0609
In vivo STEAM and motion compensated spin echo diffusion tensor CMR in multiple cardiac phases: The effect of field strength1CMR Unit, The Royal Brompton Hospital, London, United Kingdom, 2National Heart and Lung Institute, Imperial College London, London, United Kingdom, 3Bioengineering, Imperial College London, London, United Kingdom
Synopsis
Keywords: Myocardium, Magnets (B0)
Motivation: Diffusion tensor cardiovascular magnetic resonance (DT-CMR) studies described in the literature have almost uniquely been performed at 3T while 1.5T scanners are more widely available.
Goal(s): To compare the performance and microstructural parameters available from stimulated echo (STEAM) and motion compensated spin echo (MCSE) DT-CMR sequences at 1.5T and 3T.
Approach: DT-CMR was performed in 20 healthy volunteers using both sequences at both field strengths at peak systole and end diastole.
Results: MCSE and STEAM sequences are effective at both 1.5T and 3T. STEAM benefits from the increased SNR available at 3T.
Impact: DT-CMR studies should consider making use of 1.5T hardware where access to 3T scanners is more difficult particularly where MCSE sequences are to be used with systolic triggering.
Background
Diffusion tensor cardiovascular magnetic resonance (DT-CMR) is emerging as a clinical research tool providing otherwise unattainable measures relating the myocardial structure and function on a microscopic scale[1]. While stimulated echo acquisition mode (STEAM) based methods provide robust, validated measures of the changes in microstructural arrangements over the cardiac cycle[2], motion compensated spin echo (MCSE) methods are more signal efficient and potentially facilitate free breathing studies[3].For both common DT-CMR sequences, the majority of studies have been performed at 3T, where the signal to noise ratio (SNR) is higher than at 1.5T. However, artefacts may be less severe, the capital outlay is less, and there are more 1.5T systems available.
Here, we compare the quality and identify any systematic differences in the microstructural parameters obtained from in-vivo DT-CMR between 1.5T and 3T for both STEAM and MCSE in multiple cardiac phases.
Methods
20 healthy subjects (mean age 26, range 20–63, 9/11 male/female) were imaged at 1.5T (Siemens MAGNETOM Sola, maximum gradient=45mT/m) and 3T (Siemens MAGNETOM Vida, maximum gradient=60mT/m) using similar receive coils and identical software including DT-CMR source code. Breath hold DT-CMR was performed in a single mid-ventricular short axis slice timed to acquire central k-space data at peak systole and during diastasis using both a monopolar STEAM sequence and second order MCSE sequence (using waveforms based on [4,5]). Slice position was matched between scanners.DT-CMR acquired six encoding directions, “b0”, EPI phase correction and parallel imaging reference data in each breath hold, requiring 18RR intervals/breath hold with TR=2RR intervals. Field of view=360 x 135mm2, no partial Fourier, SENSE x2, acquired resolution 2.8x2.8x8mm3 reconstructed at 1.4x1.4x8mm3 and fat saturation. The field of view was reduced in the phase encode direction by using in-plane slice selective RF pulses[6].
A reference b-value of 150smm-2 was used (2 averages) and for all MCSE sequences a main b-value of 450smm-2 (8 averages). For STEAM, the main b-value was 600smm-2 at 3T and reduced to 450smm-2 (8 averages in both cases) at 1.5T due to reduced SNR at 1.5T. For MCSE TE=62ms at 3T and TE=74ms at 1.5T. For STEAM TE=25ms at 3T and TE=26ms at 1.5T.
DT-CMR data were processed using an in-house MATLAB tool, excluding “b0” data and using a b-spline based registration. DT-CMR parameters compared between 1.5T and 3T sequences.
