0565
Initial Feasibility of Free-breathing Multiparametric Mapping with Echo Planar Imaging to Derive T1, T2 and ADC Maps1Cardiovascular Innovation Research Center, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 2Department of Biomedical Engineering, Case Western Reserve University & Cleveland Clinic, Cleveland, OH, United States, 3Cardiovascular Medicine, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 4Siemens Medical Solutions USA, Inc., Cleveland, OH, United States, 5Imaging Institute, Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Quantitative Imaging, Heart
Motivation: Co-registered quantification of relevant tissue characteristics including T1, T2 and ADC has the potential to aid the diagnosis of various cardiomyopathies.
Goal(s): Our goal was to produce co-registered cardiac T1, T2 and ADC maps using free-breathing MultiParametric single shot Echo Planer Imaging (MP-EPI).
Approach: Pixel-wise value quantifications of T1, T2, and ADC were calculated and compared in a static phantom and 5 healthy subjects following respiratory motion correction.
Results: The MP-EPI technique demonstrated consistency with reference measurements (R>0.97) for T1 and T2 values, with no significant differences observed in human subjects (p>0.2), and normal ADC values.
Impact: Free breathing, co-registered multiparametric maps from EPI-based images may provide complementary information for the diagnosis and characterization of comprehensive myocardiopathies. This method has the potential to expand to include other tissue characterization in the heart, such as T2*, and CEST.
INTRODUCTION
Quantitative myocardial tissue characterization with T1 and T2 mapping and diffusion weighted imaging (DWI) offers the potential to non-invasively characterize myocardial tissue composition, such as myocardial fibrosis and acute myocardial injury1,2. Clinically, T1 and T2 maps are conventionally acquired with breath-holds, which may be difficult for patients and can lead to slice position variation due to different breath-holding positions. Methods of simultaneous T1 and T2 acquisition with/without breath holds have been proposed to provide co-registered clinical evaluation, improve patient comfort, and shorten measurement time3-4. In addition, recent advances5 in diffusion MRI have shown echo planar imaging (EPI) to be effective for free breathing acquisitions, with the use of low rank tensor motion correction (MT-MOCO). However, the