0607
Mitigating Geometric Distortion & Susceptibility Artifacts in cDTI via SAP-M2-EPI: A feasibility study1Cardiovascular Innovation Research Center (CIRC), Heart, Vascular, and Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Myocardium, Heart, cardiac diffusion, Motion compensated gradients, Aliasing, geometric distortion, PROPELLER MRI
Motivation: We aimed to enhance in vivo cardiac diffusion tensor imaging (cDTI), a technique challenged by limitations, especially in high-BMI patients, causing notable aliasing and distortion issues.
Goal(s): Our primary goal was to introduce and validate Short-Axis-PROPELLER-M2-EPI (SAP-M2-EPI) for cDTI. The focus was on reducing aliasing and distortion artifacts while ensuring robust motion correction.
Approach: SAP-M2-EPI combines motion-compensated diffusion gradients with PROPELLER, effectively minimizing motion artifacts and suppressing aliasing and distortion.
Results: Our study shows that SAP-M2-EPI successfully mitigates motion artifacts and significantly reduces aliasing and distortion, particularly beneficial for high-BMI patients. This innovative approach holds great promise for enhancing cDTI diagnostic accuracy.
Impact: Impact: SAP-M2-EPI’s success offers clinicians a potent tool for enhancing cDTI diagnoses, especially in high-BMI patients. It opens doors to in-depth cardiac research, encourages further methodological innovations, and ultimately promises better patient care through more accurate imaging.
BACKGROUND
Cardiac diffusion tensor imaging (cDTI) is a promising non-invasive, contrast-free technique for investigating myocardial microstructure, offering valuable insights into cardiac diseases.1-3 Despite its potential, cDTI encounters challenges such as motion-related signal loss, geometric distortions, susceptibility-related artifacts, and low signal-to-noise ratios (SNR). Notably, aliasing artifacts are a significant issue, particularly in patients with higher body mass index (BMI).4-6 To address these challenges, we propose an innovative approach that combines second-order motion-compensated diffusion encoding gradients (M2) with the short-axis PROPELLER (SAP) MRI technique. This integration effectively mitigates aliasing, field inhomogeneities, and motion artifacts. SAP-M2-EPI not only resolves these issues but also facilitates efficient free-breathing cDTI.THEORY
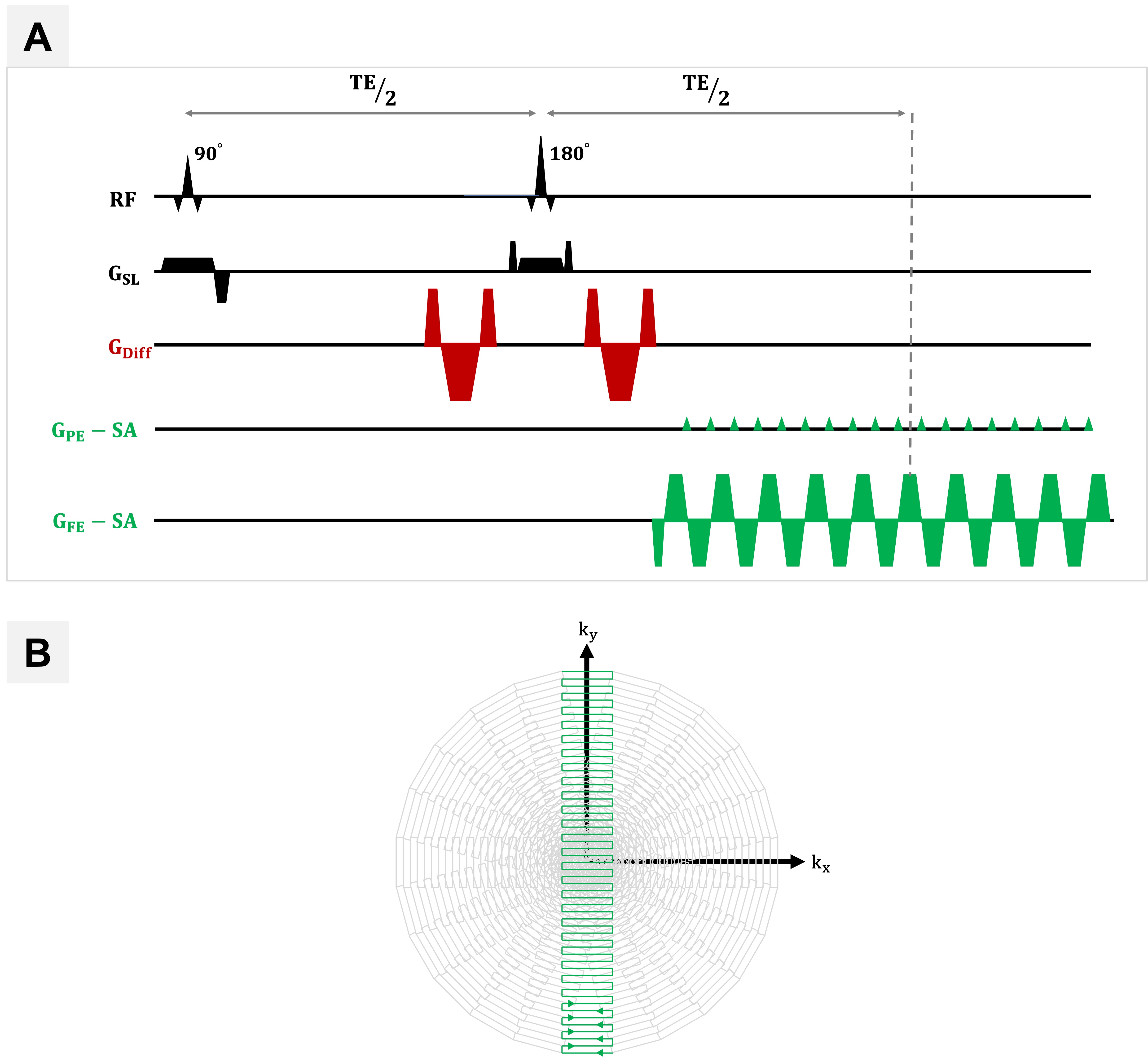
cDTI holds great promise for enhancing our understanding of cardiac diseases and their impact on myocardial microstructure. However, its application to the dynamic environment of the beating heart is challenging. M2-ssEPI7,8 