0588
Validation of in vivo VERDICT fIC against matched histology from whole-mount prostatectomy1Centre for Medical Imaging Computing, University College London, London, United Kingdom, 2Centre for Medical Imaging, University College London, London, United Kingdom, 3Department of Radiology, UCLH, London, United Kingdom, 4Department of Neuroinflammation, University College London, London, United Kingdom, 5Radiomics Group, Vall d'Hebron Institute of Oncology, Barcelona, Spain, 6Division of Surgery and Interventional Sciences, University College London, London, United Kingdom, 7Department of Urology, UCLH, London, United Kingdom, 8Department of Urology, Barts Health NHS Foundation Trust, London, United Kingdom, 9Faculty of the Built Environment, University College London, London, United Kingdom, 10Department of Pathology, University College London Cancer Institute, London, United Kingdom, 11Department of Pathology, UCLH, London, United Kingdom
Synopsis
Keywords: Simulation/Validation, Validation, Prostate cancer diffusion VERDICT
Motivation: Intracellular volume fraction (fIC) maps from VERDICT-MRI have shown potential to improve prostate cancer (PCa) stratification, but the microstructural origin of the signal has not yet been investigated in in vivo settings.
Goal(s): Investigate the accuracy of fIC from in vivo VERDICT-MRI as a measurement of cell density using matched prostatectomy specimens.
Approach: Using personalised moulds from multiparametric (mp)MRI and deep learning image registration, we align whole prostatectomy histology images with corresponding VERDICT MR images. We compare fIC maps against cell density maps derived from histology.
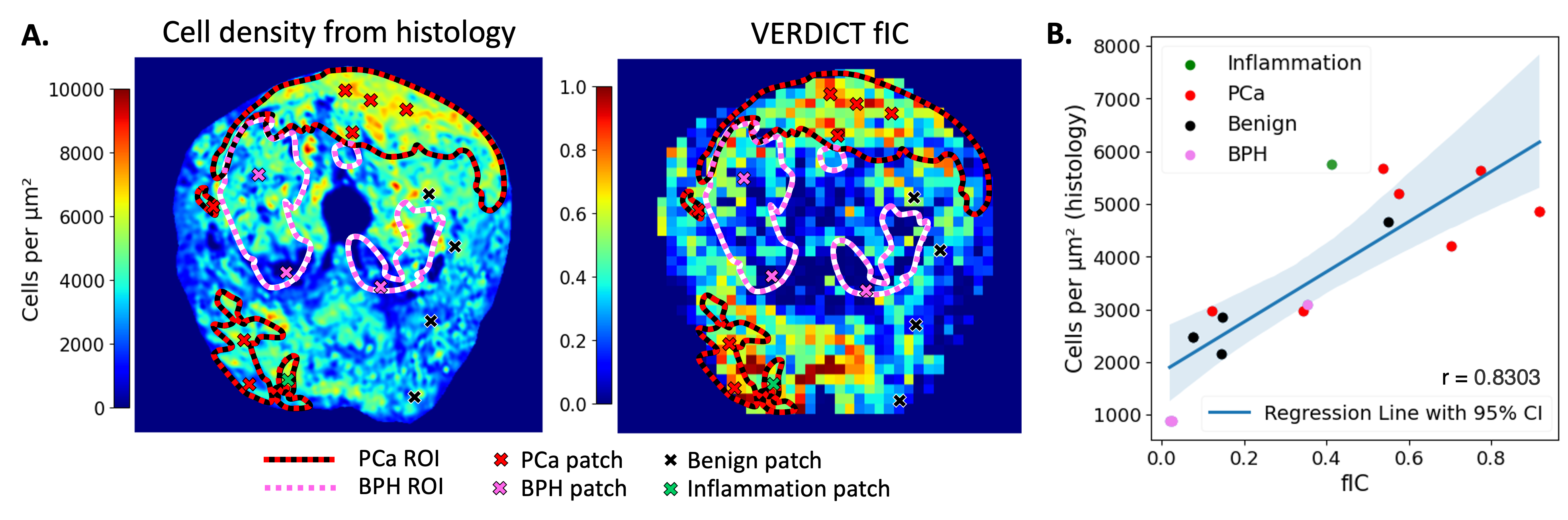
Results: fIC maps show very strong agreement with histology-derived cell density maps of epithelial cells (r=0.8303).
