RF pulse was numerically optimized using Optipulse5 for 3T systems (1ms pulse duration) to reduce lipid streaking artifacts.The first readout of each radial arrangement was in the superior-inferior (SI) orientation to capture physiological motion.6 The respiratory pattern was retrospectively extracted using principal component analysis of the 2D matrix of the Fourier‐transformed SI readouts. The cardiac pattern was recorded with a pulse oximeter since T2prep interference and low temporal sampling due to the recovery module did not allow direct extraction of the cardiac phase from SI readouts (Fig.2B); the pulse oximeter was used instead of ECG to avoid the effects of gradient switching on the ECG signal. These physiological patterns were then used for binning of the data into undersampled distinct motion states, which entered a compressed sensing-based reconstruction pipeline that included deformation fields to compensate for inter-bin motion (Fig.2C).7,8
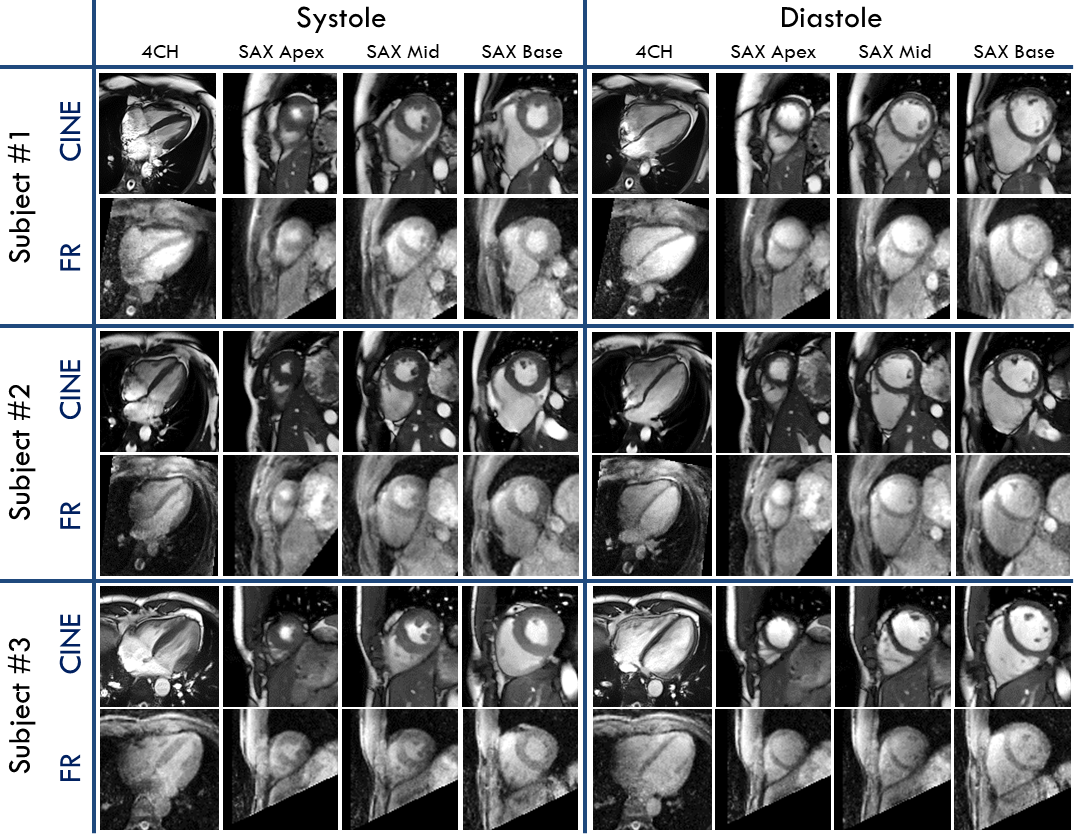
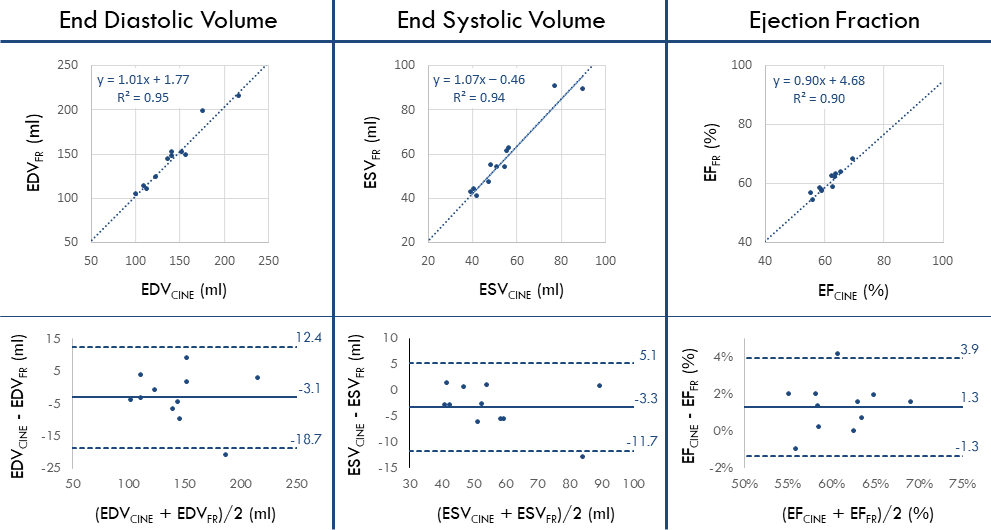
One of the primary advantages of the proposed isotropic method is that any 2D cine orientation can be retrospectively generated from the reconstructed 5D images (Fig.2D). In this study, the images were specifically reformatted into 4-chamber and short-axis orientations for comparison with routine 2D cine. The end-expiratory left-ventricular blood pool was segmented (cvi42, Circle Cardiovascular Imaging) at mid-diastole and end-systole on both the 2D routine cine and the corresponding reformatted free-running images to calculate the end-diastolic volume (EDV), end-systolic volume (ESV), and the ejection fraction (EF). The derived metrics were compared using intraclass correlation coefficient (ICC) with a 2, 1 formula9 and standard error of measurement (SEM). Furthermore, the agreement between both methods was assessed with correlation plots and Bland‐Altman analysis. Blood-to-myocardium contrast was calculated by determining $$$(S_{Blood} - S_{Myo}) / S_{Myo}$$$.