offers fast data acquisition and reduced motion susceptibility but is limited by issues like geometric distortion, aliasing, and misalignment due to field inhomogeneities. Multi-shot EPI (msEPI), while improves SNR and reduces distortion but often requires longer acquisition times, making it susceptible to motion-induced artifacts. To overcome these challenges, one approach is using non-Cartesian k-space trajectories, such as the PROPELLER method. PROPELLER collects data with blades instead of single lines, facilitating the detection and correction of motion-induced phase variations. However, it can still be sensitive to off-resonance and cause geometric distortion. Short-axis PROPELLER-EPI (SAP) addresses these issues by reducing the echo spacing (ESP) compared to the conventional PROPELLER (long-axis PROPELLER), effectively reducing geometric distortion. The combination of SAP-EPI with M2 (Figure 1) aims to mitigate the limitations of M2-ssEPI and enhance the image quality of cDTI data.METHODS
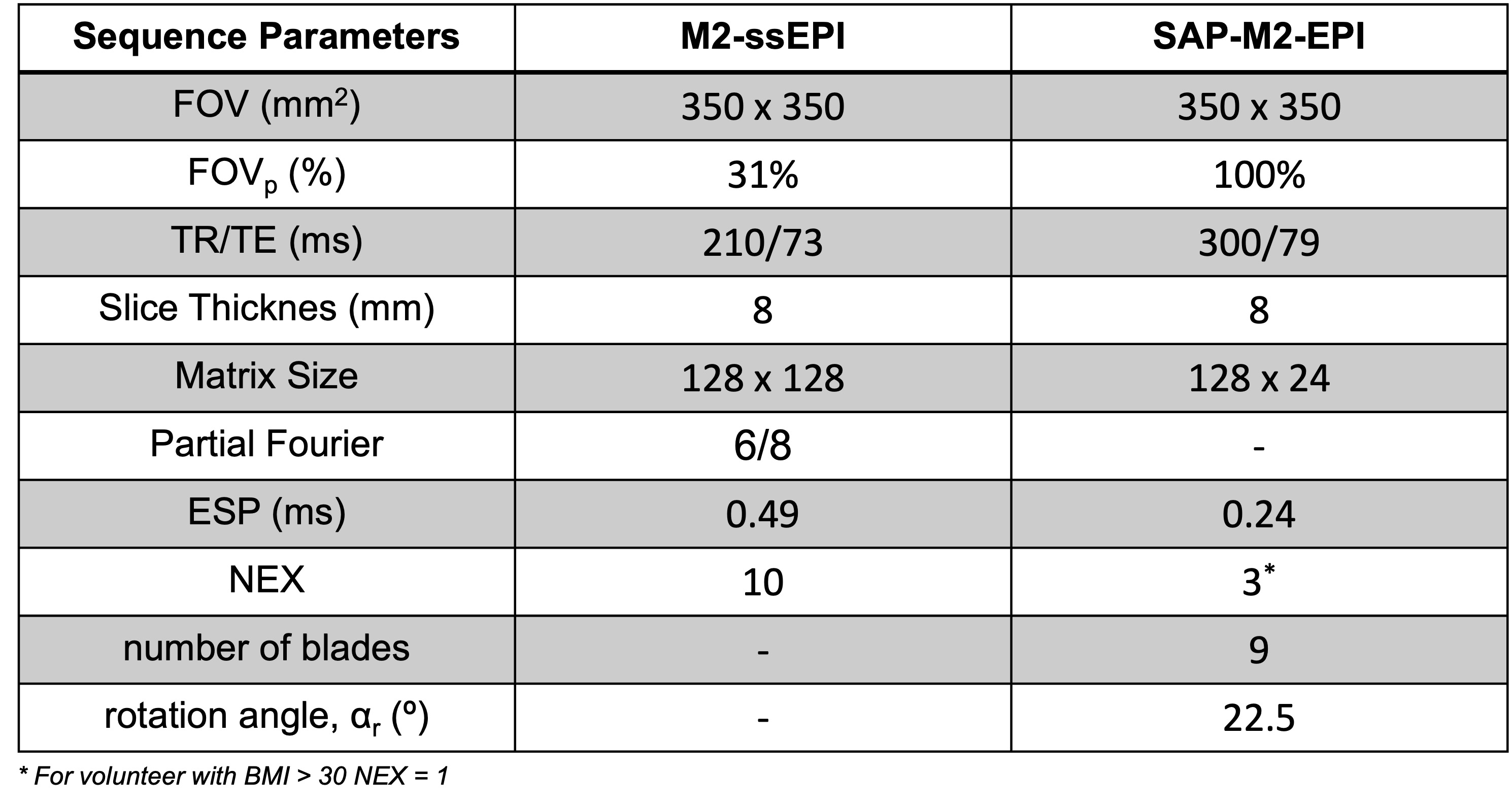
Imaging was conducted using a 3T clinical MRI system (Prisma, Siemens Healthineers, Erlangen, Germany) with a maximum gradient strength of 80 mT/m and a slew rate of 100 T/m/s. A standard 32-channel anteroposterior surface coil was used for signal reception. Data