Impact: Our study shows that VERDICT fIC maps are accurate descriptors of epithelial cell density in the prostate. The biological interpretability of these maps will facilitate translation into clinical practice, improving PCa stratification from MRI.
Introduction
Histological analysis is the most accurate way to diagnose prostate cancer (PCa). Multi-parametric MRI (mpMRI) provides a non-invasive alternative, but mpMRI PCa diagnosis shows significant variation across radiologists1 due to the heterogeneous morphology of PCa on MRI and confounding conditions such as benign prostatic hyperplasia (BPH)2, leading to diagnostic errors3,4. Most mpMRI DWI studies use the Apparent Diffusion Coefficient (ADC), which is useful for tumour detection5 but confounds several histological changes like cell density, size, and vascular perfusion effects that can occur in tumours.The Vascular Extracellular and Restricted Diffusion for Cytometry (VERDICT)-MRI framework has a specific DWI protocol with a biophysical tumour model for the diffusion signal6. The intra-cellular volume fraction (fIC) from VERDICT-MRI provides better discrimination of clinically significant (cs) PCa than ADC maps from mpMRI7–9 and better identifies false positive lesions10. Ex vivo validation of VERDICT fIC shows that high fIC zones correspond to high histological cell density11, but in vivo VERDICT validation with accurate registration is lacking.
This study uses personalised 3D-printed prostate moulds and a deep learning registration pipeline to obtain accurate matching of whole-mount prostatectomy slices and in vivo VERDICT-MRI. We aim to validate the fIC maps against cell density maps from prostatectomy histology images.
