0606
Biventricular Myocardial Kinetic Energy Distribution in Patients With Repaired Tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Taiwan, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Taiwan, Hsinchu, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Taiwan/Department of Pediatrics, National Yang-Ming University, Taiwan, Hsinchu, Taiwan
Synopsis
Keywords: Myocardium, Heart
Motivation: Patients with repaired Tetralogy of Fallot (rTOF) have varied cardiac structures, yet there's a current lack of analysis on their cardiac kinetic energy.
Goal(s): We aim to assess myocardial kinetic energy (KE) differences between patients and normal groups.
Approach: We utilized tissue phase mapping images combined with MATLAB programs to calculate myocardial kinetic energy.
Results: The results revealed differences in myocardial kinetic energy values between patients and normal groups. Besides, significant variations were observed in the proportional values across three directions, along with notable differences in the KE systolic-to-diastolic ratio of the right ventricle.
Impact: Differential myocardial kinetic energy serves as a novel indicator for evaluating cardiac function in rTOF patients. It aids in early detection of cardiac abnormalities, potentially identifying the optimal timing for pulmonary valve replacement surgery.
Introduction
Despite undergoing corrective surgery in infancy, the pulmonary valve dysfunction in patients with repaired Tetralogy of Fallot (rTOF) may lead to pulmonary regurgitation (PR), gradual deterioration of cardiac function, and irreversible myocardial damage.1 In rTOF patients, impaired global function was accompanied by altered biventricular global velocities.2 Approximately 20% of rTOF patients may further develop LV dysfunction because of adversely impact of right ventricular (RV) dilation and dysfunction on LV.3,4 Quantification of ventricular flow kinetic energy (KE) in rTOF was reported.5 However, the myocardial KE in rTOF has not been discussed thoroughly. Previous study has used ROI-based methods to calculate the KE of the ventricles, but this may lead to an underestimation of KE.6 In this study, we employed tissue phase mapping (TPM) to compute biventricular myocardial KE in rTOF patients. This study aimed to assess the myocardial KE proportion of different directions and different cardiac phases in rTOF patients.Methods