lack of a combined method for assessment of all 3 clinically relevant tissue characteristics (T1, T2, and DWI) requires multiple sequences and increases scan time. Furthermore, achieving spatial correlation between these quantitative maps remains challenging due to B0 inhomogeneities and induced geometric distortion.In this study, we propose a free-breathing method to produce co-registered cardiac T1, T2 and apparent diffusion coefficient (ADC) MultiParametric mapping using single shot EPI (MP-EPI). This approach is evaluated in phantom measurements and healthy volunteers.
METHODS
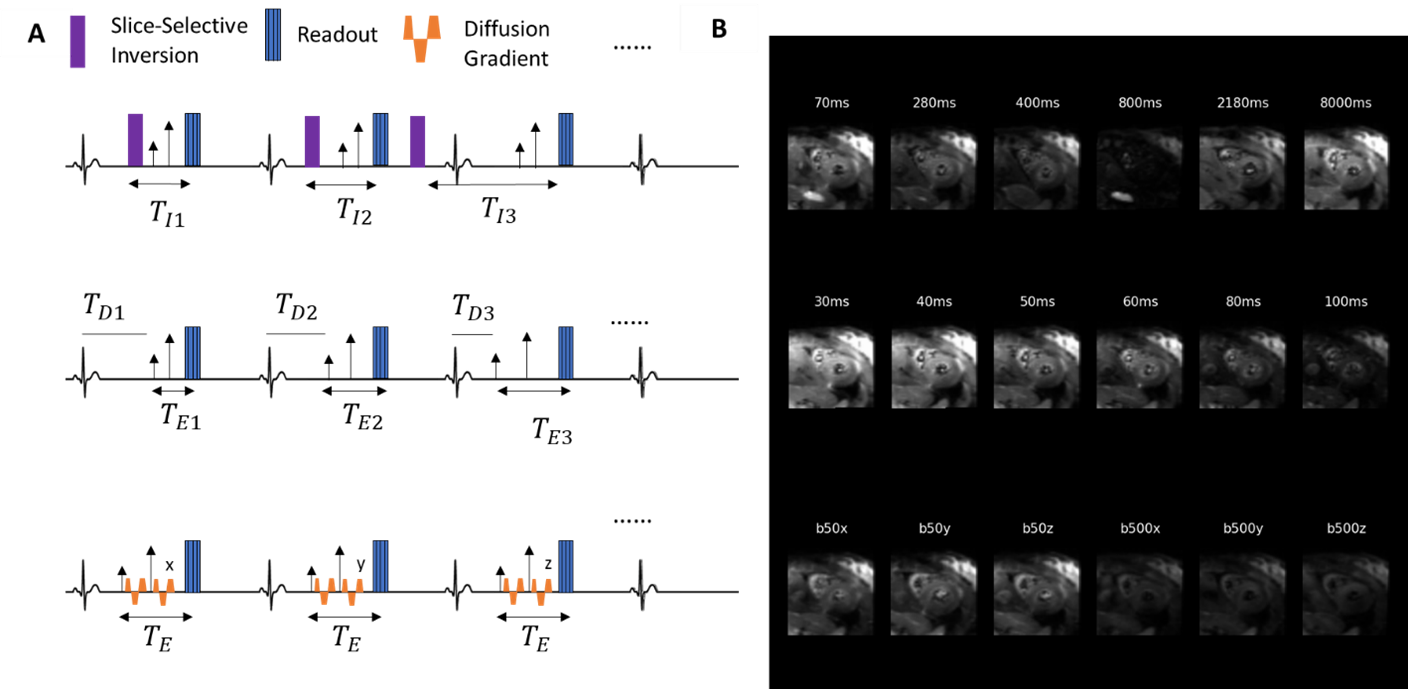
All MR imaging was performed on a 3T MR scanner (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany). In phantom experiments, inversion-recovery spin echo, and T2-weighted spin echo sequences were used to acquire reference T1 and T2 maps, respectively. 5 healthy volunteers were scanned using MP-EPI and compared with commercially available T1-MOLLI and T2-FLASH mapping (Myomaps, Siemens Healthineers AG, Erlangen, Germany) under an IRB approved protocol.The MP-EPI research sequence (2.8x2.8x8mm3, BW=2107 Hz) achieves 3 slice free breathing simultaneous T1, T2, and ADC mapping in less than 10 minutes as shown in Figure 1. Each measurement is ECG triggered to achieve imaging in end systole and employs a 2D single-shot EPI readout. The MP-EPI’s T1 mapping uses an inversion pulse and varying TI times (70-3700 ms) with fixed TE (35 ms) and b=0 s/mm2, while MP-EPI’s T2 mapping employs varying TEs (30-100 ms) and b=0 s/mm2. MP-EPI’s ADC mapping uses a B1-resistant M2 diffusion weighted spin echo sequence (TE=65 ms), with b=50, 500 s/mm2 in one average and diffusion encoding along three orthogonal directions.
Conventional retrospective respiratory motion correction (MOCO) using a mutual information optimizer was used to correct for in plane motion in T1 and T2 weighted images6 and Multitasking-based respiratory motion correction (MT-MOCO) was used in diffusion weighted images5. Pixel-wise value quantifications of T1, T2, and ADC values were calculated using custom software. A 1D grid search method from Barral7 was used to generate T1 maps, and an ordinary least squares fitting was used to fit the natural log of T2 decay. Fitting of ADC was based on the analytical equation. T1, T2, and ADC mean, and standard deviation values were calculated based on manual segmentations of the left ventricle.
