0582
High-resolution free-breathing simultaneous myocardial T1, T2 and T1ρ mapping with region-optimized virtual coils (ROVir)1School of Biomedical Engineering, ShanghaiTech University, Shanghai, China, 2Shanghai Clinical Research and Trial Center, Shanghai, China, 3Department of Cardiovascular Medicine, Ruijin Hospital Lu Wan Branch, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Synopsis
Keywords: Myocardium, Cardiomyopathy, Quantitative Imaging
Motivation: Cardiac parametric mapping with electrocardiogram-triggered single-shot acquisition has compromised spatial resolution due to limited quiescent period for data acquisition.
Goal(s): To develop a high-resolution simultaneous myocardial T1, T2 and T1ρ mapping technique.
Approach: Enhance the spatial resolution while reducing the FOV to make the acquisition window fit in the mid-diastolic quiescent period in the cardiac cycle. Subsequently, employ the ROVir technique to eliminate fold-over artifacts arising from FOV reduction.
Results: The proposed technique achieved high-resolution multi-parametric mapping without a loss of quantitative precision.
Impact: A novel framework was proposed to shorten the acquisition window and improve the spatial resolution of electrocardiogram-triggered cardiac parametric mapping beyond common k-space undersamping. High-resolution myocardial parametric mapping can provide more precise and reliable diagnostic information.
Introduction
Parametric mapping has emerged as a promising non-invasive tool for diagnosing various myocardial diseases1, 2. The combination of multiple parameters can enhance diagnostic sensitivity and confidence for suspected cardiomyopathy, as these parameters offer complementary insights into the myocardium3. Recently, we proposed a free-breathing multi-parametric mapping (FB-MultiMap) technique employing Cartesian sampling and dictionary matching, allowing for the acquisition of co-registered T1, T2 and T1ρ parameter maps in a single scan4. However, current cardiac mapping techniques commonly adopt electrocardiogram-triggered single-shot diastolic acquisition to minimize the influence of cardiac motion, leading to compromised spatial resolution due to the limited quiescent period of ~200ms. For high-spatial-resolution cardiac parametric mapping, an alternative way to k-space undersampling would be to restrict the phase-encoding (PE) FOV to only include the heart. Although this can effectively reduce the number of k-space phase-encoding lines, reduced FOV would introduce fold-over artifacts to the cardiac region. The region-optimized virtual coils (ROVir) technique is a specialized coil compression technique, exhibiting the ability to selectively preserve the signal from the user-specified Region of Interest (ROI), while suppressing the signal energy from undesired spatial regions5. It has been successfully applied for cardiac cine imaging acceleration6. In this study, we explored the feasibility of improving the spatial resolution of FB-MultiMap by reducing the PE FOV and employing ROVir reconstruction to eliminate aliasing artifacts.Methods
FB-MultiMap with ROVirThe FB-Multimap technique employs electrocardiogram-triggered single-shot Cartesian acquisition over 16 consecutive cardiac cycles4 (Fig.1A). In this study, we aimed to improve the spatial resolution of FB-MultiMap while reduced the PE FOV to restrict the acquisition window to an appropriate range of ~220 ms. Subsequently, ROVir was employed to eliminate aliasing artifacts by selecting the initial few virtual coils that mainly contain signal energy from the heart. The framework of combining ROVir with high-resolution FB-MultiMap is shown in Fig.1B. Apart from acquiring high-resolution images with reduced FOV (HR+reduceFOV), a single-shot acquisition with FOV encompassing the entire torso was performed as a calibration scan, which was used for delineating the target and exclusion regions (Fig.2). Then, the optimal ROVir linear mixing weights were calculated, based on which the optimal ROVir virtual coils were formed and subsequently arranged in accordance with their eigenvalues6. The top-5 virtual coils were retained to generate artifacts-free images and the parameter maps were extracted by the dictionary matching as in FB-MultiMap.