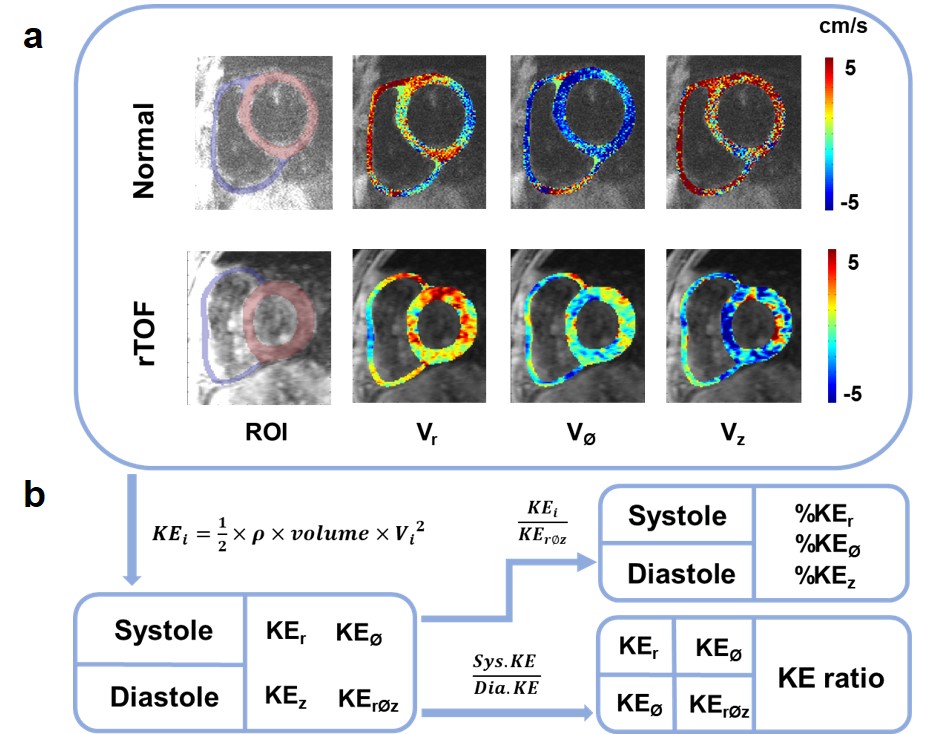
This study recruited 32 rTOF patients (22±4 y/o; male/female=21/11) and 32 age-matched normal controls (22±1 y/o; male/female=15/17). Images were acquired at a 3-T MR scanner (Tim Trio or Skyra, Siemens) with prospective ECG triggering and respiratory navigator-echo. A 2D dark-blood fast low-angle shot sequence was performed for TPM acquisitions with TR/TE=6.5/4.2 ms, pixel size=1.17x1.17 mm2, slice thickness=6 mm, flip angle=7°, acceleration factor=5, Venc=15 and 25 cm/s for in-plane and through-plane motions, respectively, and temporal resolution=26 ms. In Figure 1(a), the region-of-interest (ROI) were determined manually in LV and RV with a self-developed program for computing radial (Vr), circumferential (VØ), and longitudinal (Vz) velocities. Figure 1(b) illustrates the calculation of the myocardial KE amplitude in basal, mid, and apical regions in three directions, along with the summation of them (KErØz) during systolic and diastolic phases. In the previous study, KE was calculated based on the region-of-interest (ROI).6 In our study, we compute KE on a pixel-wise basis by the following equation:KEi = 1/2 × ρ × volume × Vi2 [1]
where Vi represents the voxelwise velocity along direction (r, ø, or z); ρ the myocardial density (1050 kg/m3); and volume the volume of one single voxel. The KE proportion in three directions were calculated during systolic and diastolic phases. The ratio of systolic-to-diastolic KE was also computed. Two-tailed Student t test was performed when appropriate. p<0.05 was considered statistical significance.
Results
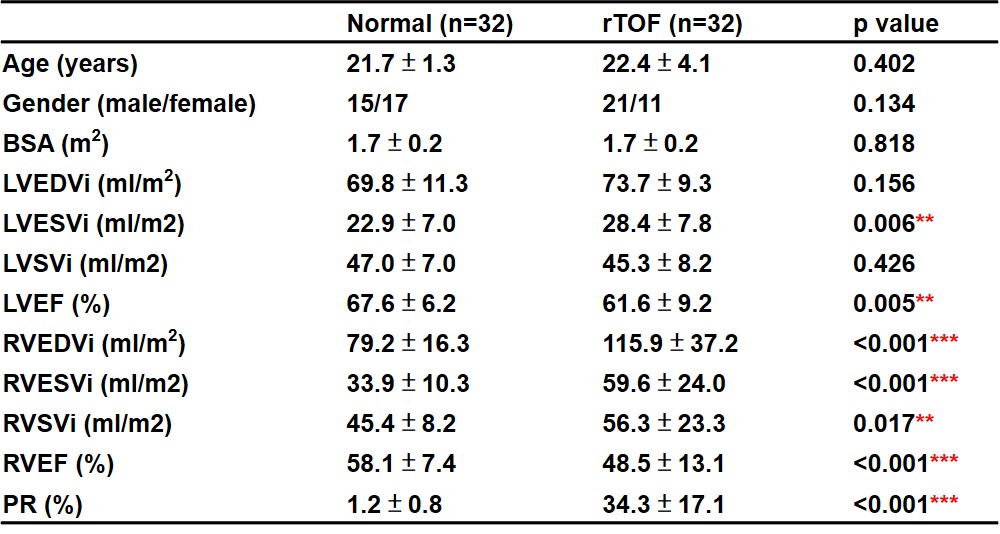
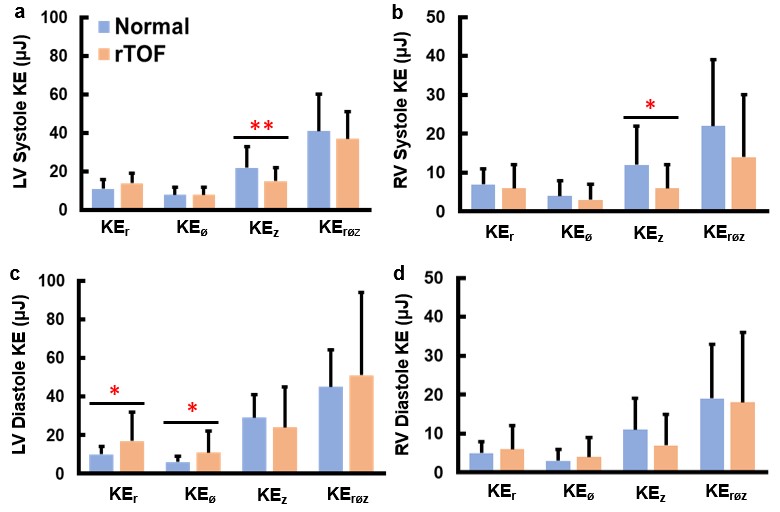
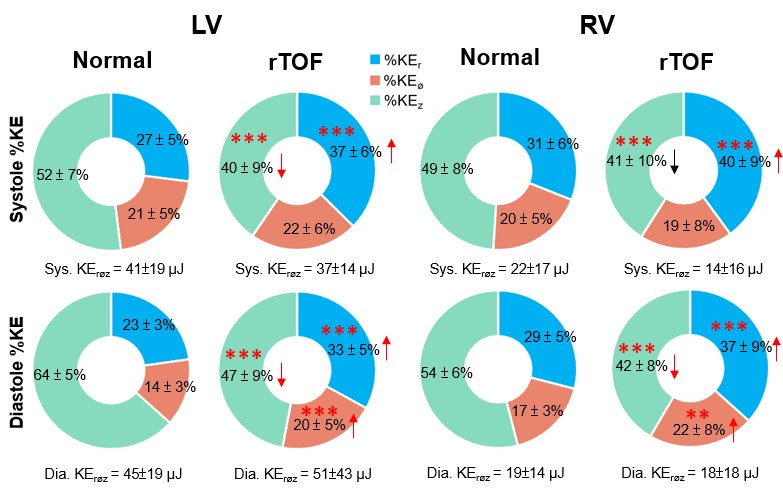
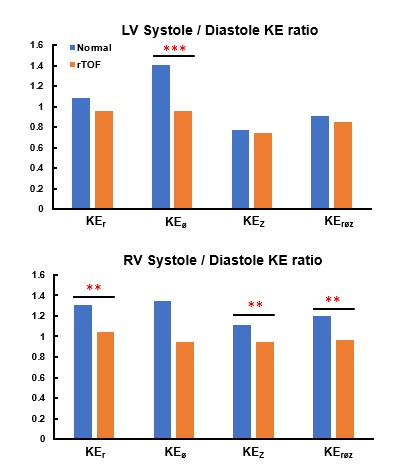