acquisition involved modifying a custom EPI sequence by incorporating M2 gradients. This modified sequence was employed for both M2-ssEPI and SAP-M2-EPI data acquisitions with the parameters listed in Figure 2. Free-breathing, ECG-triggered whole LV cDTI was conducted on a total of 10 healthy volunteers (mean age: 33 $$$\pm$$$12 years; 4 females) who participated with varying BMI ranges: BMI < 25 (4 volunteers), 25 < BMI < 28 (5 volunteers), and BMI > +30 (1 volunteer). Each subject underwent the acquisition of three mid-ventricular short-axis slices. Manual LV segmentation and shape comparisons were conducted by manually segmenting epicardial and endocardial borders of M2-ssEPI, SAP-M2-EPI, and CINE short-axis (CINE-SAX) datasets. Geometric distortions' impact on LV shape was quantitatively assessed using the Dice similarity coefficient (DSC) and misregistration area.RESULTS & DISCUSION
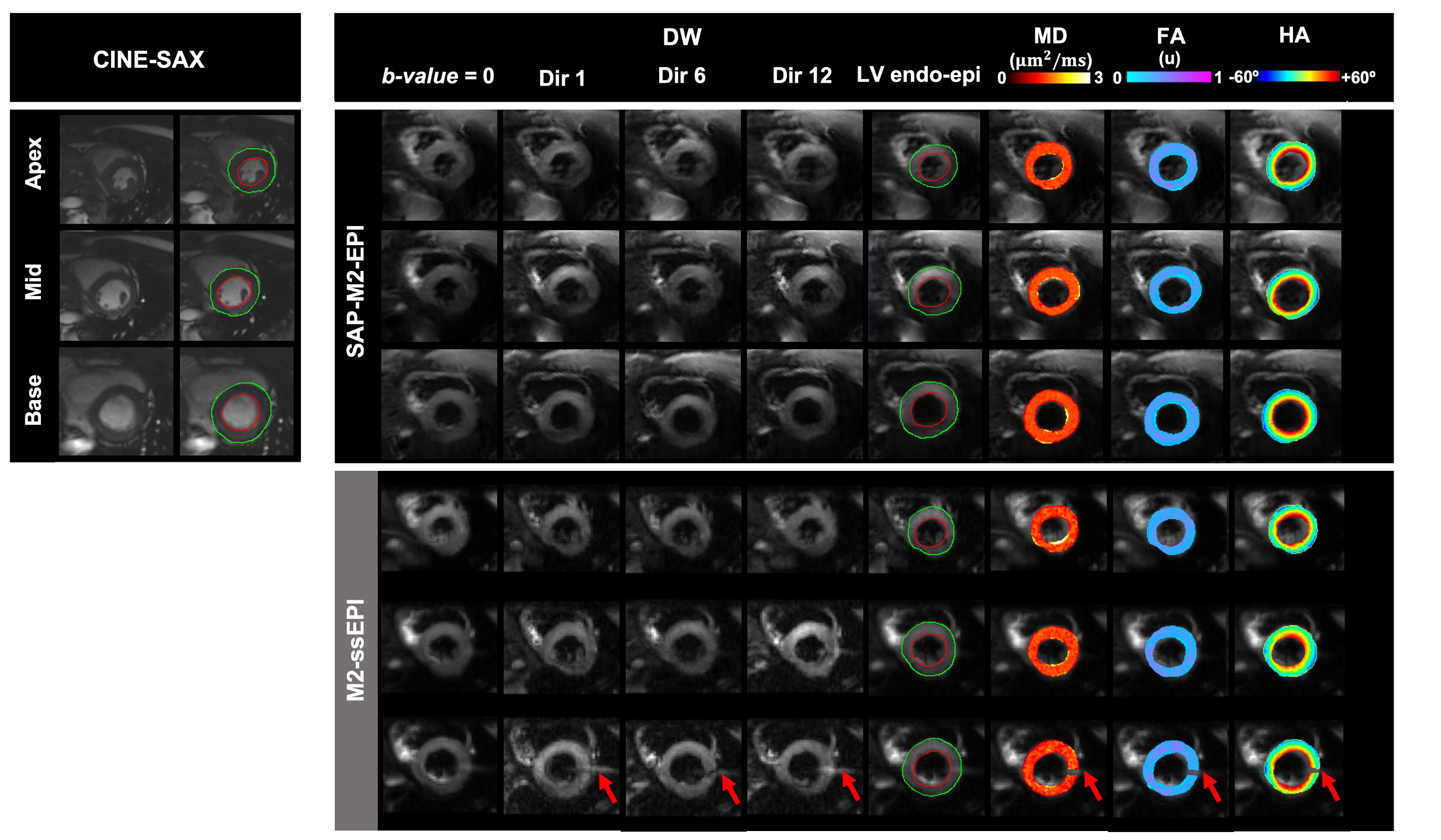
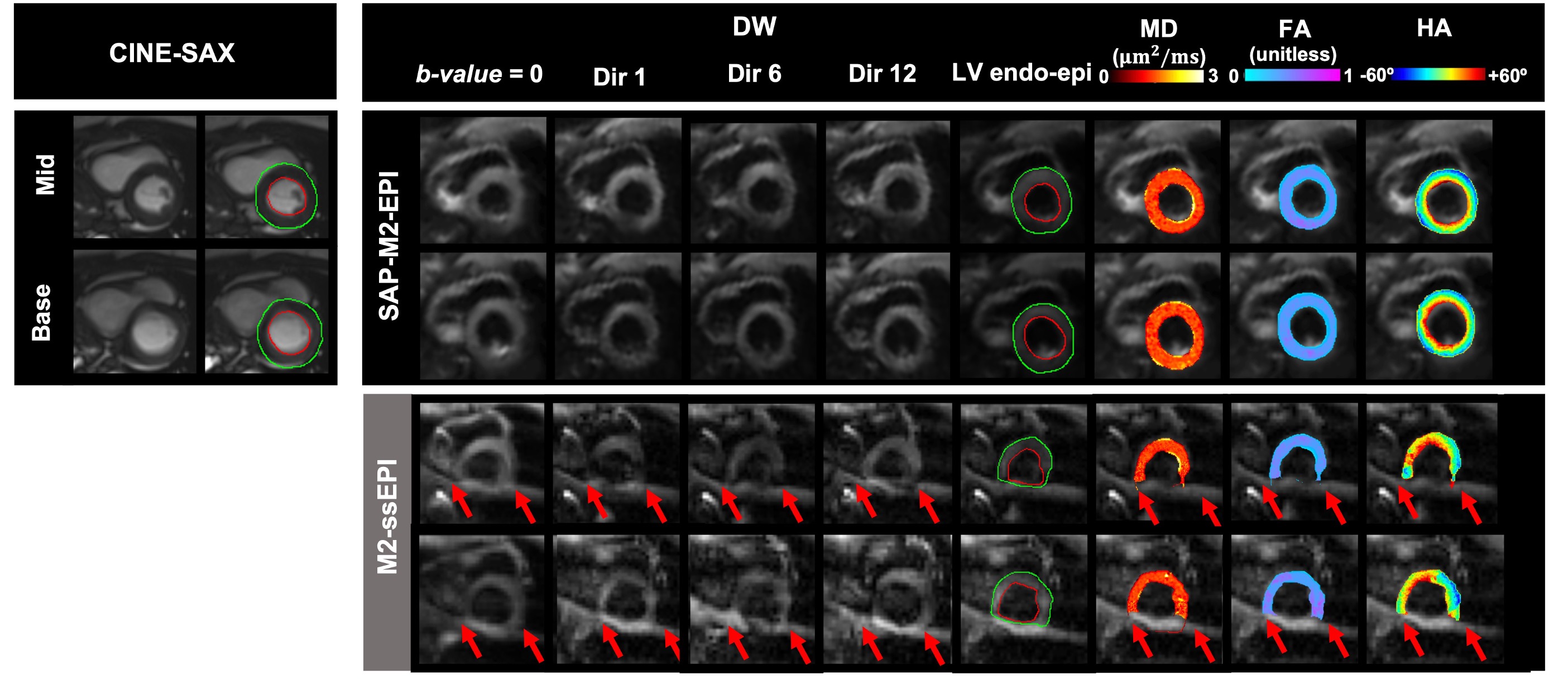
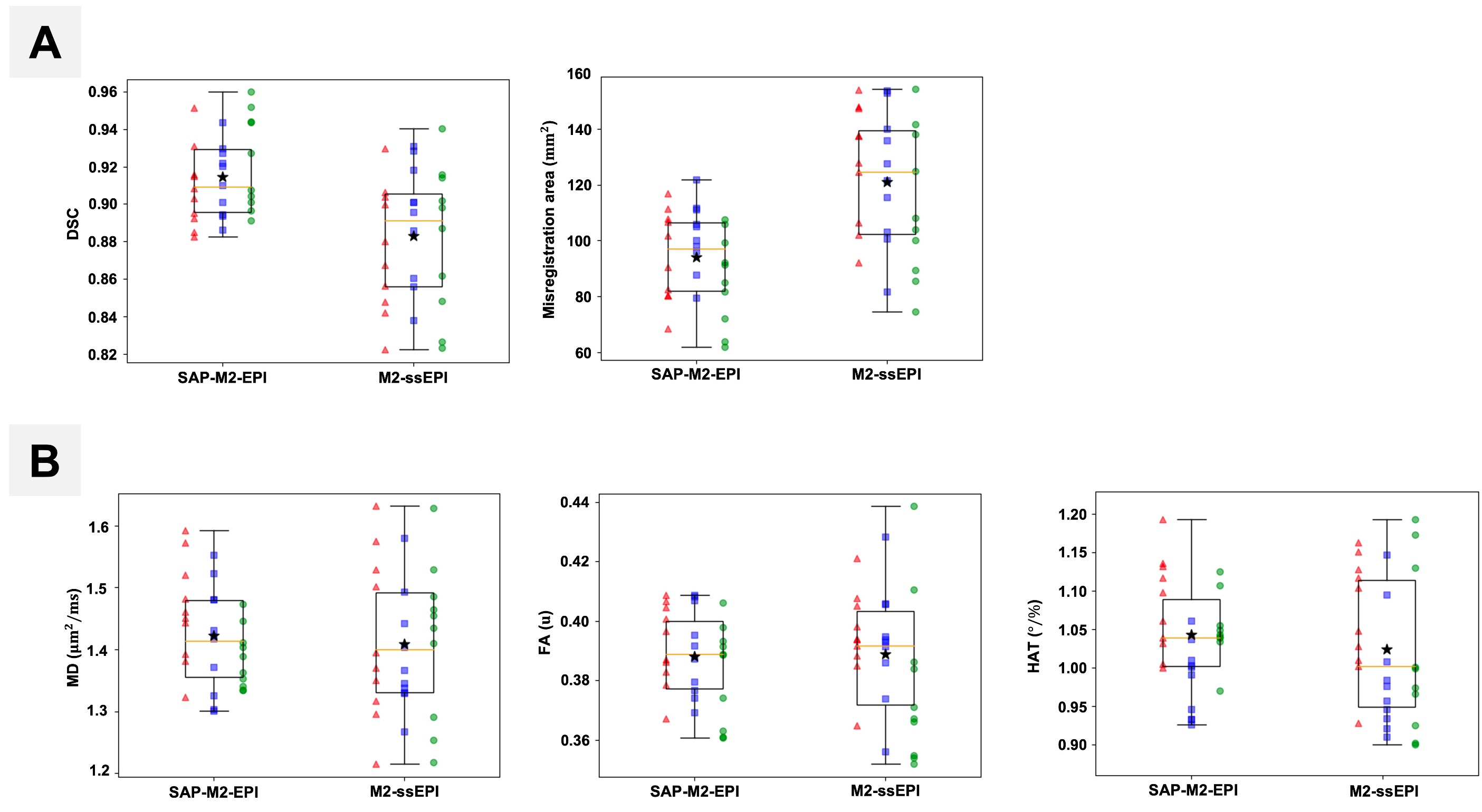
Figure 3 displays DW images, mean diffusivity (MD), fractional anisotropy (FA), and HA for a volunteer with a BMI of 25. Both SAP-M2-EPI and M2-ssEPI sequences yielded high-quality LV images with minimal motion artifacts and off-resonance effects. However, a minor aliasing artifact