Methods
Patient data. The study cohort is from the Histo-MRI clinical trial (NCT04792138), which performs mpMRI and VERDICT-MRI on men with clinical PCa suspicion12. MR images are acquired on a 3T scanner (Achieva, Ingenia; Philips Healthcare; Best; The Netherlands). Pre-operative MRI is used to print personalised 3D moulds of the prostate for prostatectomy candidates. The prostate is scanned in the mould (ex vivo MRI) and sectioned following the mould’s guides13, resulting in histology slices with the same spacing and orientation as the MRI.The sample presented corresponds to a 68-year-old White British with lesions graded Likert Score 3 from mpMRI and Gleason Score 3+4 from prostatectomy. Annotations on MRI (T2-weighted from mpMRI and VERDICT fIC) and histology are drawn by experienced radiologists and histopathologists.
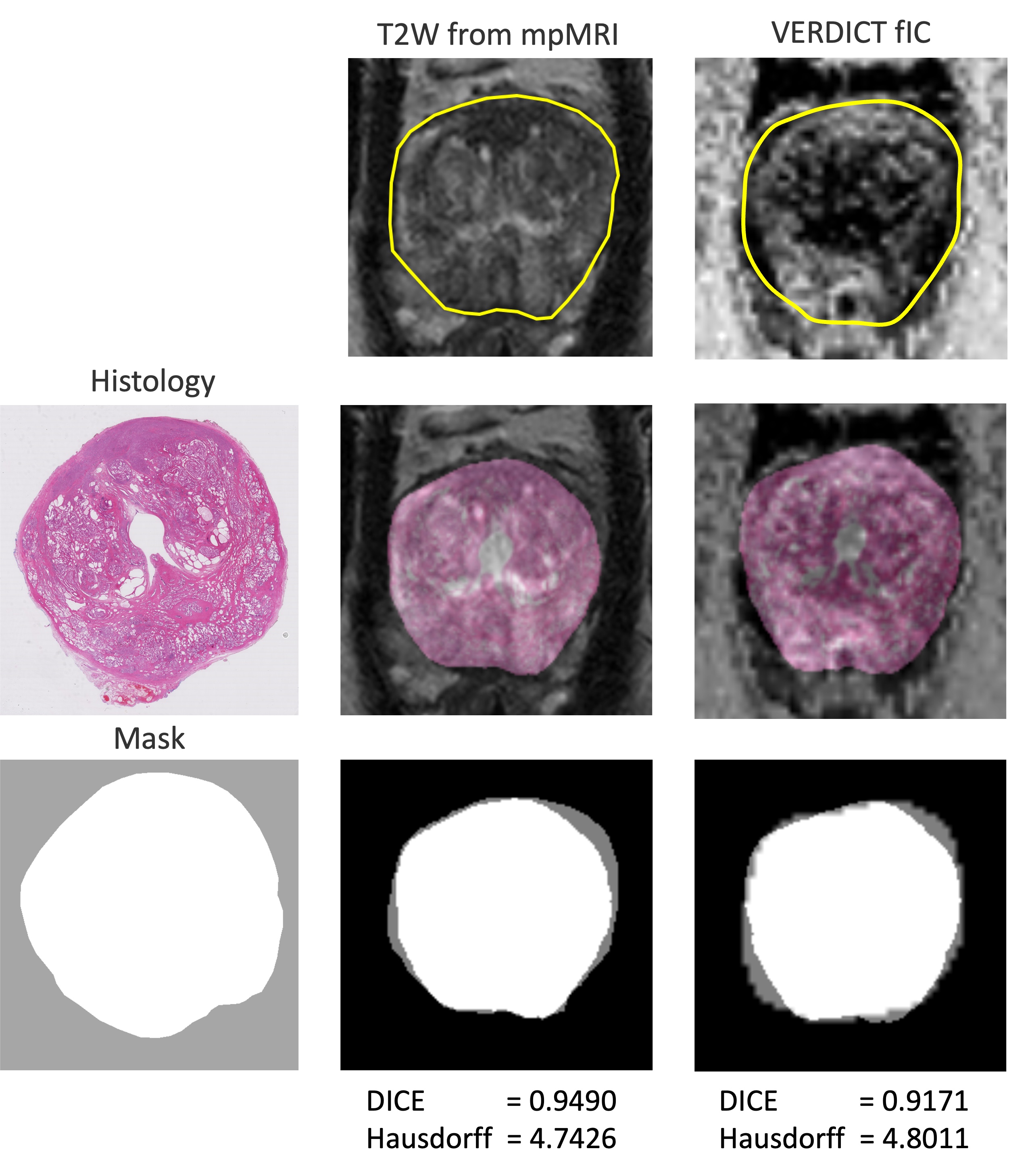
Registration. We extend ProsRegNet14, a deep learning multi-modal registration network, to register histology to DWI. We compare performance of histology to fIC registrations against the default histology to T2-weighted (T2W) registrations using the DICE coefficient and Hausdorff distance of the prostate masks.
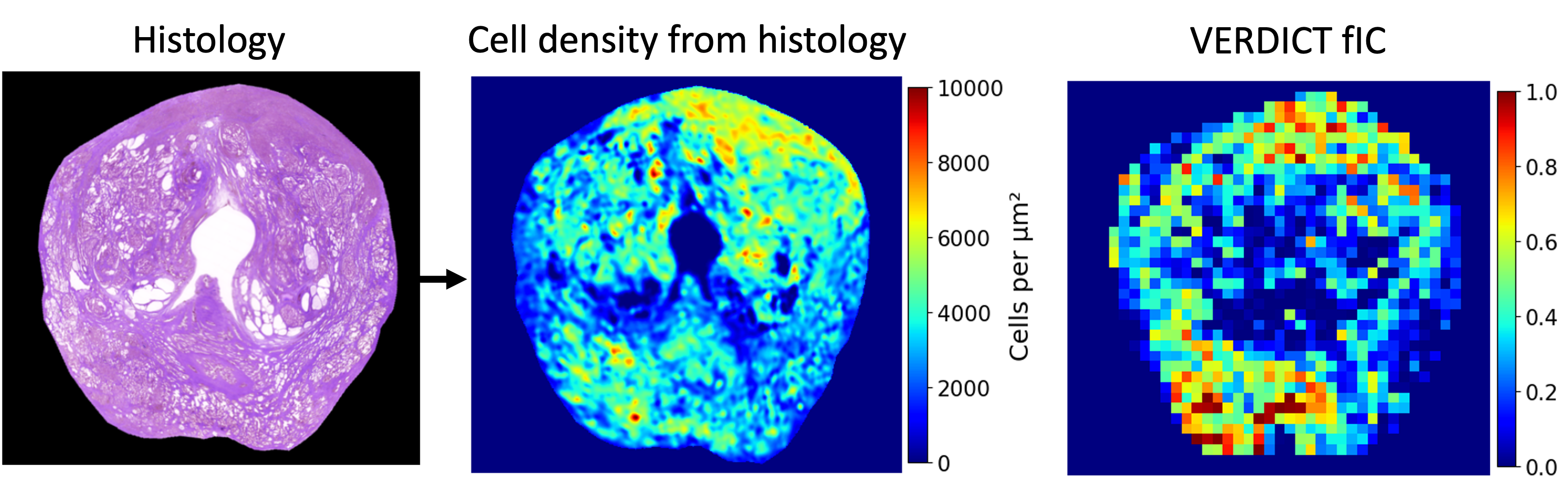
fIC validation. We compare fIC to cell density maps derived from whole-mount histology using a custom pipeline on QuPath15, validated by an expert histopathologist, where each outputted pixel corresponds to a 512-pixel-wide patch from the histology with an area of 0.216μm2. Epithelial and basal cell sizes are calculated from manual segmentations on histology.