In Table 1, rTOF group exhibited dilated RV and decreased global RV and LV ejection fraction (RVEF and LVEF) even though the RVEF and LVEF were still within the normal referencing ranges. The rTOF group presented lower LV and RV systolic KEz (both p<0.01) and increased diastolic KEr and KEØ (both p<0.05) than normal group (Figure 2). In Figure 3, the rTOF group exhibited a significantly higher systolic and diastolic %KEr and diastolic %KEØ than the normal group in LV and RV (all p<0.001). The rTOF group presented decreased systolic and diastolic %KEz in LV and RV (all p<0.001). As for KE ratio between systolic and diastolic phases (Figure 4), the rTOF group exhibited lower ratios in LV KEØ, RV KEr, KEz and KErØz than that in normal group (p<0.01-0.001).Discussion and Conclusion
In this study, the pixel-wise %KE presented more altered indices than KE amplitudes. The altered systole-to-diastole KE ratio in rTOF group manifested in circumferential direction in LV and in radial and longitudinal directions in RV. The altered %KEr and preserved KEr amplitude in rTOF group might illustrate that %KEr could potentially reveal myocardial abnormalities in an early stage. The lower RV systole-to-diastole KE ratio in rTOF group suggested that the rTOF group may need to exert more effort in diastolic function.7 A previous study reported altered longitudinal and circumferential wall motion in rTOF patients.8 In this study, we also observed abnormal myocardial motion in the three directions in a new insight of myocardial KE evaluated by TPM, describing the usefulness of KE-related indices for detection of early myocardial abnormalities in rTOF patients. The decreased systolic and diastolic %KEz were compensated by increased systolic and diastolic %KEr as well as %KEØ in both LV and RV. This compensatory mechanism might be viewed as to maintain cardiac function and could potentially involve structural changes in the heart.9 In systole, the decreased %KEz was compensated solely by increased %KEr. However, in diastole, the decreased %KEz was compensated by increased %KEr and %KEØ, indicating that %KEØ may be a key factor influencing diastolic function. In conclusion, the pixel-wise %KE could potentially reveal myocardial abnormalities in an early stage in rTOF patients. The altered systole-to-diastole KE ratio illustrated the deteriorated diastolic function in rTOF group.Acknowledgements
