0561
Viscoelastic properties of pancreatic ductal adenocarcinoma: ex vivo biomechanical validation of in vivo MR elastography1Radiology and Nuclear Medicine, Amsterdam UMC, location AMC, Amsterdam, Netherlands, 2Imaging and Biomarkers, Cancer Center Amsterdam, Amsterdam, Netherlands, 3Radiology, Netherlands Cancer Institute, Amsterdam, Netherlands, 4Soft Tissue Engineering and Mechanobiology, Eindhoven University of Technology, Eindhoven, Netherlands, 5Endocrinology, Amsterdam Gastroenterology, Amsterdam, Netherlands
Synopsis
Keywords: Elastography, Pancreas, Elastography
Motivation: There are discrepancies in pancreatic MRE outcomes. Biomechanical validation of MRE in pancreatic ductal adenocarcinoma (PDAC) poses substantial challenges.
Goal(s): This study aims to conduct biomechanical analysis on the surgically removed specimen and correlate this to preoperative MRE outcomes.
Approach: Six PDAC patients underwent MRE prior to surgical intervention, resulting in shear wave speed (SWS) and phase angle (ф) for whole-tumor and tumor-center. Compression testing was performed on specimen at 5%-strain resulting in Young’s moduli (E). Correlation analysis was done with MRE outcomes and E.
Results: Pearson’s correlation revealed a significant correlation between SWStumor-whole and E (r(6)=.857, p=.029) and фtumor-center (r(6)=.844, p=.035).
Impact: Validation using ex vivo compression mechanical testing of pancreatic MRE outcomes gives more insight in the accuracy of the measured elastic properties in complex and inhomogeneous tumorous tissue, which is imperative for clinical application of MRE as a predictive biomarker.
Introduction
