0604
Right ventricular electromechanical discoordination predict long-term clinical outcomes in patients with pulmonary arterial hypertension1Fuwai Hospital, Chinese Academy of Medical Sciences, Beijing, China, 2Université Paris-Saclay, CentraleSupélec, ENS Paris-Saclay, CNRS:LMPS, Paris, France, 3MR Research Collaboration, Siemens Healthineers Ltd., Beijing, China, 4MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Heart Failure, Myocardium, pulmonary hypertension; electromechanical discoordination;
Motivation: Non-invasive and accurate evaluation of right ventricular (RV) function in pulmonary arterial hypertension (PAH) is of urgent need in clinical practice.
Goal(s): To investigate the clinical implications of RV electromechanical dyssynchrony which were non-invasively derived from cardiac MRI.
Approach: Calculate systolic stretch fraction (SSF) and diastolic relaxation fraction (DRF) based on strain MRI and test their prognostic values in an observation prospective PAH cohort.
Results: SSF-RV-Longitudinal could independently predict the clinical worsening.
Impact: The present study first reported SSF-RV-Longitudinal as a novel parameter to evaluate RV function, which could predict the clinical worsening in PAH patients.
Introduction
Right ventricular (RV) function is a major prognostic determining factor in pulmonary arterial hypertension (PAH). The progression of PAH will inevitably result in RV remodeling[1], which can be manifested as electrical dyssynchrony (E-dys) and mechanical dyssynchrony (M-dys). The purpose of this study was to investigate clinical implications of RV electromechanical dyssynchrony in patients with PAH by using novel systolic stretch and diastolic relaxation discoordination indexes which were noninvasively derived from cardiac magnetic resonance (CMR).Methods
This is an observational prospective cohort study. Seventy-six treatment-naïve, newly diagnosed PAH patients by right heart catheterization (RHC) from a prospective registry[2] and agreed to undergo CMR scanning were consecutively recruited between January 2011 and December 2017. All enrolled patients received RHC and CMR scanning within one week at the baseline. Cardio-pulmonary hemodynamic parameters were collected during RHC. Twelve-lead ECGs were collected a day before RHC. QRS duration was described as the widest interval in any of 12 leads and was acquired digitally. The