Results
Figure 1 shows the ProsRegNet registration performance. There is no significant difference when using fIC maps as target than when using T2W images from mpMRI.Figure 2 illustrates the correspondence between fIC maps and histology cell density maps. High fIC values in cancerous regions correspond to high cell density areas in histology. There is an area with high fIC and medium histology cell density due to an intra-prostatic portion of the ejaculatory duct (on histology). Figure 3 quantifies the correlation between the maps using 15 ROIs throughout the prostate (r=0.8303). Areas of BPH do not show high fIC values.
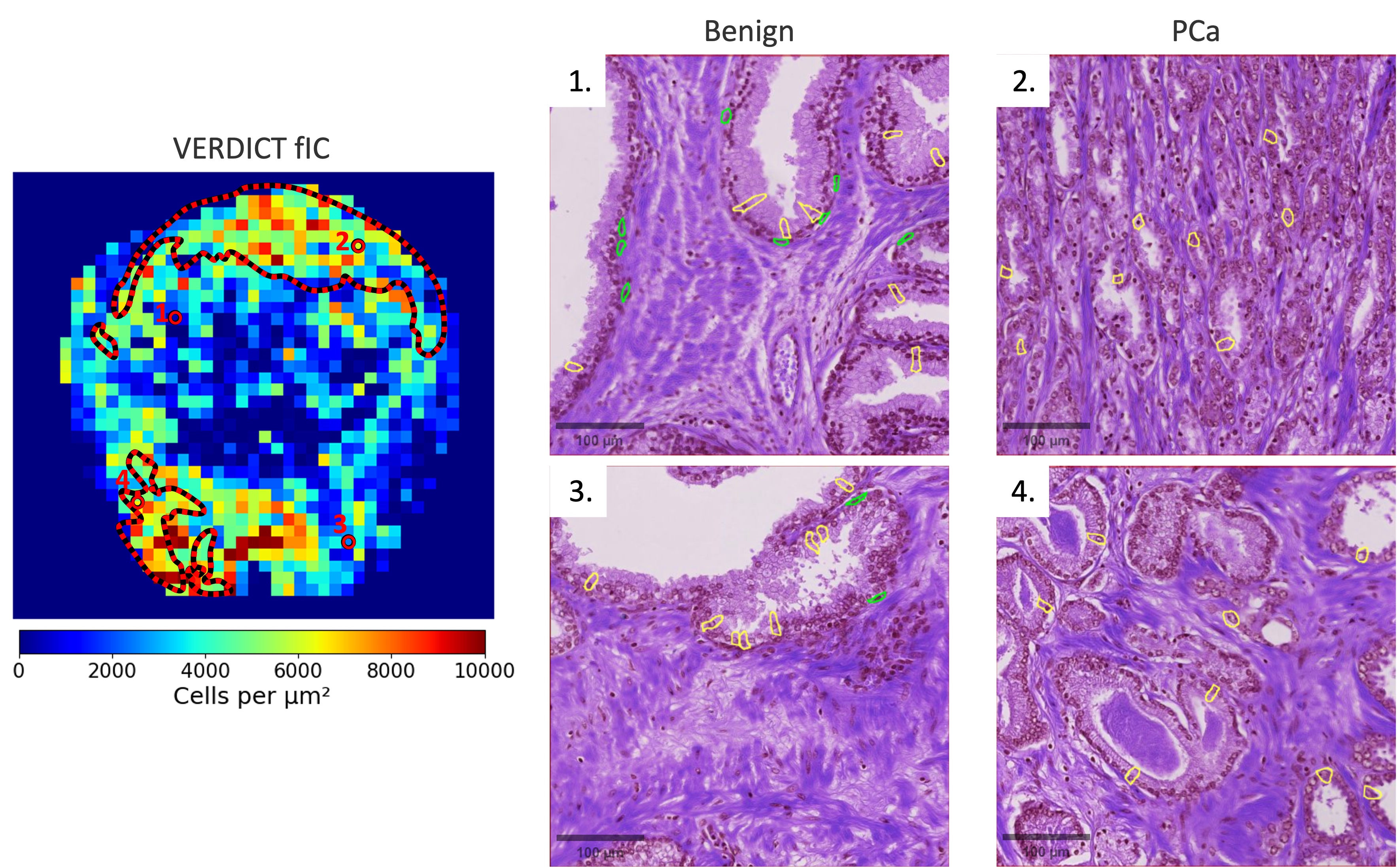