Magnetic Resonance Elastography (MRE) is a non-invasive technique to assess soft tissue viscoelastic properties.1 Pancreatic ductal adenocarcinoma (PDAC) has a poor prognosis, with 20% becoming eligible for curative surgical resection after chemotherapy.2 Recent work states that tumor stromal deposition could hinder drug delivery.3 Viscoelastic properties are hypothesized to be related to stromal deposition, therefore MRE could serve as a predictive measure for chemotherapy efficacy. A variety of MRE methodology and their reported values require biomechanical validation (through e.g. biopsies).4,5 However, this poses substantial challenges, primarily due to inaccessibility of the pancreas and the heterogeneous nature of tumors, rendering analysis on biopsies inadequate. Rheology is limited by frequency disparities with MRE, while atomic force microscopy is not sensitive to tissue macrostructure.6,7 Studies have utilized bioindentation or compression to characterize anisotropic elastic properties of tissue.8,9 This study aims to conduct biomechanical analysis on the surgically removed specimen and correlate this to preoperative MRE outcomes.Methods
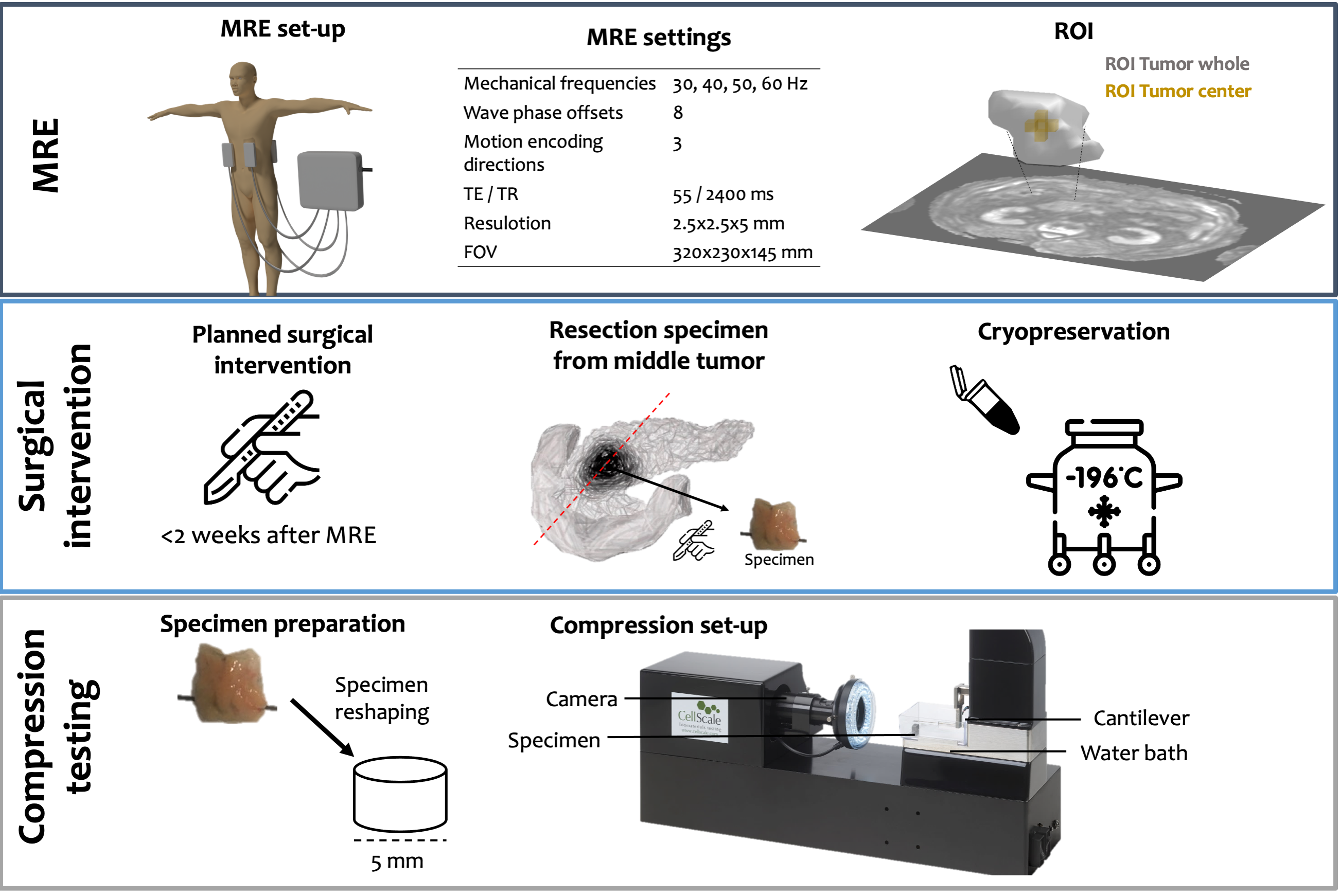
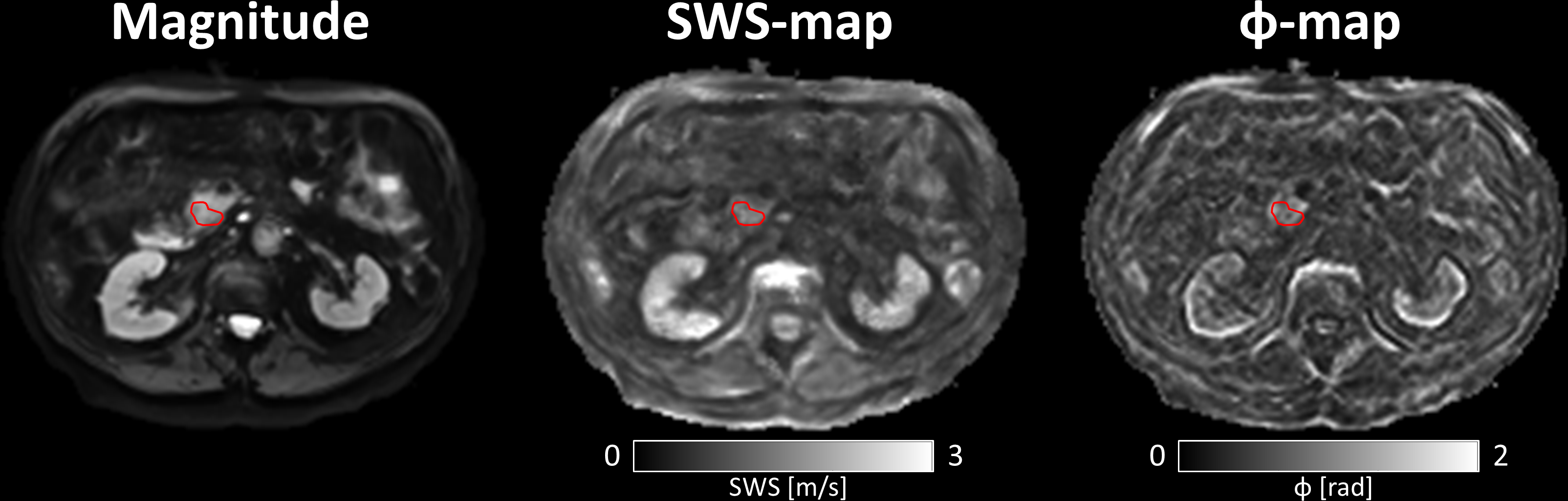
Six patients (♂=4, age=68±8 years) clinically diagnosed with PDAC and planned surgical intervention were included. MRE was scheduled <2 weeks before resection. MRE data was acquired on a 3.0T MRI scanner (Ingenia,Philips,Best,Netherlands). Patients fasted 4 hours prior to examination. Axial multi-slice multi-frequency SE-EPI MRE (Figure 1) data was acquired in free-breathing with four compressed-air