0569
Optimizing MR Fingerprinting Pulse Sequences for Neonates and Across Age Ranges1Case Western Reserve University, Cleveland, OH, United States
Synopsis
Keywords: Pulse Sequence Design, MR Fingerprinting
Motivation: Due to significantly different relaxation times and image contrasts between neonate and adult brain, MR sequences optimized for adults are sub-optimal and may produce measurement bias in pediatric scans.
Goal(s): Optimizing MR fingerprinting pulse sequence for neuroimaging across age ranges.
Approach: We predicted and minimized measurement errors using the systematic error index model with a digital neonate brain phantom to optimize MRF sequence parameters. Optimized sequences were compared against an adult-optimized sequence via simulation and in vivo scans.
Results: Optimized sequences showed improved image quality and accuracy for infant scans and maintained accuracy for adult scans in both simulation and in vivo experiments.
Impact: We present the first application of the systematic error index model for MRF sequence optimization for brain scans across age ranges to achieve high measurement accuracy with reduced scan time.
Introduction
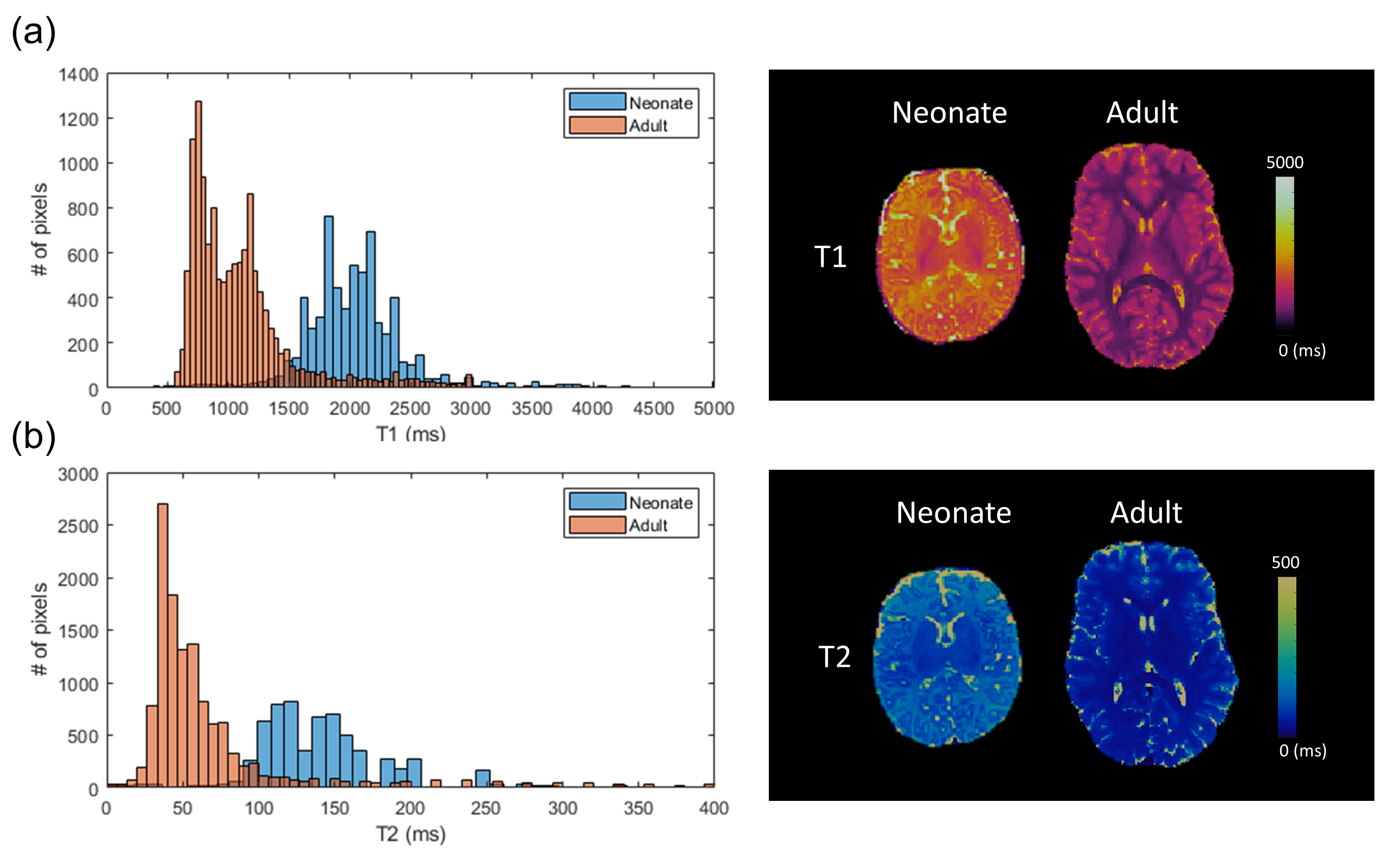
Although optimal pulse sequence design of MR fingerprinting (MRF)1 has been widely investigated for adult brain, there is no optimization framework targeting pediatric patients to date. T1 and T2 values in infant brains are substantially higher, and the contrast between gray matter (GM) and white matter (WM) are drastically different from adults (Figure 1a-b). MRF sequences optimized specifically for T1 and T2 ranges of adult brains could yield reduced sensitivity to higher T1 and T2 values, thus leading to measurement errors in pediatric scans.Here, we propose applying the systematic error index (SEI) model2 to optimize pulse sequences for MRF scans with two goals: design 1) a general MRF sequence that can be used for both infants and adults and 2) an MRF sequence specifically for infants with further scan acceleration. We show that the optimized MRF scans could produce accurate and robust T1 and T2 measurements for neonates and adults in simulation and in vivo experiments.