Imaging experiments
The proposed high-resolution FB-MultiMap technique was tested in one healthy subject after IRB approval and obtaining written informed consent. The MRI experiment was performed on a 3.0T scanner with 36-channel coils. All scans were performed during free-breathing and with the same imaging position. As a reference for comparison, a FB-MultiMap scan with traditional resolution and full FOV (fullFOV) were performed. Prior to the HR+reduceFOV imaging of FB-MultiMap, a calibration scan was performed with the same FOV and resolution as the fullFOV scan. The imaging parameters including FOV and spatial resolution are summarized in Table.1.
Results & Discussion
Fig.3 illustrates the images obtained through direct coil-combination and ROVir coil-combination. The signal of the interference regions was suppressed by ROVir in both the calibration and fullFOV images (Fig.3A, B). Significant aliasing artifacts can be observed in the HR+reduceFOV FB-MultiMap images reconstructed by direct coil-combination, whereas the artifacts were effectively suppressed after using ROVir (Fig.3C). Importantly, ROVir does not affect the contrast evolutions of FB-MultiMap, as evident by the similar parametric maps acquired using the fullFOV and HR+reduceFOV techniques in Fig.4. However, it is noted that there is an obvious straight line artifact in the left ventricle blood pool of the HR+reduceFOV parametric maps, potentially caused by the residual fold-over artifacts or undersampling aliasing. The measurements obtained with fullFOV and HR+reduceFOV techniques are in close agreement (T1: 1164±41ms vs. 1178±42ms; T2: 43.4±6.4ms vs. 42.4±3.2ms; T1ρ: 45.9±4.4ms vs. 44.2±4.5ms). A magnified view of the interventricular septum (Fig.4) reveals sharper boundaries in the HR+reduceFOV parameter maps.Conclusion
We demonstrated the feasibility of combining FB-MultiMap and ROVir for high-resolution simultaneous myocardial T1, T2 and T1ρ mapping. Subsequent investigations will focus on improving the image quality and validating the proposed technique in more subjects.Acknowledgements
No acknowledgement found.References
1. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson. 2017;19(1):75.
2. Qi H, Bustin A, Kuestner T, Hajhosseiny R, Cruz G, Kunze K, et al. Respiratory motion-compensated high-resolution 3D whole-heart T1ρ mapping. J Cardiovasc Magn Reson. 2020;22(1):12.
3. Warnica W, Al-Arnawoot A, Stanimirovic A, Thavendiranathan P, Wald RM, Pakkal M, et al. Clinical Impact of Cardiac MRI T1 and T2 Parametric Mapping in Patients with Suspected Cardiomyopathy. Radiology. 2022;305(2):319-26.
4. Lyu Z, Hua S, Xu J, Shen Y, Guo R, Hu P, Qi H. Free-Breathing Simultaneous Native Myocardial T1, T2 and T1ρ Mapping with Cartesian Acquisition and Dictionary Matching. J Cardiovasc Magn Reson. in press.
5. Kim D, Cauley SF, Nayak KS, Leahy RM, Haldar JP. Region-optimized virtual (ROVir) coils: Localization and/or suppression of spatial regions using sensor-domain beamforming. Magn Reson Med. 2021;86(1):197-212.
6. Kim D, Coll-Font J, Lobos RA, Stab D, Pang J, Foster A, et al. Single breath-hold CINE imaging with combined simultaneous multislice and region-optimized virtual coils. Magn Reson Med. 2023;90(1):222-30.