RESULTS & DISCUSSION
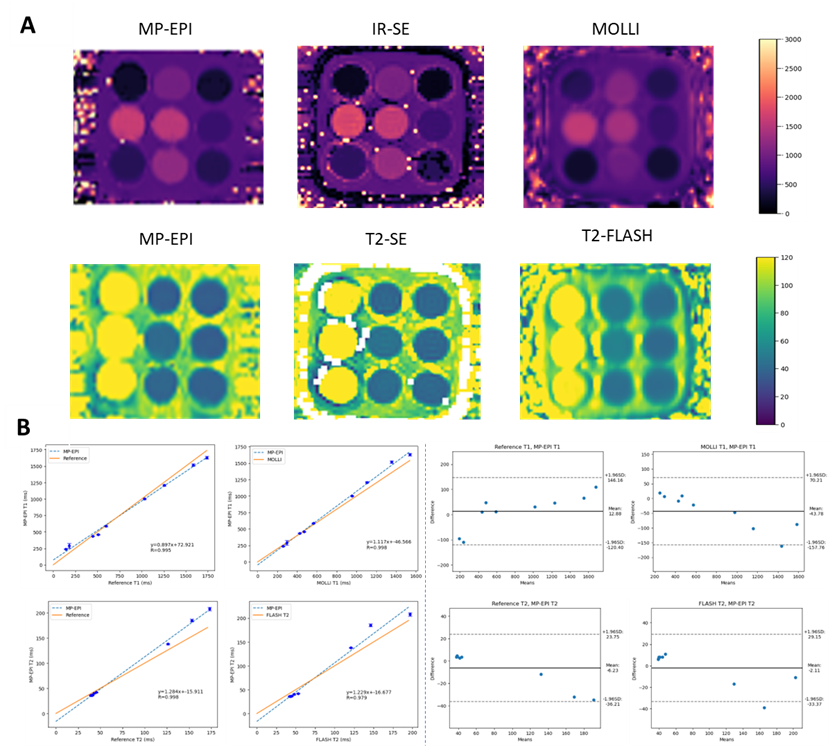
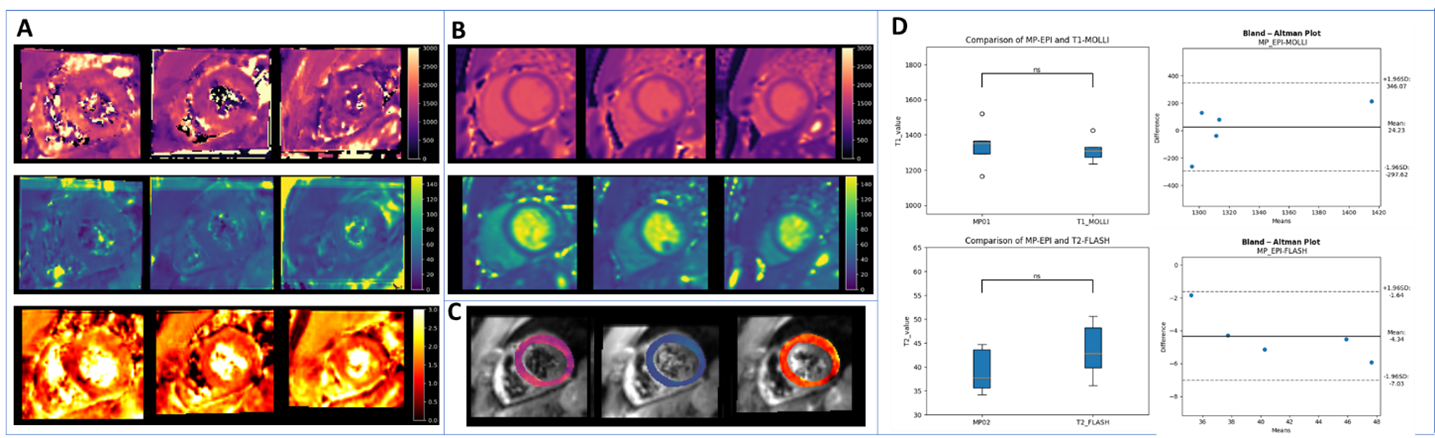
Figure 2A shows T1 and T2 maps from phantom studies. The quantitative analysis shown in figure 2B demonstrates the agreement of MP-EPI maps with the reference maps (R=0.995, 0.998 for T1 and T2, respectively) and clinical standard sequences (R=0.995, 0.978 for T1-MOLLI and T2-FLASH, respectively). Bland–Altman analyses are shown in Figure 2C, with the following limits of agreement: MP-EPI T1: ±133 ms compared with MOLLI: T1 ±226.23 ms; MP-EPI T2: ±30 ms compared with FLASH: T2 ±16.17 ms.Figure 3A and 3B shows example MP-EPI maps and T1, T2 clinic maps from a representative healthy subject. The co-registered MP-EPI maps in the mid-ventricular short axis view of the same subject are shown in Figure 3C. Based on a student’s t-test, T1 and T2 values in the myocardium were not significantly different (p=0.72,0.23) between MP-EPI (T1: 1339±115 ms, T2: 39± 4 ms) and reference values (T1: 1315±63 ms, T2: 43±5 ms), with the following limits of agreement: T1: ±321 ms; T2: ±2.7 ms (Figure 3D). ADC values were within normal range (1.510± 0.06*10-3 mm2/s) compared to literature8.