Figure 4 presents the VERDICT fIC map alongside two benign and two PCa histology ROIs, showing high epithelial cell density in areas of high fIC. Basal cells surrounding epithelial cells in benign tissue do not appear in PCa patches, while there is characteristic proliferation of epithelial cells in PCa regions16.
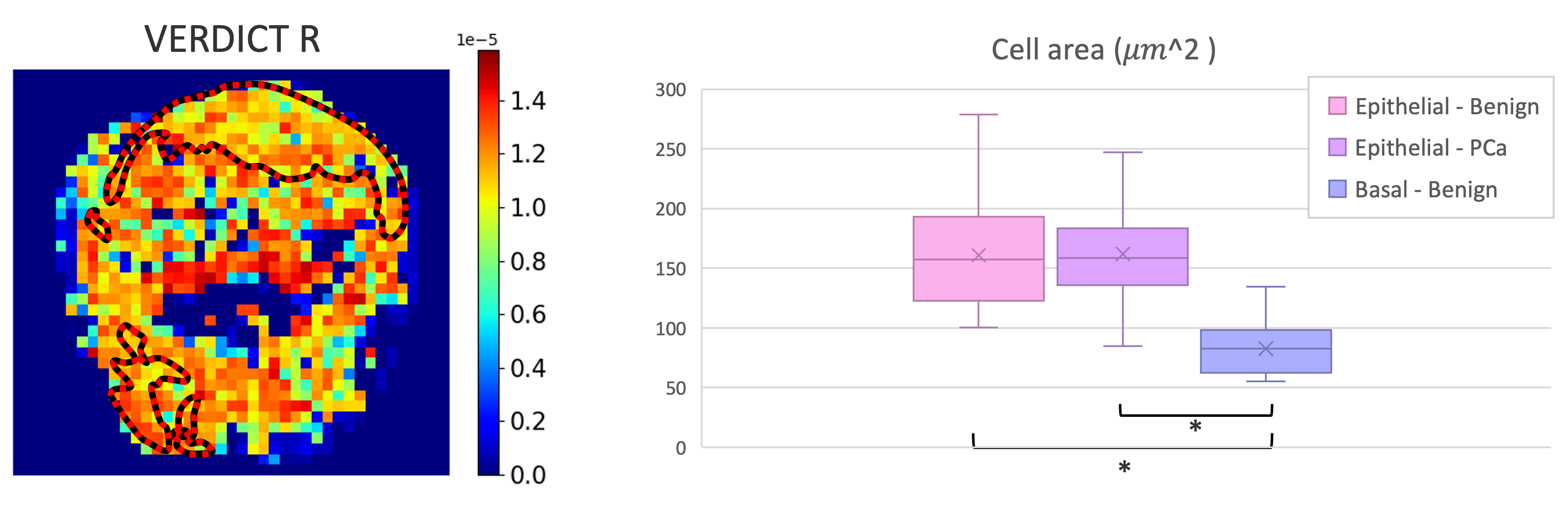
The VERDICT radius (R) map (Figure 5) shows little spatial variation (11-14μm). This matches the histological cell size analysis (boxplot), where we find no significant difference in epithelial cell size in benign and PCa regions. Epithelial cells are significantly larger than basal cells.