QRS duration z-score were calculated adjusting by age and gender[3], with E-dys defined as z-score ≥2. CMR was performed on a 1.5 T scanner (MAGNETOM Avanto, Siemens Healthineers AG, Erlangen, Germany). Breath-hold short-axis cine images encompassing the whole LV and RV from apex to base were acquired using balanced steady-state free-precession (bSSFP) sequence (repetition time/echo time, 3.2 ms/1.6 ms; temporal resolution, 34 ms; flip angle, 60 degrees; field of view, 280×340 mm2; matrix, 150×256; voxel size, 1.9mm×1.3mm; slice thickness, 8 mm). Acquired CMR images were analyzed using a prototype software (Trufi Strain V2.1, Siemens Healthineers AG, Erlangen, Germany). Comprehensive analysis of biventricular volumetric, strain and mechanical dyssynchrony were performed using Trufi Strain V2.1. The conventional M-Dys was calculated as a standard deviation of all time-to-peak strain values in the radial, circumferential, or longitudinal directions. The novel myocardial discoordination indexes, including systolic stretch fraction (SSF)[4] and diastolic relaxation fraction (DRF)[5] were also calculated in the radial, circumferential, or longitudinal directions using Matlab (The Mathworks Inc.) software. The postprocessing algorithm for calculating SSF and DRF was summarized in Figure 1. The follow-up was documented from the date the patients underwent RHC to the occurrence of endpoint. The designed primary endpoint was clinical worsening event, a composite of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term clinical response. Each patient was followed at 6-month ± 2-week intervals.Results
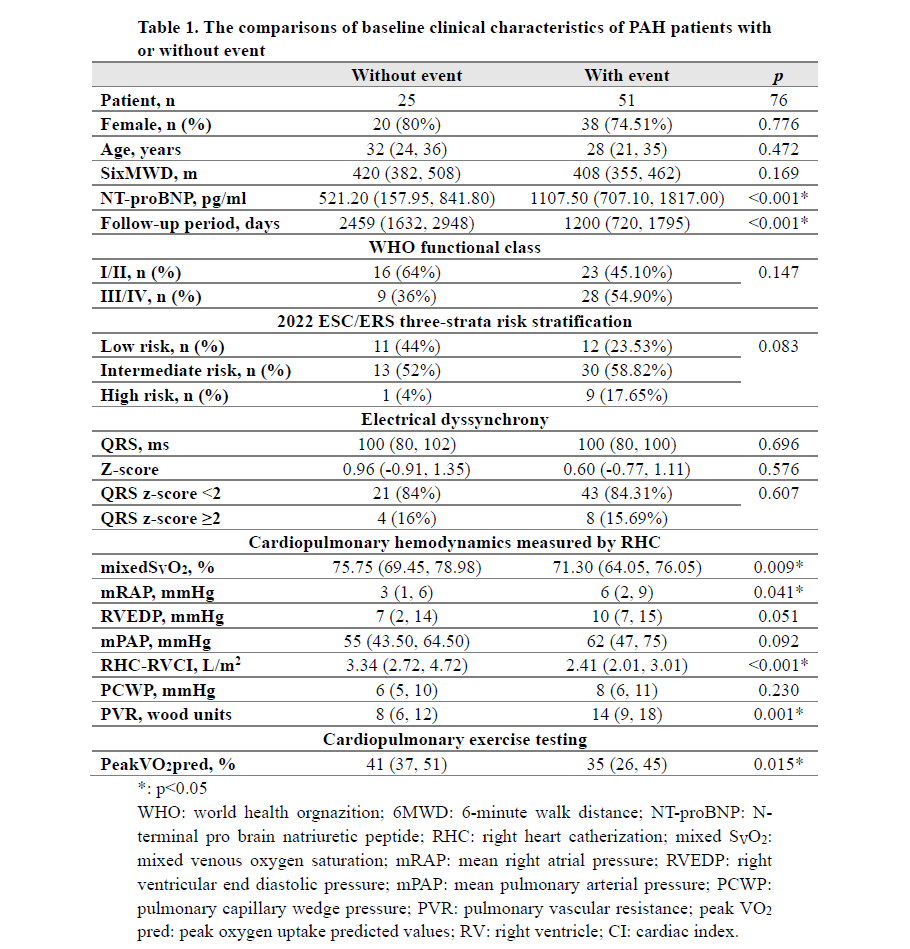
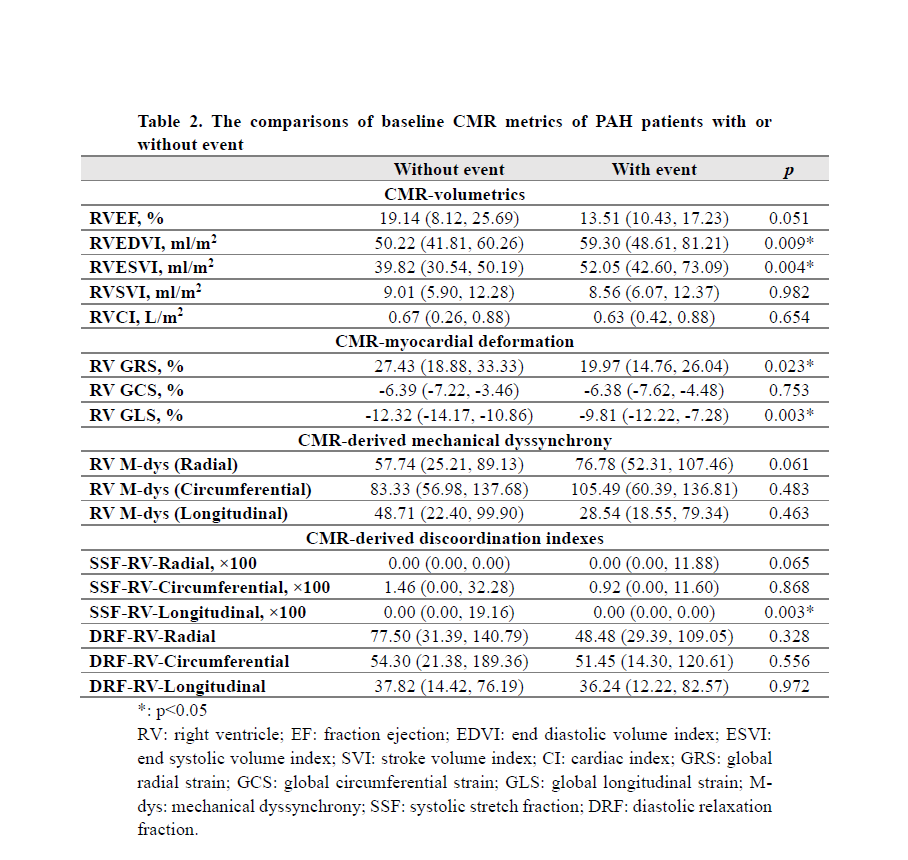
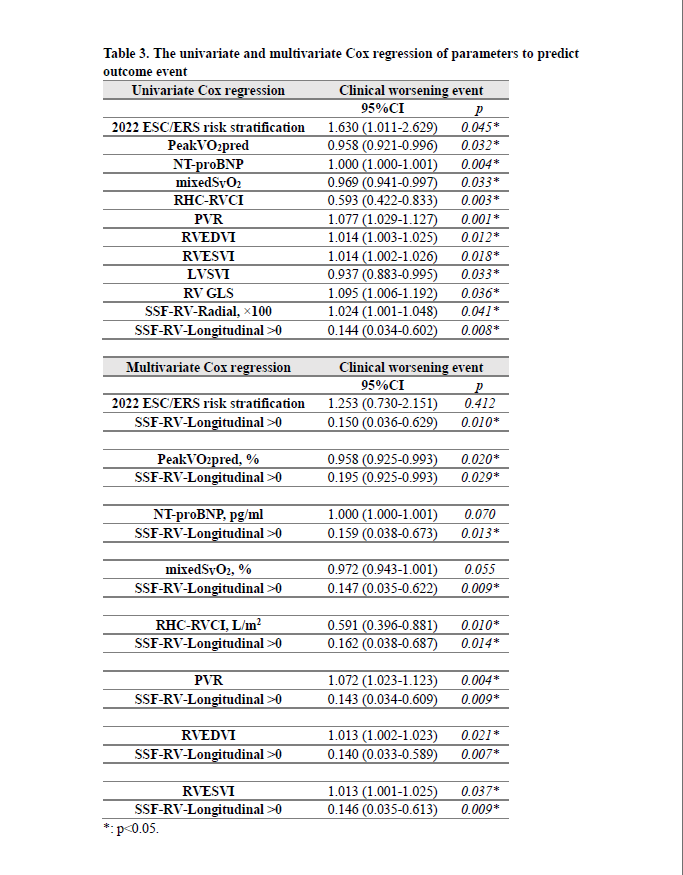
Seventy-six PAH patients (58 female, with median age 30) were enrolled in this analysis. The median follow-up period was 1550 (range 26 to 3919) days, during which 51 patients had clinical worsening events (including 29 all-cause mortality) as showed in Table 1. Comparisons of baseline clinical characteristics showed patients with event had significantly higher levels of NT-proBNP, mean right atrial pressure, right ventricular end diastolic pressure, and pulmonary vascular resistance (PVR), but significantly lower mixed venous oxygen saturation (mixedSVO2), and RHC-RV cardiac index (RHC-RVCI). Comparisons of baseline CMR metrics showed patients with