was noted in the base slice of the M2-ssEPI images. For the volunteer with a BMI exceeding 30 (Figure 4), SAP-M2-EPI significantly outperformed M2-ssEPI, which exhibited severe aliasing artifacts. SAP-M2-EPI significantly reduced aliasing artifacts and geometric distortions. Shorter ESP and higher pseudo bandwidth (pBW) contributed to improved image fidelity, especially in EPI-based sequences. Figure 5A illustrates the DSC and misregistration area of LV in DW images compared to CINE-SAX images for all volunteers across all slices, excluding the volunteer with BMI > 30. This highlights SAP-M2-EPI's robustness to off-resonance artifacts, boasting a mean DSC of 0.92 and a misregistration area of 90 mm² compared to M2-ssEPI with a DSC of 0.89 and a misregistration area of mm2. Overall, M2-ssEPI performed well with subjects having BMI<28, exhibiting strong agreement between SAP-M2-EPI and M2-ssEPI. Parameter maps of DTI in Figure 5B showed consistent uniformity across all image slices. However, M2-ssEPI demonstrated limitations with higher BMI subjects, making SAP-M2-EPI a more reliable option for clinical practice. This study highlights the potential of SAP-M2-EPI in overcoming challenges associated with high BMI, a critical factor in cardiovascular patient care.CONCLUSION