Figures
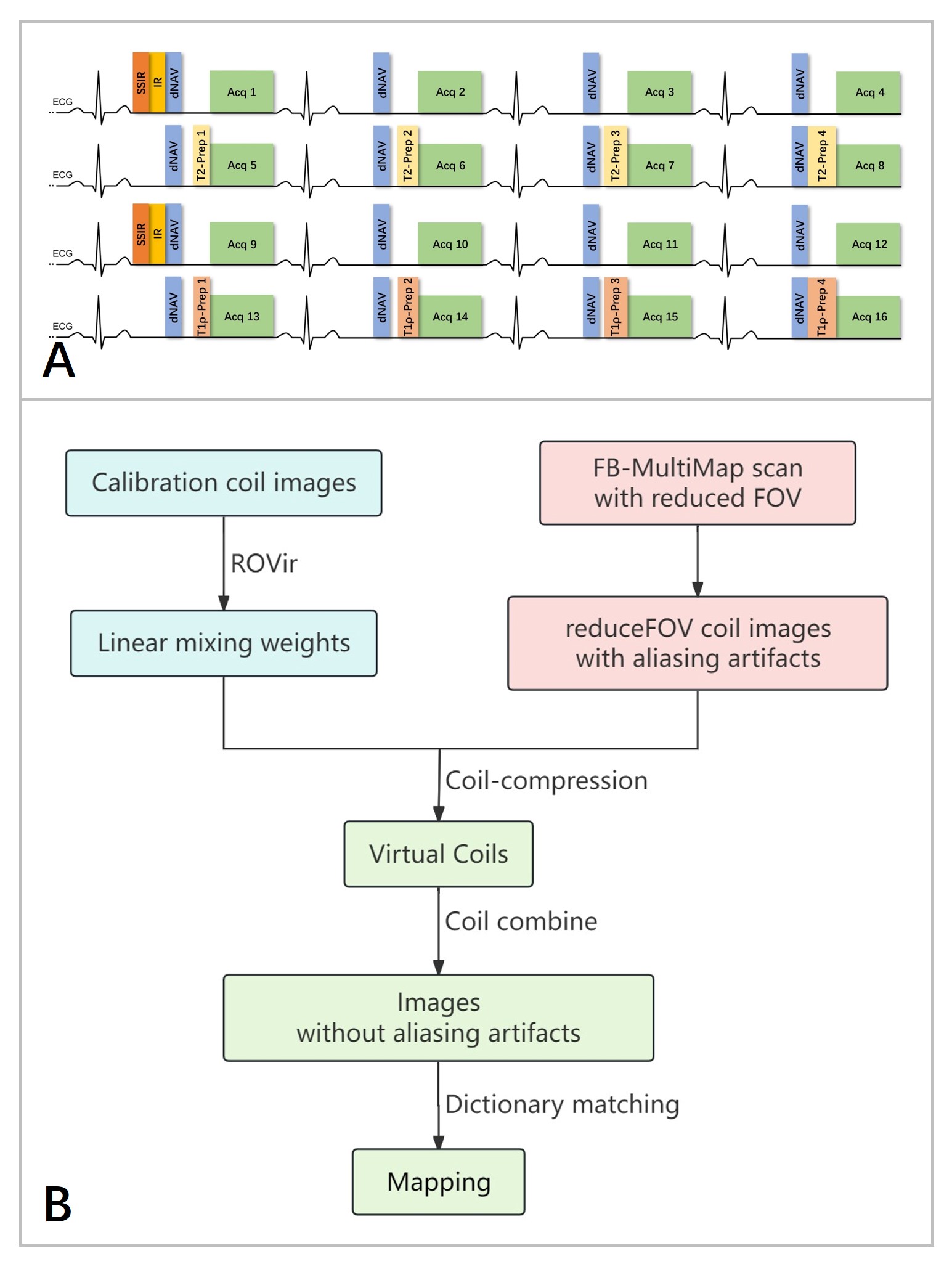
Fig.1 (A) The sequence diagram of FB-MultiMap. (B) Flowchart of the proposed high-resolution multi-parametric mapping technique combining FB-MultiMap and ROVir with a reduced FOV acquisition.