This study has received funding by the Veterans General Hospitals, University System of Taiwan Joint Research Program and Kaohsiung Veterans General Hospital.References
1. Apitz, Christian, Gary D. Webb, and Andrew N. Redington. "Tetralogy of Fallot." The Lancet 374.9699 (2009): 1462-1471.
2. Ruh A, Sarnari R, Berhane H, et al. Impact of age and cardiac disease on regional left and right ventricular myocardial motion in healthy controls and patients with repaired tetralogy of fallot. Int J Cardiovasc Imaging. 2019;35(6):1119-1132.
3. Khalaf, Alexander, et al. "Right-and left-ventricular strain evaluation in repaired pediatric tetralogy of Fallot patients using magnetic resonance tagging." Pediatric cardiology 34 (2013): 1206-1211.
4. Broberg, Craig S., et al. "Prevalence of left ventricular systolic dysfunction in adults with repaired tetralogy of Fallot." The American journal of cardiology 107.8 (2011): 1215-1220.
5. Jeong D, Anagnostopoulos PV, Roldan-Alzate A, et al. Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot. J Thorac Cardiovasc Surg. 2015;149(5):1339-1347.
6. Ke SY, Weng KP, Chang MC, et al. Differential Adaptation of Biventricular Myocardial Kinetic Energy in Patients With Repaired Tetralogy of Fallot Assessed by MR Tissue Phase Mapping. J Magn Reson Imaging. 2023;57(5):1492-1504.
7. Loke YH, Capuano F, Kollar S, et al. Abnormal Diastolic Hemodynamic Forces: A Link Between Right Ventricular Wall Motion, Intracardiac Flow, and Pulmonary Regurgitation in Repaired Tetralogy of Fallot. Front Cardiovasc Med. 2022;9:929470. Published 2022 Jul 14.
8. Berganza FM, de Alba CG, Özcelik N, Adebo D. Cardiac Magnetic Resonance Feature Tracking Biventricular Two-Dimensional and Three-Dimensional Strains to Evaluate Ventricular Function in Children After Repaired Tetralogy of Fallot as Compared with Healthy Children. Pediatr Cardiol. 2017;38(3):566-574.
9. Mauger CA, Govil S, Chabiniok R, et al. Right-left ventricular shape variations in tetralogy of Fallot: associations with pulmonary regurgitation. J Cardiovasc Magn Reson. 2021;23(1):105. Published 2021 Oct 7.
Figures