In conclusion, our work advances in vivo cDTI by improving image quality with respect to geometric distortion in higher BMI patients using a short-axis PROPELLER (SAP) EPI readout. SAP-EPI could potentially enable new insights in scenarios where magnetic susceptibility and B0 inhomogeneity result in severe geometric distortion.Acknowledgements
This work was partially funded by the National Institute of Health R01 HL151704, the National Institute of Health R01HL159010, and the National Institute of Health R01 HL135242.References
[1] R. J. van Gorkum, C. Guenthner, A. Koethe, C. T. Stoeck, and S. Kozerke, “Characterization and correction of diffusion gradient-induced eddy currents in second-order motion-compensated echo-planar and spiral cardiac DTI,” Magnetic Resonance in Medicine, vol. 88, no. 6, pp. 2378–2394, 2022.
[2] R. R. Edelman, J. Gaa, V. J. Wedeen, E. Loh, J. M. Hare, P. Prasad, and W. Li, “In vivo measurement of water diffusion in the human heart,” Magnetic resonance in medicine, vol. 32,no. 3, pp. 423–428, 1994.
[3] T. G. Reese, R. M. Weisskoff, R. N. Smith, B. R. Rosen, R. E. Dinsmore, and V. J. Wedeen, “Imaging myocardial fiber architecture in vivo with magnetic resonance,” Magnetic Resonance in Medicine, vol. 34, no. 6, pp. 786–791, 1995.