Results
While the proposed free-running images present a lower blood-to-myocardium contrast (0.67 ± 0.19) compared to that of 2D routine CINE (2.03 ± 0.91) images, it still provides sufficient contrast to enable straightforward left ventricle segmentation (Fig.3). The Bland-Altman plots revealed a slight underestimation of both EDV and ESV values by the proposed method. This consistent underestimation results in an ejection fraction (EF) bias of less than 2%. The proposed method exhibited high reproducibility compared to the clinical routine method, as evidenced by ICC (and SEM) values of 0.97 (5.62) for EDV, 0.97 (3.04) for ESV, and 0.95 (0.95) for EF.Discussion
The proposed framework enabled 3D cardiac functional assessment at 3T without the injection of a contrast agent or the risk of confounding inhomogeneity artifacts during a constant 5-minute time. Validation of the proposed 3D interrupted free-running acquisition demonstrated a high level of concordance in left ventricular function measurements when compared to the 2D routine cine method. Future work will focus on the validation of this framework in a larger cohort that includes patients, as well as cardiac self-gating. The acquisition parameter optimization using the EPG simulations will also be extended for higher image resolutions to enable the visualization of small cardiac structures and congenital heart disease.Acknowledgements
No acknowledgement found.References
- Kramer, C. M., Barkhausen, J., Bucciarelli-Ducci, C., Flamm, S. D., Kim, R. J., & Nagel, E. (2020). Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. Journal of Cardiovascular Magnetic Resonance, 22(1), 1-18.
- Di Sopra, L., Piccini, D., Coppo, S., Stuber, M., & Yerly, J. (2019). An automated approach to fully self‐gated free‐running cardiac and respiratory motion‐resolved 5D whole‐heart MRI. Magnetic resonance in medicine, 82(6), 2118-2132.
- Pang, J., Bhat, H., Sharif, B., Fan, Z., Thomson, L. E., LaBounty, T., ... & Li, D. (2014). Whole‐heart coronary MRA with 100% respiratory gating efficiency: self‐navigated three‐dimensional retrospective image‐based motion correction (TRIM). Magnetic resonance in medicine, 71(1), 67-74.
- Piccini, D., Littmann, A., Nielles‐Vallespin, S., & Zenge, M. O. (2011). Spiral phyllotaxis: the natural way to construct a 3D radial trajectory in MRI. Magnetic resonance in medicine, 66(4), 1049-1056.
- Sieber, X., Romanin, L., Bastiaansen, J., ... & Van Heeswijk, R. (2022). Efficient fat suppression in free-running whole-heart CMR using OptiPulse. Proceedings in International Society for Magnetic Resonance in Medicine.
- Coppo, S., Piccini, D., Bonanno, G., Chaptinel, J., Vincenti, G., Feliciano, H., ... & Stuber, M. (2015). Free‐running 4D whole‐heart self‐navigated golden angle MRI: initial results. Magnetic resonance in medicine, 74(5), 1306-1316.
- Roy, C.W., Milani, B., Yerly, J., ... & Stuber, M. (2023). Intra-bin correction and inter-bin compensation of respiratory motion in free-running 5D whole-heart MRI. Proceedings in International Society for Magnetic Resonance in Medicine.
- Yerly, J., Roy, C.W., Prsa, M., Milani, B., & Stuber, M. (2023). High on Sparsity: Inter-Bin Compensation of Cardiac Motion for Improved Assessment of Left Ventricular Function Using 5D whole-heart MRI. Proceedings in International Society for Magnetic Resonance in Medicine.
- Shrout, P. E., & Fleiss, J. L. (1979). Intraclass correlations: uses in assessing rater reliability. Psychological bulletin, 86(2), 420.
Figures