Methods
Sequence OptimizationCost function: We aim to optimize the flip angle and TR train of MRF-FISP3 sequence. The cost function was constructed as the total scan duration of MRF sequence multiplied by the sum of percentage errors on the resulting T1 and T2 maps. In actual MRF scans, errors mainly come from undersampling and background phase variation due to system imperfections during acquisition. Here, these confounding factors and errors were simulated via SEI model. The ground truth T1 and T2 maps were generated based on segmented numerical brain phantoms. For goal 1, both adult4 and neonate5 phantoms were input into the cost function, whereas only the neonate phantom was the input for goal 2.
Optimization: We optimize MRF sequences with 480 time points for goal 1 and sequences of 240 time points for goal 2. For each goal, 500 optimization trials were initiated from random seeds and carried out by simulated annealing method6 to find the global minimum.
Validation
The MRF sequence optimized for adult (Adult-opt) by Jordan et al7, goal 1 (Neonate-opt1), and goal 2 (Neonate-opt2) was evaluated in simulation using brain phantoms and in vivo experiments. All simulations were performed by generating time-resolved MRF images with undersampling artifacts and phase variations via the partially separable approach8, followed by dictionary matching to obtain tissue property maps. Mean absolute errors were calculated for T1 and T2. All in vivo scans were performed using a Siemens 3T Vida scanner. MRF scans were acquired using stack-of-spiral trajectories with undersampling factors of 48 in-plane and 3 through-plane. Matrix size was 256x256x144 with image resolution of 1.2x1.2x1 mm3 for adults, and 1mm3 isotropic for neonates. All MRF scans were reconstructed with iterative low-rank method9, where the MRF datasets acquired with 240 time points were further processed with locally low-rank reconstruction10.
Results
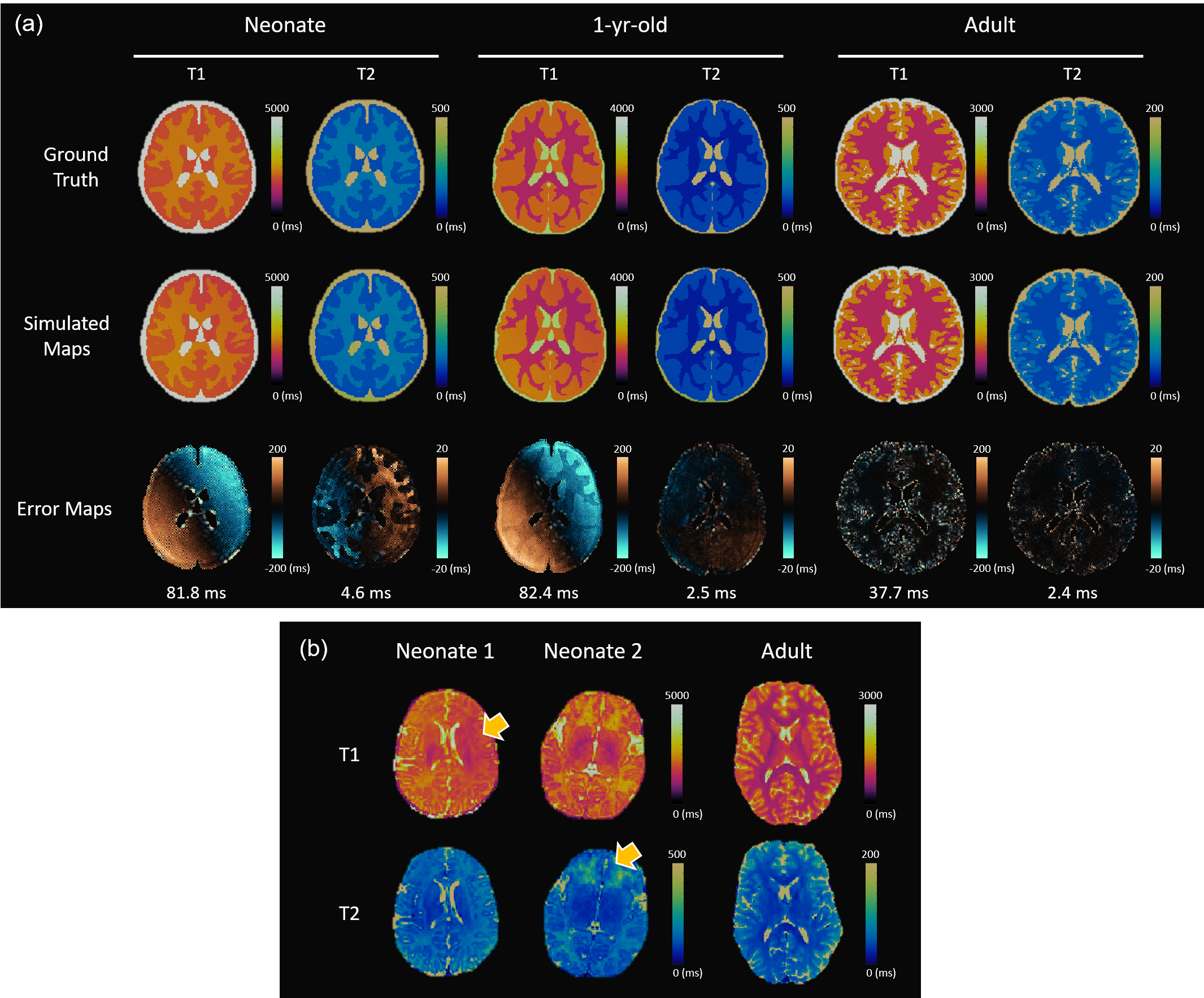
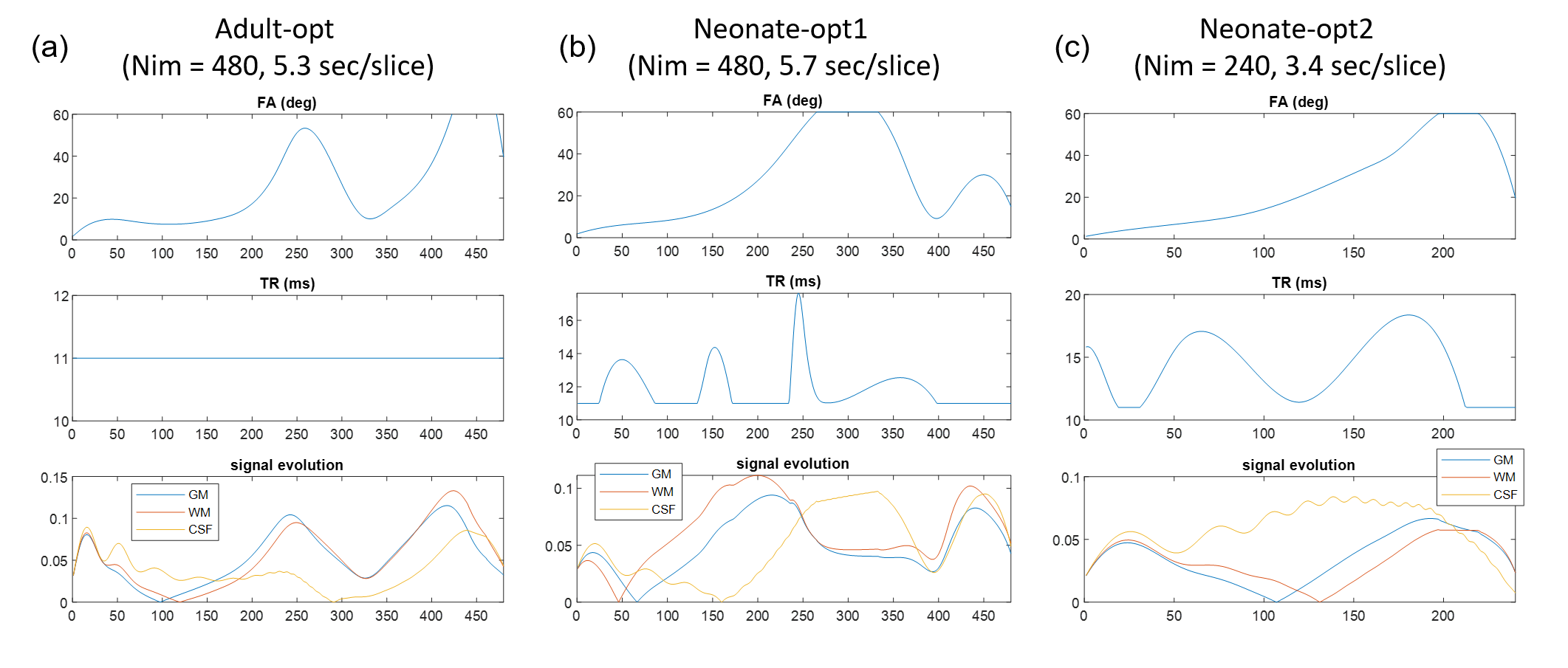
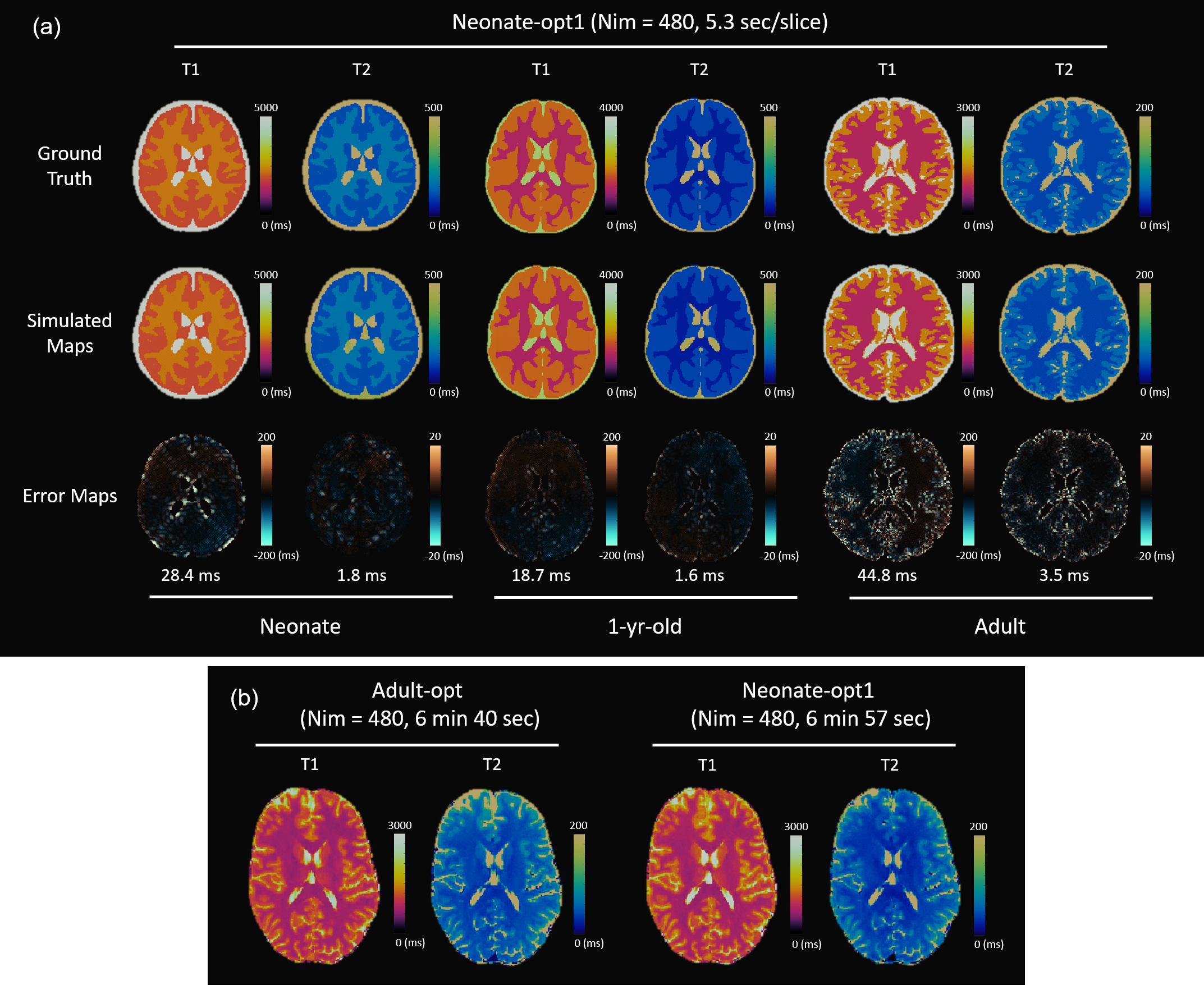
Figure 2a shows the simulation results of Adult-opt using the neonate, 1-year-old baby5, and adult brain phantoms. While measurement errors on adult MRF maps were minimal, MRF maps of neonate and 1-year-old baby were subject to apparent shading artifacts, especially for T1 map. Shading artifacts can be seen on in vivo MRF maps of two