event had significantly larger RV end diastolic volume index (RVEDVI), RV end systolic volume index (RVESVI), and SSF-RV-Longitudinal, but significantly lower RV global radial strain (RV GRS) and RV global longitudinal strain (RV GLS, Table 2). The univariate Cox regression found 2022 ESC/ERS risk stratification, peak oxygen uptake predicted values (peakVO2 pred), NT-proBNP, mixedSVO2, RHC-RVCI, PVR, RVEDVI, RVESVI, RV GLS, SSF-RV-Radial, and SSF-RV-Longitudinal >0 could predict clinical worsening event (Table 3). Furthermore, the multivariate Cox regression found SSF-RV-Longitudinal >0 could independently predict clinical worsening event after adjusting by 2022 ESC/ERS risk stratification, peakVO2 pred, NT-proBNP, mixedSVO2, RHC-RVCI, PVR, RVEDVI, and RVESVI. The Kaplan-Meyer analysis showed patients with SSF-RV-Longitudinal >0 had better prognosis than patients with SSF-RV-Longitudinal =0 (Log rank: p = 0.002, Figure 2-D). In addition, SSF-RV-Longitudinal had better ability to predict prognosis than RHC-RVCI (Log rank: p = 0.017), RV GLS (Log rank: p = 0.025), and RVEDVI (Log rank: p = 0.041) (Figure 2-A to C).Discussion
SSF is a quantification of magnitude and duration of regional positive strain rate deflections, indicating myocardial stretching during ventricular systole. In this study, RV-SSF measured in the longitudinal direction was firstly reported to have the ability to predict clinical worsening of PAH patients. In addition, at the baseline, SSF-RV-Longitudinal had better ability to distinguish patients who might have clinical worsening than conventional parameters, like RVCI, RVEDVI, and RV GLS. Therefore, more attention should be paid to RV myocardial stretching, rather than only focusing on the contraction of RV, when evaluating RV function.Conclusion
SSF-RV-Longitudinal could independently predict the clinical worsening of PAH patients and is a novel parameter to evaluate RV function.Acknowledgements
This study was supported by grants from the National Key Research and Development Program of China (No. 2016YFC1304400) and Youth Foundation of Fuwai Hospital (Grant number: 2022-FWQN06).References
1. Cao J, Li S, Cui L, Zhu K, Huo H, Liu T. Biventricular Myocardial Strain Analysis in Patients with Pulmonary Arterial Hypertension Using Cardiac Magnetic Resonance Tissue-Tracking Technology. J Clin Med. 2022 Apr 15;11(8):2230. doi: 10.3390/jcm11082230.