Results
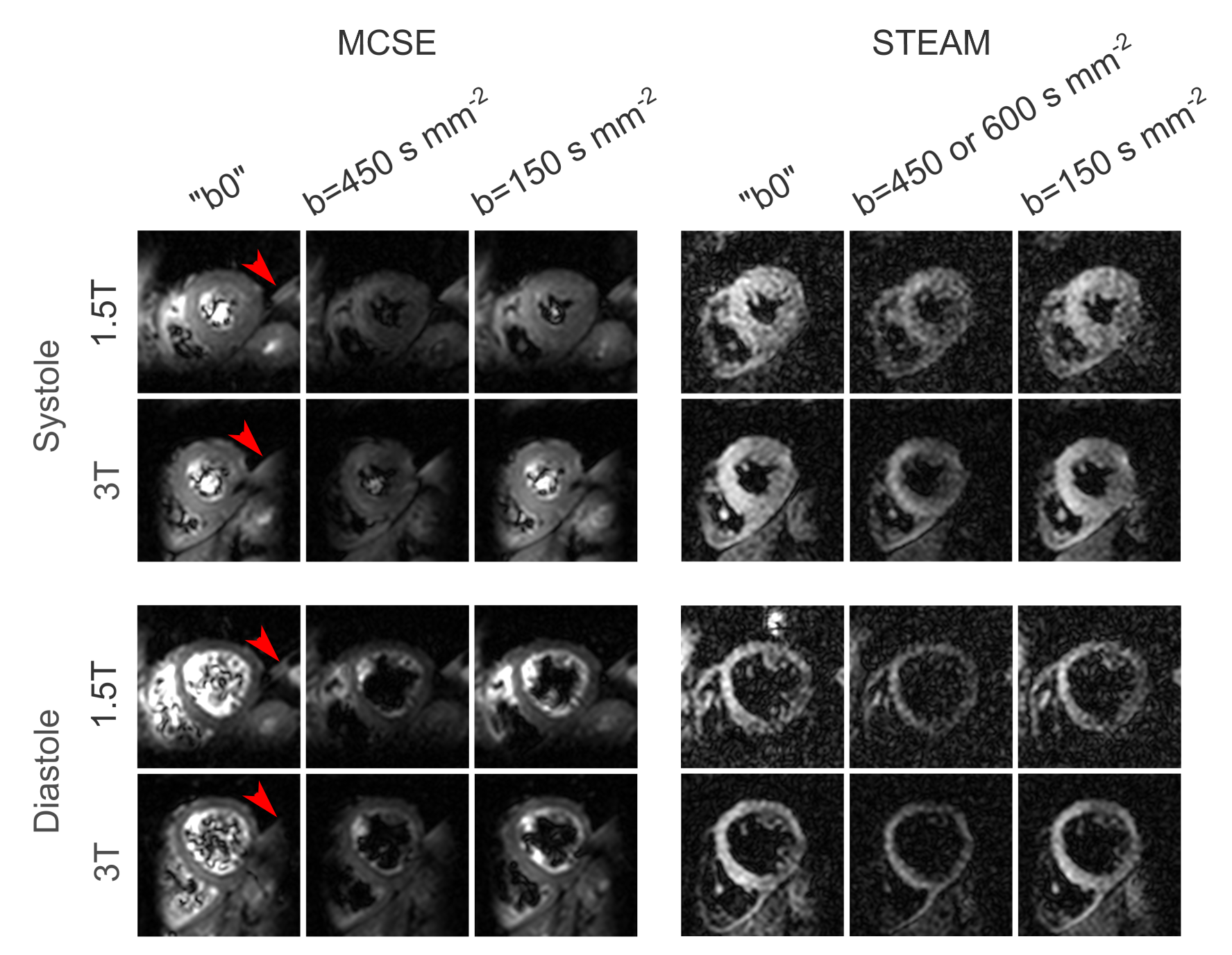
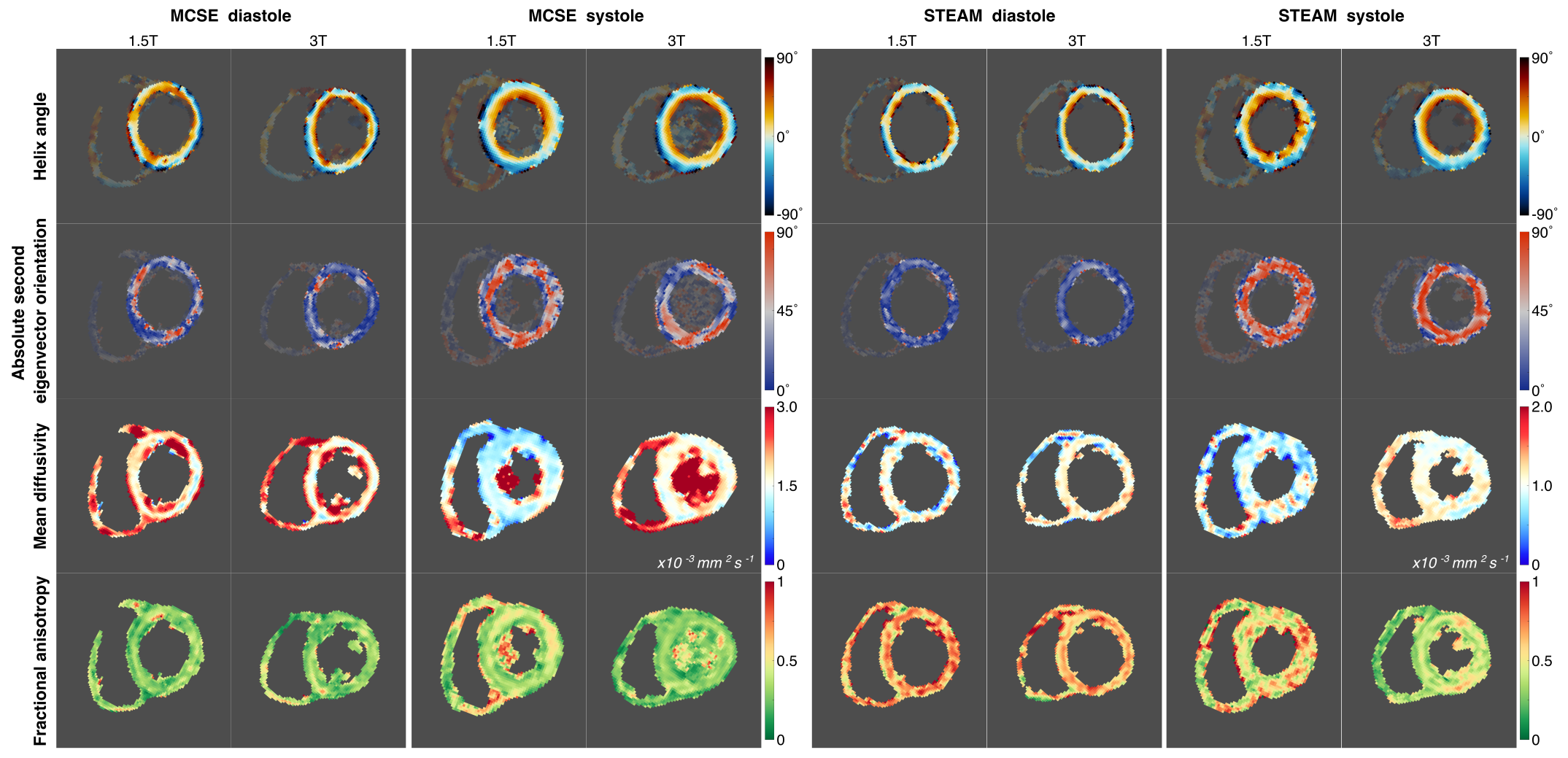
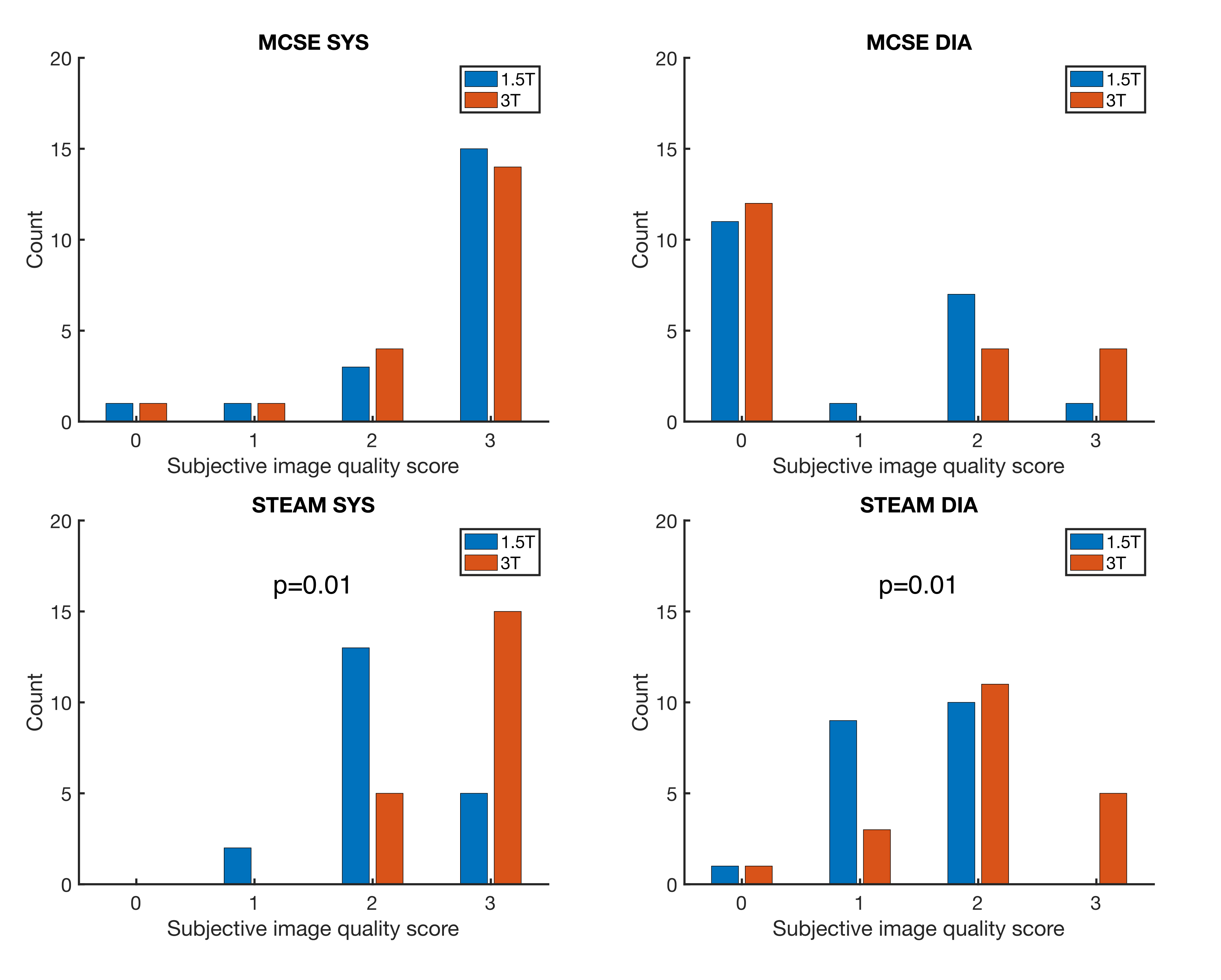
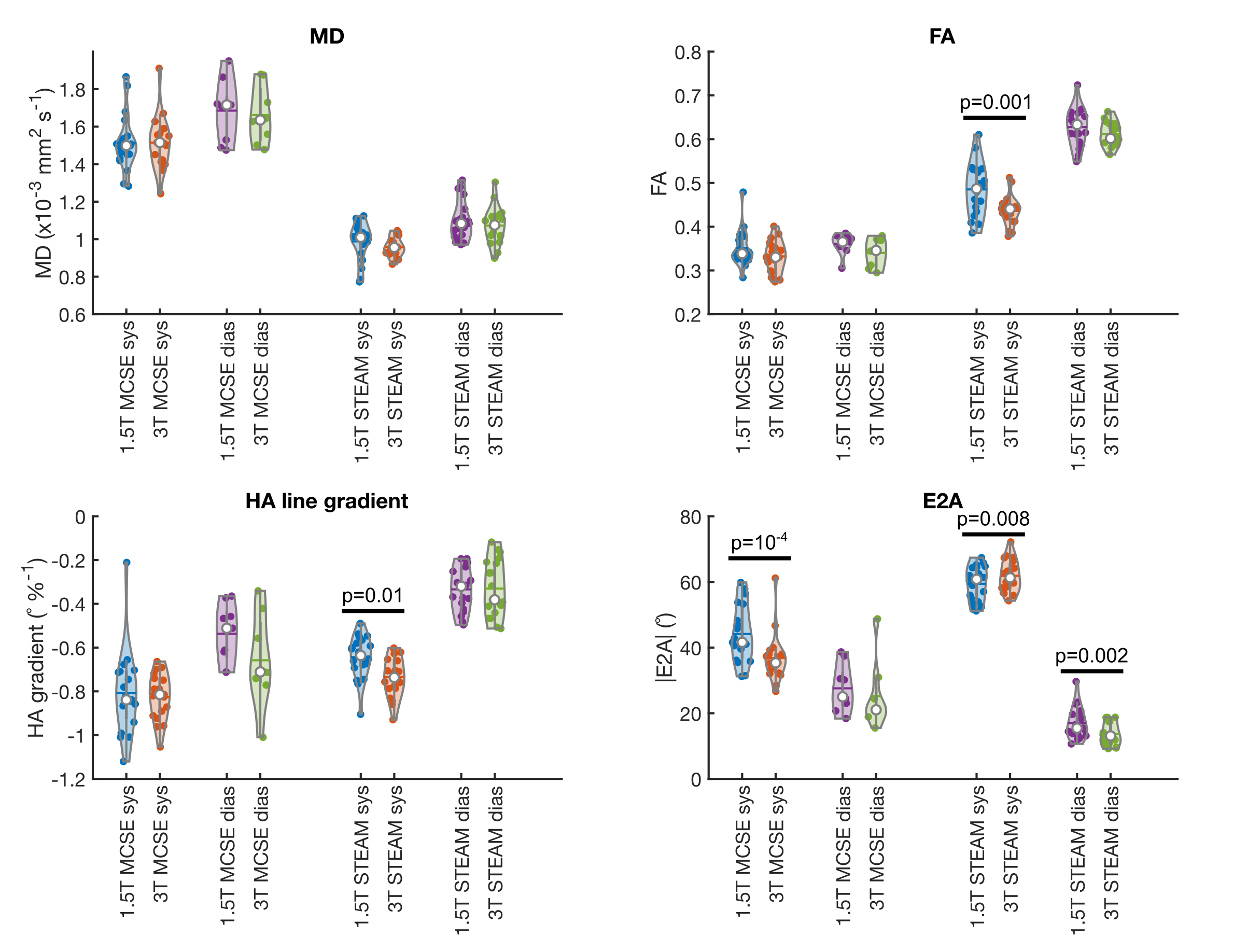
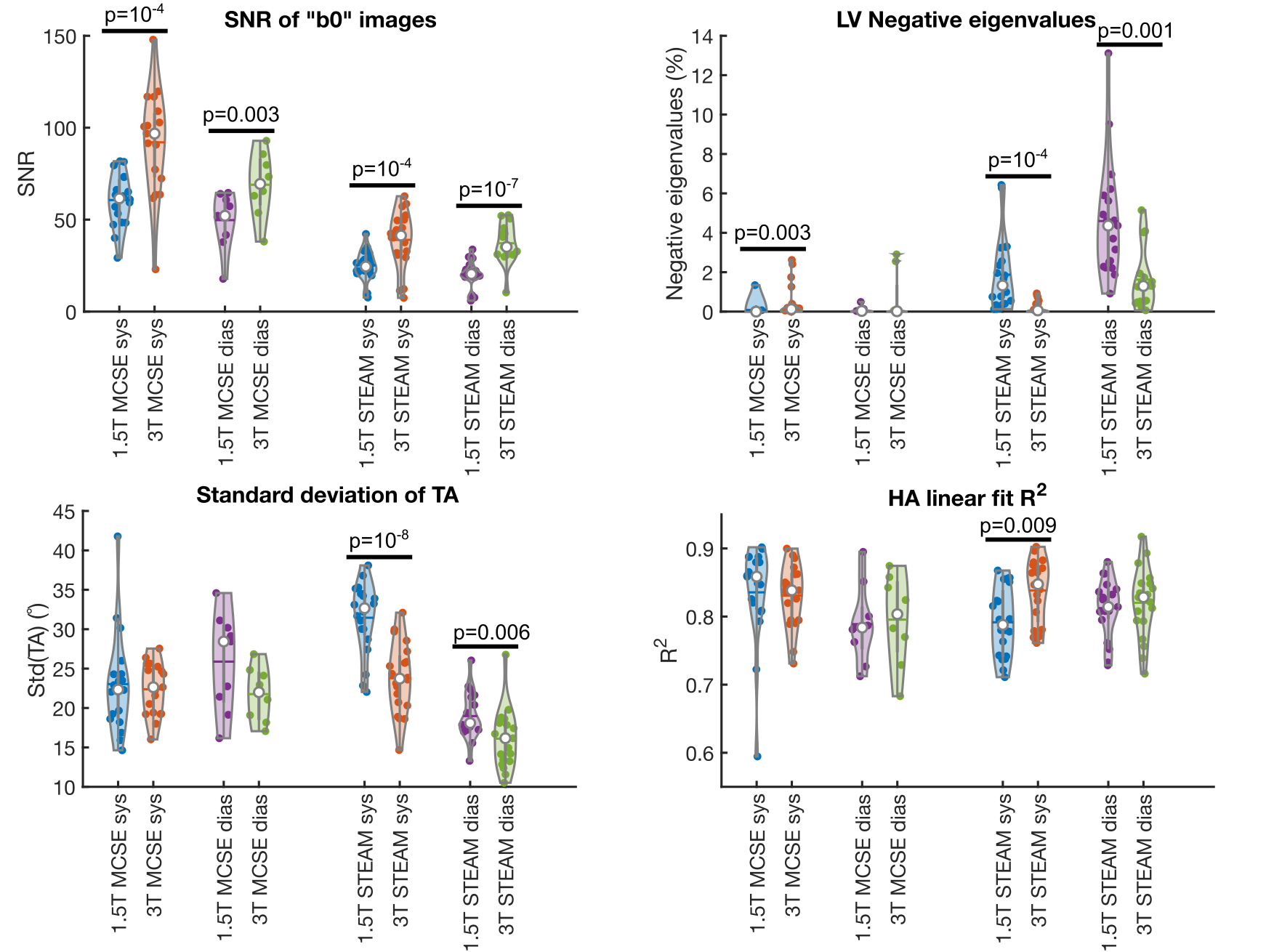
A maximum of 1 acquisition was deemed to have failed for all combinations of field strength, sequence and cardiac phase apart from MCSE in diastole where 11 (1.5T) and 12 (3T) acquisitions were rejected as the helix angle (HA) demonstrated <50% normal appearance circumferentially or the acquisition was abandoned due to poor image quality. Figure 1 demonstrates the quality of diffusion weighted images