transducers.10 Inversions were done using the k-MDEV algorithm, resulting in shear-wave-speed (SWS) and phase-angle (φ) maps.11 Regions-of-interest (ROI) were drawn over the pancreatic tumor on MRE magnitude images for whole-tumor and tumor-center (5-pixel kernel).After surgical intervention, two specimens were taken from the middle of the tumor, using the pancreatic duct as reference for alignment with MRE. Specimens were cryopreserved in liquid nitrogen and fixated using optimal-cutting-temperature compound. Specimens were planarized using a cryotome (Shandon Cryotome,GMI,MN,USA). Compression testing was performed with a Microtester G2 (CellScale Biomaterials,Waterloo,Canada) using parallel-plate compression and a cantilever (2mm diameter steel-rod and 5x5mm plate). Compression tests consisted of five cycles at 5% nominal-strain ($$$\epsilon$$$), as deformations at 5%-$$$\epsilon$$$ correspond with expected deformations in MRE.1 During the load phase deformation is applied with a 1% step-size. In the recovery phase the cantilever returns to the initial height. The force (F) exerted was measured through deflection of the cantilever. The area of compression (A) was approximated through the contact radius with the parallel plate.
To calculate the apparent Young’s modulus (E), Hooke’s law is fitted to the force-strain curve for the final 2.5%-$$$\epsilon$$$ in the last loading cycle ($$$\frac{\Delta\mathbf{F}/\Delta\epsilon}{A}$$$). Linear regression and Pearson's correlation was performed for whole-tumor and tumor-center data. Significance level was set at .05 and statistical analysis was done in SPSS (version28,IBM,Armonk,NY,USA).