2. Quan R, Zhang G, Yu Z, et al. Characteristics, goal-oriented treatments and survival of pulmonary arterial hypertension in China: Insights from a national multicentre prospective registry. Respirology. 2022 Jul;27(7):517-528. doi: 10.1111/resp.14247.
3. Schäfer M, Collins KK, Browne LP, et al. Effect of electrical dyssynchrony on left and right ventricular mechanics in children with pulmonary arterial hypertension. J Heart Lung Transplant. 2018 Jul;37(7):870-878.
4. Kirn B, Jansen A, Bracke F, van Gelder B, Arts T, Prinzen FW. Mechanical discoordination rather than dyssynchrony predicts reverse remodeling upon cardiac resynchronization. Am J Physiol Heart Circ Physiol. 2008 Aug;295(2):H640-6. doi: 10.1152/ajpheart.00106.2008.
5. Frank BS, Schäfer M, Douwes JM, et al. Novel measures of left ventricular electromechanical discoordination predict clinical outcomes in children with pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol. 2020 Feb 1;318(2):H401-H412. doi: 10.1152/ajpheart.00355.2019.
Figures
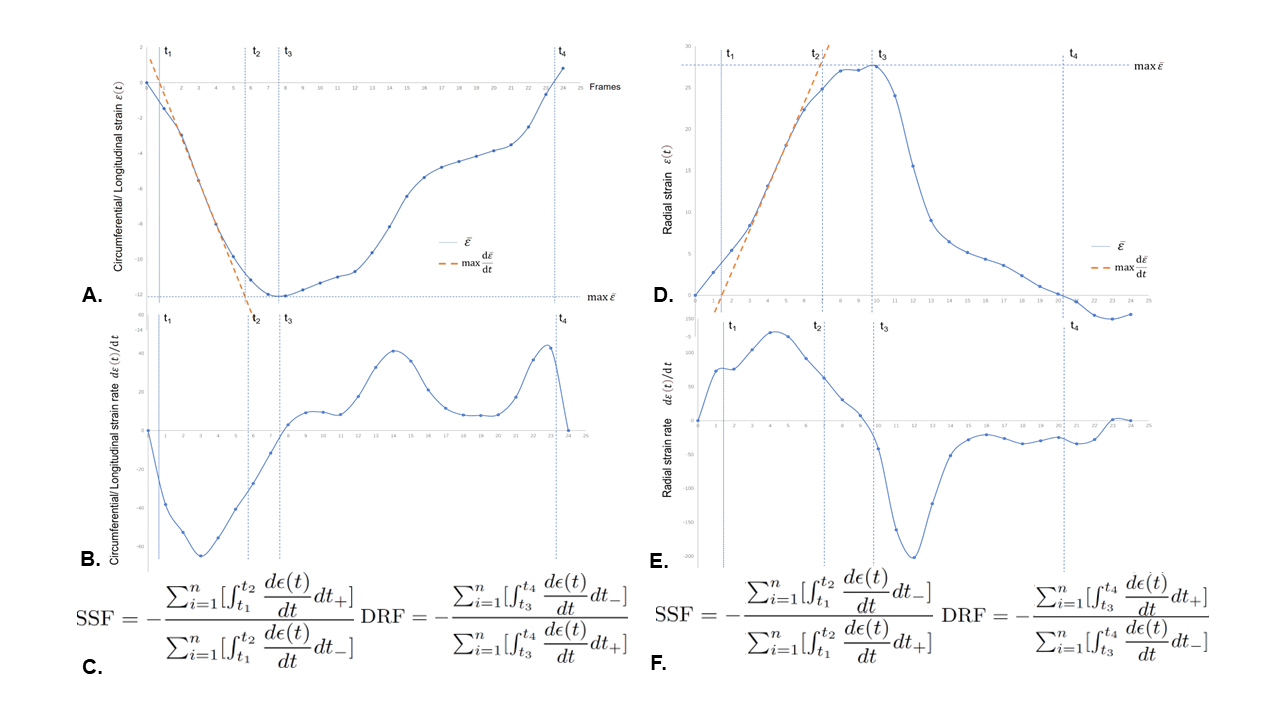
Figure 1. The schematic diagram of the postprocessing algorithm for right ventricular (RV) discoordination indexes.