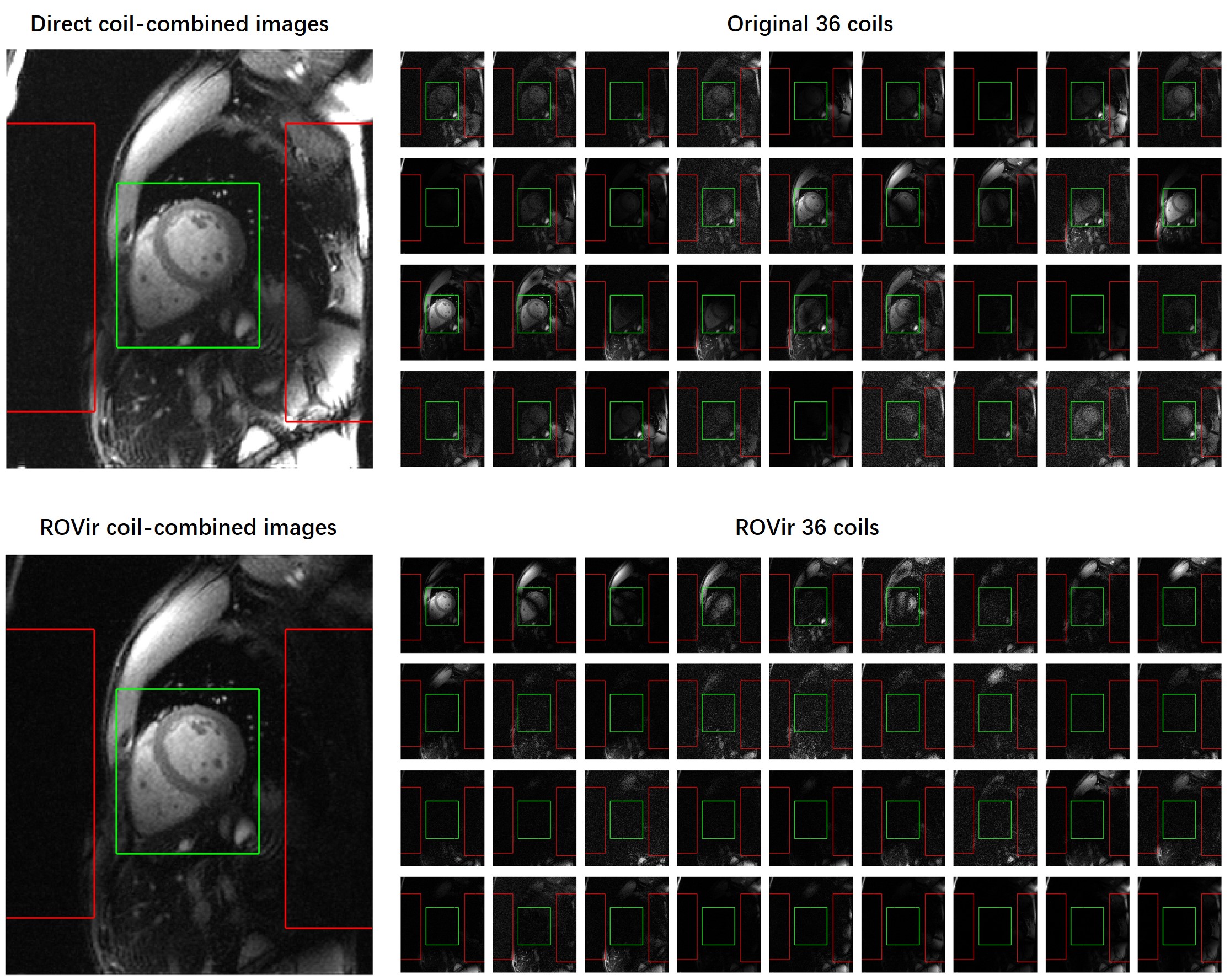
Fig.2 Illustration of applying ROVir to the full FOV images. The target and interference regions for ROVir are contoured by green and red boxes, respectively.