[4] C. Nguyen, Z. Fan, B. Sharif, Y. He, R. Dharmakumar, D. S. Berman, and D. Li, “In vivo three-dimensional high resolution cardiac diffusion-weighted mri: a motion compensated diffusion-prepared balanced steady-state free precession approach,” Magnetic resonance in medicine, vol. 72, no. 5, pp. 1257–1267, 2014.
[5] J. Dou, T. G. Reese, W.-Y. I. Tseng, and V. J. Wedeen, “Cardiac diffusion mri without motion effects,” Magnetic Resonance in Medicine, vol. 48, no. 1, pp. 105–114, 2002.
[6] C. L. Welsh, E. V. DiBella, and E. W. Hsu, “Higher-order motion-compensation for in vivo cardiac diffusion tensor imaging in rats,” IEEE Transactions on medical imaging, vol. 34, no. 9, pp. 1843–1853, 2015.
[7] C. Nguyen, Z. Fan, Y. Xie, J. Pang, P. Speier, X. Bi, J. Kobashigawa, and D. Li, “In vivo diffusion-tensor MRI of the human heart on a 3 tesla clinical scanner: An optimized second order(m2) motion compensated diffusion-preparation approach,” Magnetic resonance in medicine, vol. 76, no. 5, pp. 1354–1363, 2016.
[8] C. T. Nguyen, A. G. Christodoulou, J. Coll-Font, S. Ma, Y. Xie, T. G. Reese, C. Mekkaoui, G. D.Lewis, X. Bi, D. E. Sosnovik, et al., “Free-breathing diffusion tensor MRI of the whole left ventricle using second-order motion compensation and multitasking respiratory motion correction,” Magnetic resonance in medicine, vol. 85, no. 5, pp. 2634–2648, 2021.
Figures