neonate scans as well (Figure 2b), as shown by yellow arrows.Figure 3 shows patterns of flip angle and TR and signal evolutions from three neonatal tissues (GM, WM and CSF) for Adult-opt, Neonate-opt1, and Neonate-opt2. In Figure 4a, Neonate-opt1 yielded less shading and reduced errors for both neonate and 1-year-old baby in the simulation. As a tradeoff, errors on adult MRF maps became slightly higher. However, in vivo MRF maps of adults are artifact-free (Figure 4b).
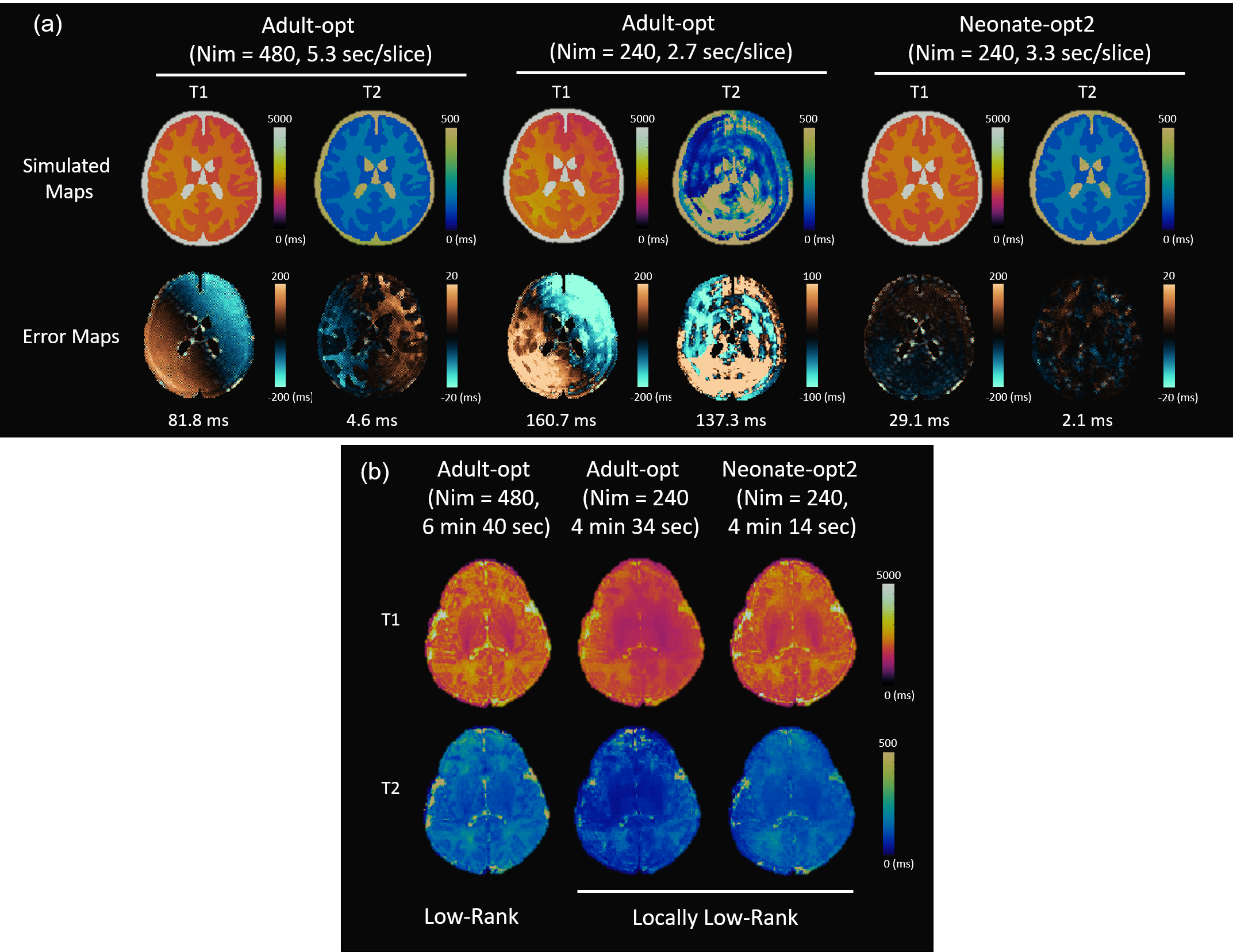
Figure 5a compares the simulated MRF maps of neonates using Neonate-opt2 and Adult-opt. Directly truncating Adult-opt to 240 time points leads to severe shading on T1 map and aliasing artifacts on T2 map. In comparison, Neonate-opt2 of 240 time points obtain much higher measurement accuracy. In in vivo scans of a newborn infant (Figure 5b), MRF maps obtained from Adult-opt with 240 time points show similar shading and aliasing artifacts with simulation results, where the Neonate-opt2 scan was immune to such bias. Neonate-opt2 suffered from low SNR due to high undersampling factors, and image quality can be improved with locally low-rank reconstruction. However, measurement bias from the truncated Adult-opt cannot be suppressed after advanced reconstructions.