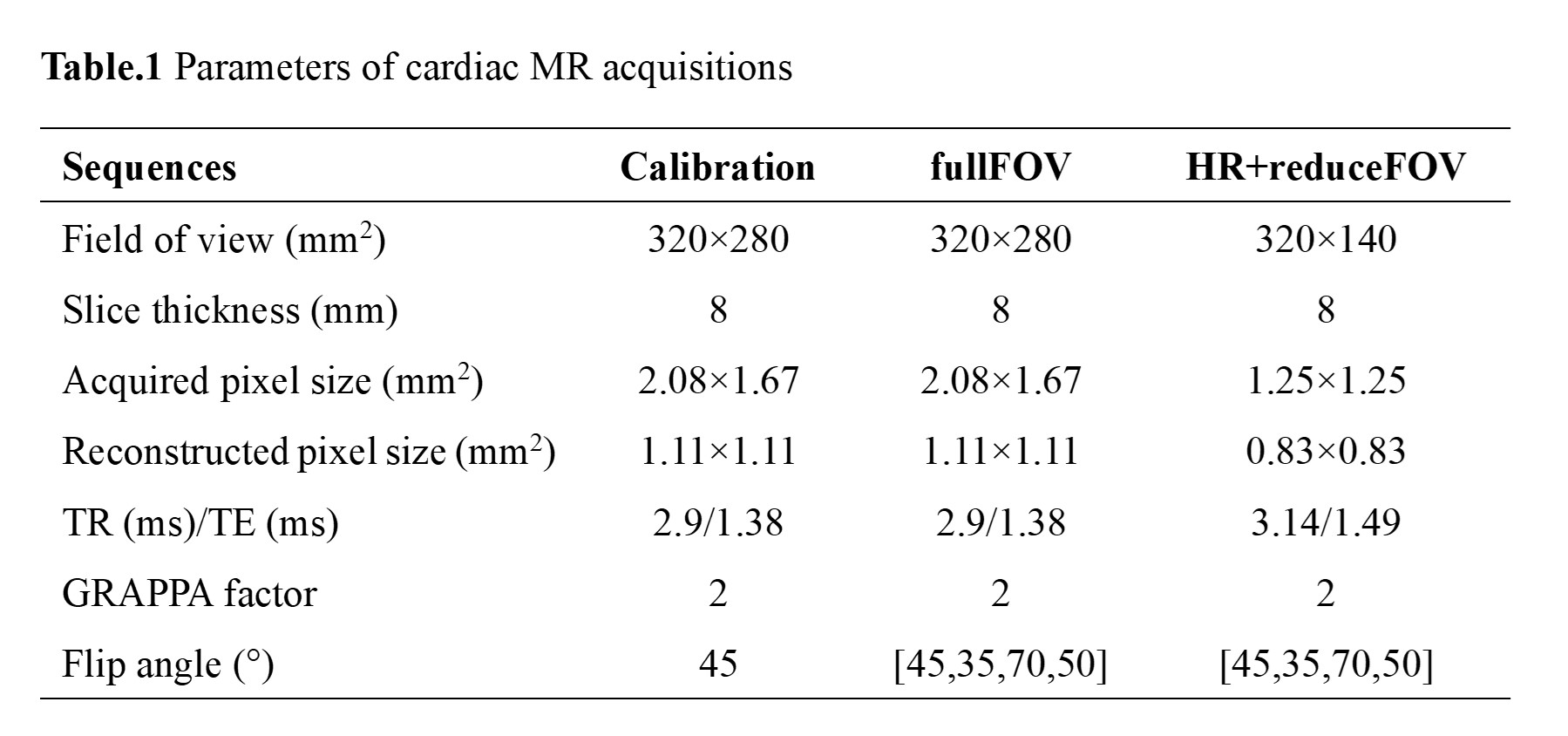
Table.1 Parameters of cardiac MR acquisitions
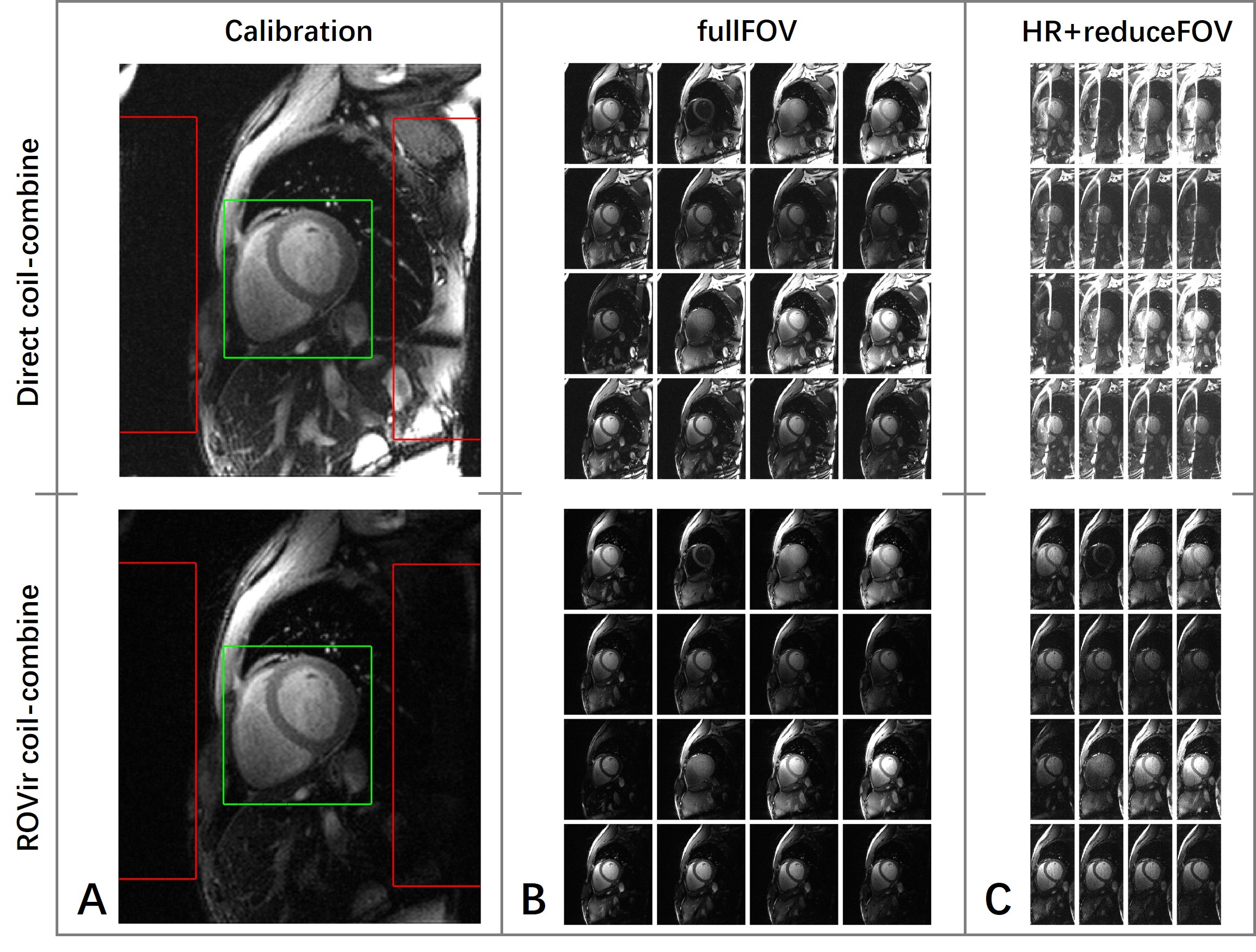
Fig.3 Illustration of applying different coil-combination methods on calibration image (A), FB-MultiMap with conventional spatial resolution and full FOV (B) and FB-MultiMap with high spatial resolution and reduced FOV (C).