CONCLUSION
We demonstrated initial feasibility of a novel free breathing multiparametric technique (MP-EPI) capable of simultaneous T1, T2, and ADC quantification in phantom studies and healthy volunteers in less than 10 minutes. This method promotes patient comfort and has the potential to improve clinical analysis with multiple co-registered quantitative tissue characterizations.Acknowledgements
This work was partially funded by the National Institute of Health R01 HL151704, the National Institute of Health R01HL159010, and the National Institute of Health R01 HL135242.References
1. Mazur, Weronika, et al. “Diffusion-Weighted Imaging and Diffusion Tensor Imaging of the Heart in Vivo: Major Developments.” Advances in Interventional Cardiology, 2022, https://doi.org/10.5114/aic.2022.121345.
2. Moulin, Kevin, et al. “MRI of Reperfused Acute Myocardial Infarction Edema: ADC Quantification versus T1 and T2 Mapping.” Radiology, 24 Mar. 2020, p. 192186, https://doi.org/10.1148/radiol.2020192186.
3. Liu, Yu-Chi, et al. “Myocardial T1 and T2 Quantification and Water–Fat Separation Using Cardiac MR Fingerprinting with Rosette Trajectories at 3T and 1.5T.” Magnetic Resonance in Medicine, vol. 85, no. 1, 27 July 2020, pp. 103–119, https://doi.org/10.1002/mrm.28404.
4. Hermann, Ingo, et al. “Free‐Breathing Simultaneous T1, T2, and T2∗ Quantification in the Myocardium.” Magnetic Resonance in Medicine, vol. 86, no. 3, 29 Mar. 2021, pp. 1226–1240, https://doi.org/10.1002/mrm.28753.
5. Nguyen, Christopher, et al. “Free‐Breathing Diffusion Tensor MRI of the Whole Left Ventricle Using Second‐Order Motion Compensation and Multitasking Respiratory Motion Correction.” Magnetic Resonance in Medicine, vol. 85, no. 5, 30 Nov. 2020, pp. 2634–2648, https://doi.org/10.1002/mrm.28611.
6. Xue, Hui, et al. “Motion Correction for Myocardial T1 Mapping Using Image Registration with Synthetic Image Estimation.” Magnetic Resonance in Medicine, vol. 67, no. 6, 29 Aug. 2011, pp. 1644–1655, https://doi.org/10.1002/mrm.23153.
7. Barral, Joëlle K, et al. “A Robust Methodology for in Vivo T1 Mapping.” Magnetic Resonance in Medicine, vol. 64, no. 4, 1 Oct. 2010, pp. 1057–1067, https://doi.org/10.1002/mrm.22497.
8. Moulin, Kevin, et al. “In Vivo Cardiac Diffusion Imaging without Motion‐Compensation Leads to Unreasonably High Diffusivity.” Journal of Magnetic Resonance Imaging, 31 Mar. 2023, https://doi.org/10.1002/jmri.28703.
Figures