C showed the algorithms of systolic stretch fraction (SSF) and diastolic relaxation fraction (DRF) in the circumferential, or longitudinal directions. F showed the algorithms of SSF and DRF in the radial directions. The calculations of SSF and DRF required separation of d (t)/dt curves into positive and negative components with subsequent integration and summation of each interval to compute the final ratio.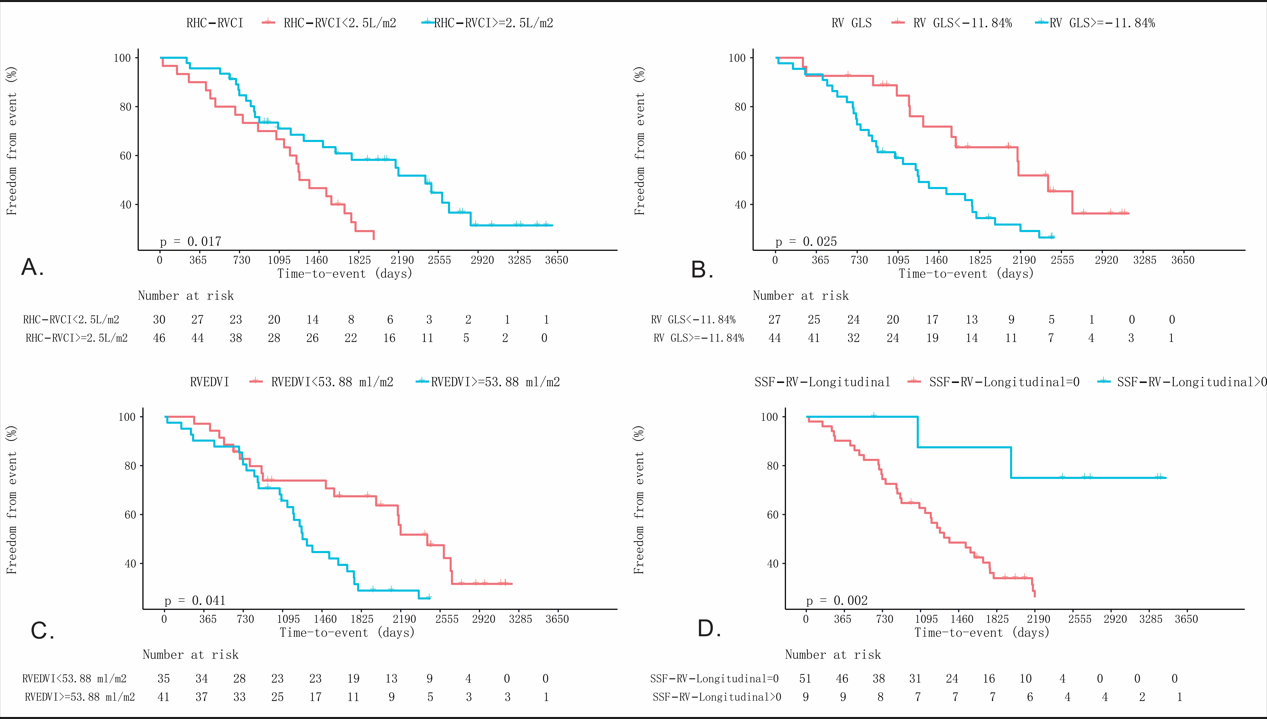
Figure 2. The Kaplan-Meyer curves to predict clinical worsening events of PAH patients.
RHC-RVCI: right heart catherization derived right ventricular cardiac index; GLS: global longitudinal strain; RVEDVI: right ventricular end diastolic volume index.