for both cardiac phases, sequences and field strengths in a successful acquisition. Figure 2 shows example DT-CMR maps in a different subject. Data quality was subjectively scored based on the HA map (figure 3, see caption for scoring) with improvements in quality at 3T for STEAM but not MCSE.Figure 4 compares typical DT-CMR parameters between field strengths, demonstrating differences for STEAM between field strengths for FA (systole), transmural HA gradient (systole) and E2A (sheetlet angle, both phases). Figure 5 compares DT-CMR data quality measures between field strengths. The SNR of “b0” data in both sequences and cardiac phases is higher at 3T. The number of LV myocardial pixels containing negative eigenvalues is higher at 1.5T for STEAM (both phases) but higher at 3T in systole for MCSE. The standard deviation of the transverse angle was lower in systole and diastole and the Pearson R2 of the transmural variation in HA was higher in systole for 3T using STEAM, suggesting better DT-CMR data quality.
Discussion
We have demonstrated that both STEAM and MCSE can be successfully used at both 1.5T and 3T (with the previously reported high failure rates of MCSE in diastolic phases[6]).While distances diffused are independent of field strength, SNR and difference in image artefacts between field strengths can affect the DT-CMR parameters measured. Here we show that parameters obtained using MCSE are minimally affected by field strength, but that the data quality in STEAM benefits from higher SNR at 3T. Some residual fat artefacts were observed using MCSE at 3T due to the larger chemical shift (figure 1), but these may be partially mitigated in future using binomial excitation pulses. While increased field strength seems to provide minimal benefit to the MCSE DT-CMR protocol evaluated here, the echo time reductions available to MCSE DT-CMR via high (>40mT/m) and ultrahigh strength gradients (>100mT/m) are currently only available at >1.5T.
Acknowledgements
This work was supported by British Heart Foundation Grant RG/19/1/34160.References
1. Khalique Z et al. JACC Imaging 2020 doi: 10.1016/j.jcmg.2019.07.016
2. Nielles-Vallespin S et al. JACC 2017 doi: 10.1016/j.jacc.2016.11.051
3. Sharrack N et al. JCMR 2022 doi:10.1186/s12968-022-00892-y.
4. Welsh C et al. IEEE TMI 2015. doi: 10.1109/TMI.2015.2411571
5. Stoeck C et al. MRM 2016. doi: 10.1002/mrm.25784
6. Scott AD et al. JCMR 2018 doi: 10.1186/s12968-017-0425-8
Figures