Discussion and Conclusion
This work presents an in vivo validation of VERDICT-MRI fIC maps, showing excellent agreement with histological analysis of whole-mount prostatectomy.We adapt ProsRegNet to accurately align histology with fIC maps and demonstrate comparable performance to registrations against T2W images. Histological analysis shows that epithelial cell size does not change with PCa and that only epithelial cells proliferate in areas of high fIC, confirming that high fIC values are due to high epithelial cell density. In our results, pathologies that mimic cancer, like BPH, do not have high fIC, suggesting the ability of fIC maps to further improve tissue characterization.
This validation of VERDICT fIC maps can accelerate the incorporation of VERDICT-MRI into clinical practice, potentially reducing unnecessary biopsies8. Future work will analyse more samples for statistical analysis.
Acknowledgements
This work is supported by the EPSRC-funded UCL Centre for Doctoral Training in Intelligent, Integrated Imaging in Healthcare (i4health) [EP/S021930/1]; EPSRC grant numbers EP/N021967/1, EP/R006032/1; Prostate Cancer UK, Targeted Call 2014, Translational Research St.2, grant number PG14-018-TR2; the National Institute for Health and Care Research, University College London Hospitals Biomedical Research Centre; and Cancer Research UK National Cancer Imaging Translational Accelerator.References
1. Ahmed, H. U. et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. The Lancet 389, 815–822 (2017).
2. Lovegrove, C. E. et al. Prostate imaging features that indicate benign or Malignant pathology on biopsy. Translational Andrology and Urology vol. 7 S420–S435 Preprint at https://doi.org/10.21037/tau.2018.07.06 (2018).
3. Rosenkrantz, A. B. et al. Interobserver reproducibility of the PI-RADS version 2 lexicon: A multicenter study of six experienced prostate radiologists. Radiology 280, 793–804 (2016).
4. Westphalen, A. C. et al. Variability of the positive predictive value of PI-RADS for prostate MRI across 26 centers: Experience of the society of abdominal radiology prostate cancer disease-focused panel. Radiology 296, 76–84 (2020).
5. Wu, X. et al. Correlation between apparent diffusion coefficient value on diffusion-weighted MR imaging and Gleason score in prostate cancer. Diagn Interv Imaging 98, 63–71 (2017).
6. Panagiotaki, E. et al. Noninvasive quantification of solid tumor microstructure using VERDICT MRI. Cancer Res 74, 1902–1912 (2014).
7. Johnston, E. W. et al. VERDICT MRI for prostate cancer: Intracellular volume fraction versus apparent diffusion coefficient. Radiology 291, 391–397 (2019).
8. Singh, S. et al. Avoiding Unnecessary Biopsy after Multiparametric Prostate MRI with VERDICT Analysis: The INNOVATE Study. Radiology (2022) doi:10.1148/radiol.212536.
9. Appayya, M. B. et al. The intracellular component of VERDICT (Vascular, Extracellular, and Restricted Diffusion for Cytometry in Tumors) MRI distinguishes Gleason 4 pattern better than Apparent Diffusion Coefficient. (2018).
10. Sen, S. et al. Differentiating False Positive Lesions from Clinically Significant Cancer and Normal Prostate Tissue Using VERDICT MRI and Other Diffusion Models. Diagnostics 12, (2022).
11. Bailey, C. et al. VERDICT MRI validation in fresh and fixed prostate specimens using patient-specific moulds for histological and MR alignment. NMR Biomed 32, (2019).
12. Singh, S. et al. Histo-MRI map study protocol: a prospective cohort study mapping MRI to histology for biomarker validation and prediction of prostate cancer. BMJ Open 12, e059847 (2022).
13. Bourne, R. M. et al. Apparatus for histological validation of in vivo and ex vivo magnetic resonance imaging of the human prostate. Front Oncol 7, (2017).
14. Shao, W. et al. ProsRegNet: A Deep Learning Framework for Registration of MRI and Histopathology Images of the Prostate. (2020).
15. Bankhead, P. et al. QuPath: Open source software for digital pathology image analysis. Sci Rep 7, (2017).
16. Humphrey, P. A. Histopathology of prostate cancer. Cold Spring Harb Perspect Med 7, (2017).
Figures