Conclusions
We apply the SEI to optimize MRF sequence designs for neuroimaging across age ranges. The optimized MRF scans could achieve high mapping accuracy for both infants and adult, or specifically for infants at shorter scan time. The optimizer can be adapted to design MRF sequences for other clinical applications.Acknowledgements
The authors would like to acknowledge funding from Siemens Healthineers and NIH grants EB026764-01, EB029658-02, and NS109439-01.References
1. Ma D, Gulani V, Seiberlich N, et al. Magnetic Resonance Fingerprinting. Nature. 2013;495(7440):187-192.
2. Hu S, McGivney DF, Qiu Z, Ma D. Characterizing Artifacts in Multi-dimensional MR Fingerprinting with High Efficiency for Sequence Optimization: Systematic Error Index. In: The 31st Annual Meeting, International Society of Magnetic Resonance in Medicine. ; 2023.
3. Jiang Y, Ma D, Seiberlich N, Gulani V, Griswold MA. MR fingerprinting using fast imaging with steady state precession (FISP) with spiral readout. Magn Reson Med. 2015;74(6):1621-1631. doi:10.1002/mrm.25559
4. BIC - The McConnell Brain Imaging Centre: ICBM 152 N Lin 2009. Accessed April 8, 2020. http://www.bic.mni.mcgill.ca/ServicesAtlases/ICBM152NLin2009
5. Oishi K, Chang L, Huang H. Baby brain atlases. NeuroImage. 2019;185:865-880. doi:10.1016/j.neuroimage.2018.04.003
6. Kirkpatrick S, Gelatt CD, Vecchi MP. Optimization by simulated annealing. Science. 1983;220(4598):671-680. doi:10.1126/science.220.4598.671
7. Jordan SP, Hu S, Rozada I, et al. Automated design of pulse sequences for magnetic resonance fingerprinting using physics-inspired optimization. Proc Natl Acad Sci U S A. 2021;118(40). doi:10.1073/PNAS.2020516118/-/DCSUPPLEMENTAL
8. Hu S, Jordan S, Boyacioglu R, et al. A fast MR fingerprinting simulator for direct error estimation and sequence optimization. Magn Reson Imaging. 2023;98:105-114. doi:10.1016/j.mri.2023.01.011
9. Zhao B, Setsompop K, Adalsteinsson E, et al. Improved magnetic resonance fingerprinting reconstruction with low-rank and subspace modeling. Magn Reson Med. 2018;79(2):933-942. doi:10.1002/mrm.26701
10. Lima da Cruz G, Bustin A, Jaubert O, Schneider T, Botnar RM, Prieto C. Sparsity and locally low rank regularization for MR fingerprinting. Magn Reson Med. 2019;81(6):3530-3543. doi:10.1002/mrm.27665
Figures