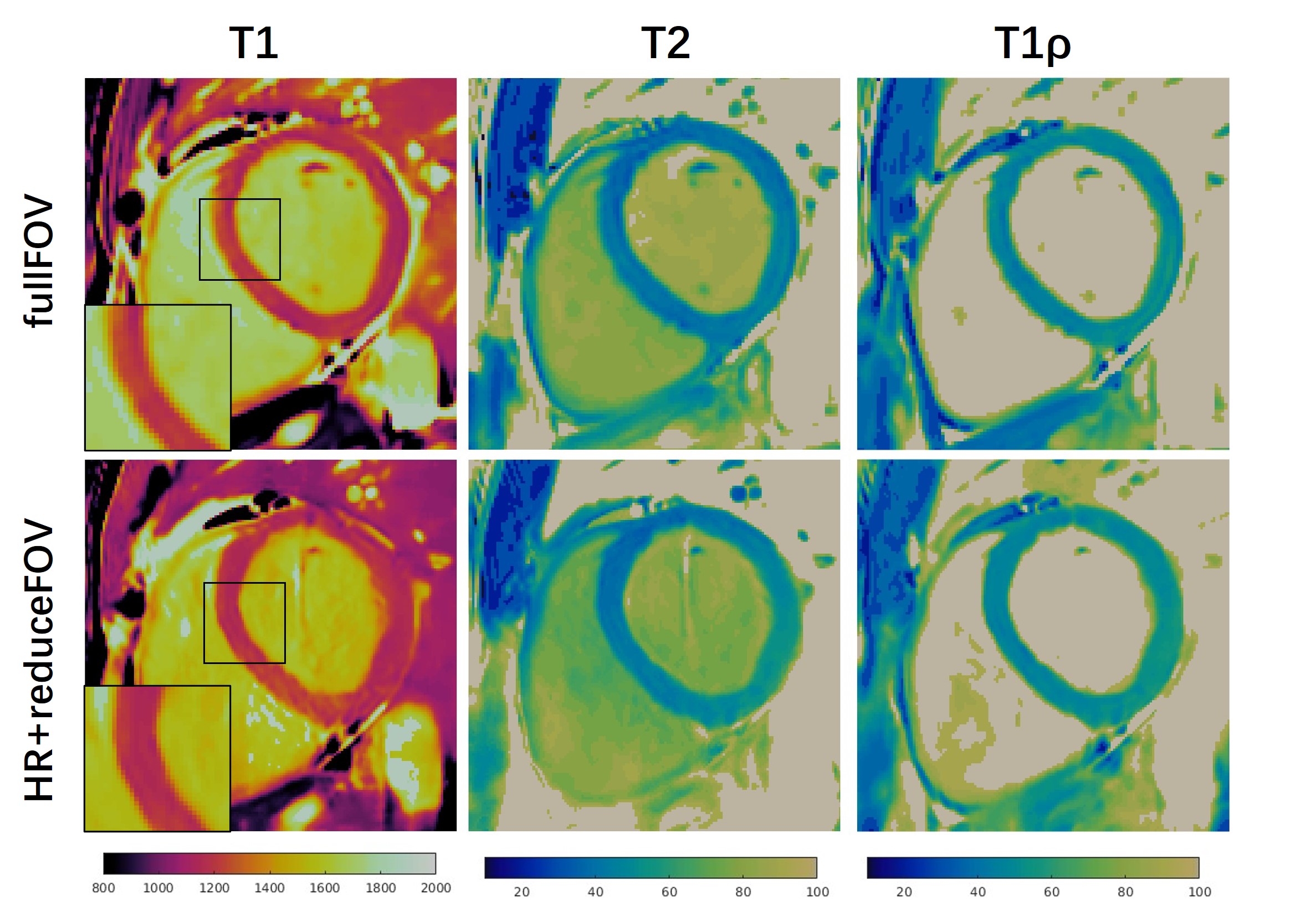
Fig.4 FB-MultiMap parametric maps measured using conventional spatial resolution with full FOV (first row), and high spatial resolution with reduced FOV (second row).