Results
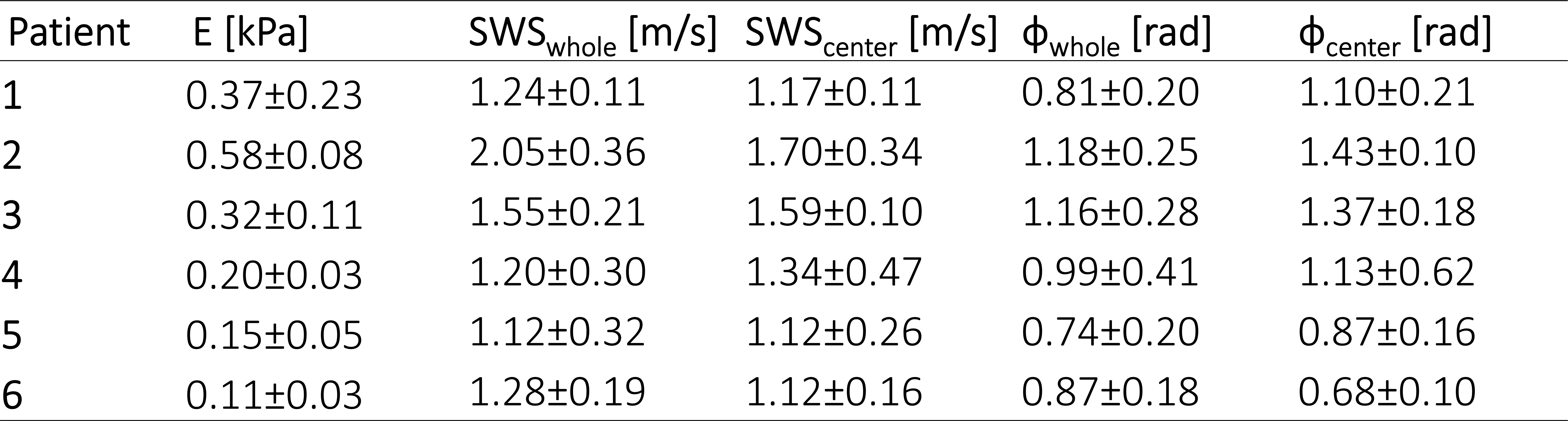
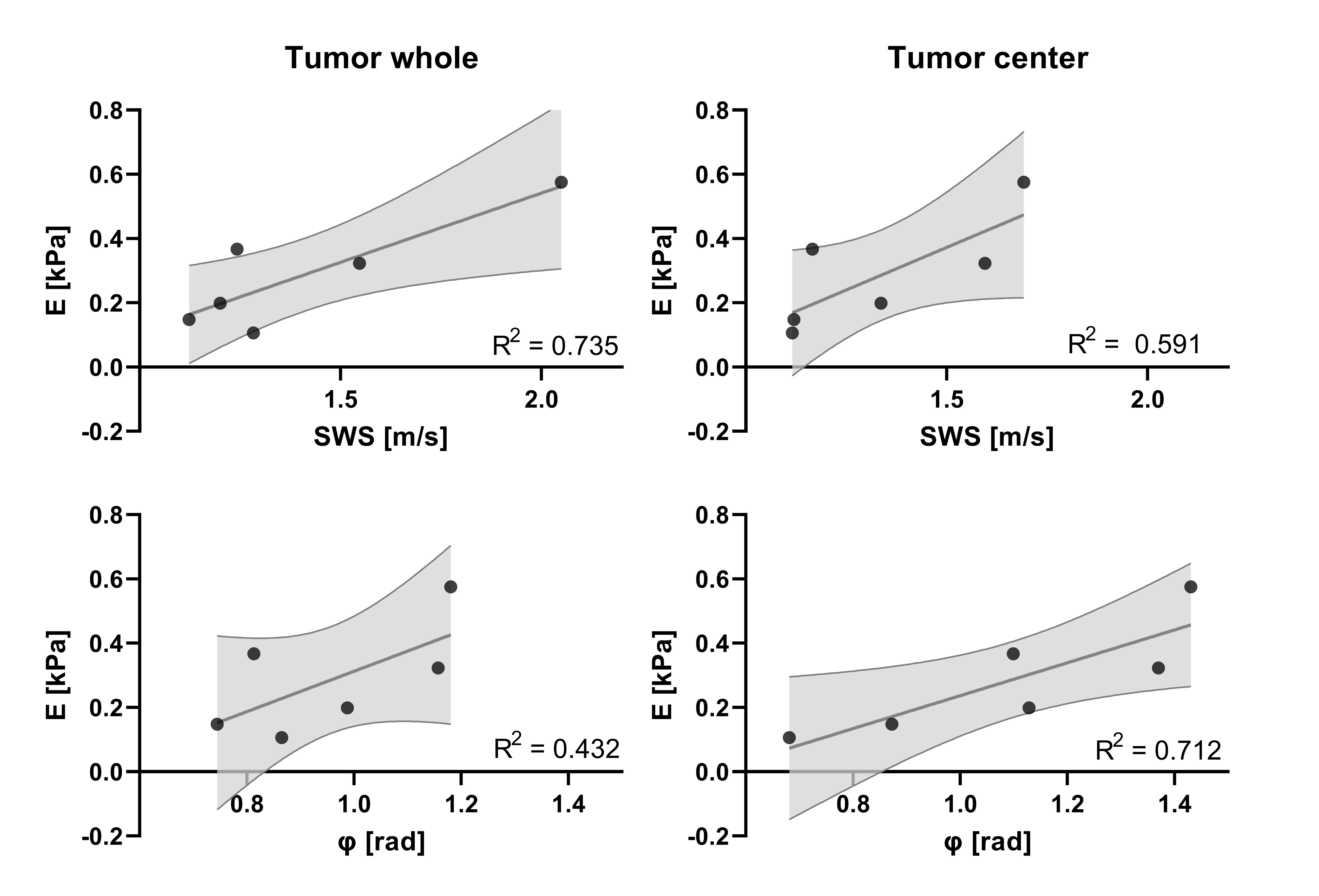
MRE parameters were SWScenter=1.34±0.25 and SWSwhole=1.41±0.35 m/s (p=.371) and фcenter=1.10±0.29 and фwhole=0.96±0.18 rad (p=.101), with example SWS- and ф-maps shown in Figure 2. An compression test is shown in Figure 3. Simple linear regression of E and SWS resulted in: slopecenter=0.53 with 95%-confidence-intervals of [-0.08-1.14] and R2=0.591, and slopewhole=0.43 [0.08-0.79] with R2=0.735. For ф the results were: slopecenter=0.51 with 95%-confidence-intervals of [0.06-0.96] and R2=0.712, and slopewhole=0.63 [-0.37-1.63] with R2=0.432, both are shown in Figure 4.Pearson’s correlation revealed a significant correlation between SWSwhole and E, but not for SWScenter (Tumor center: r(6)=.869, p=.074 and whole tumor: r(6)=.857, p=.029). Contrarily, фcenter showed significant correlation but not фwhole (Tumor center: r(6)=.844, p=.035 and whole tumor: r(6)=.657, p=.156).
Discussion & Conclusion
Pearson’s correlation showed significant correlations for фcenter and SWSwhole with E at 5%-$$$\epsilon$$$. The deviations between whole-tumor and tumor-center could be due to inhomogeneity of PDAC microenvironment.Accuracy of MRE in bovine livers and resected prostate tumors have been verified in previous studies.12,13 A linear rise of SWS with fibrosis has been shown in bovine livers and mesenteric adipose tissue, while the shear attenuation has a mild inverse correlation with inflammation.14,15
Cryopreservation has been shown to preserve biomechanical properties.16 Biological soft tissue is highly sensitive to test conditions. To overcome this, we implemented repeated measures of multiple specimens. However, there are other factors influencing complex viscoelastic behavior (e.g. lack of perfusion). Moreover, scattering caused by the vascular network in MRE influences outcomes. The small sample size and discrepancies in alignment hinder accurate comparison.
Future analysis could investigate the linear behavior at low-strain sweep as this could be potentially associated with multi-frequency MRE. Future work will involve histopathological analysis to give more insight into the underlying microenvironment.
To conclude, in vivo determined viscoelastic MRE parameters are correlated with ex vivo biomechanical properties measured by compression tests of PDAC tumors. MRE in PDAC shows the underlying elastic properties accurately, which gives impact and makes the application of MRE as a clinical tool viable.
Acknowledgements
No acknowledgement found.References
1. Manduca A, Bayly PJ, Ehman RL, et
al. MR elastography: Principles, guidelines, and terminology. Magnetic
Resonance in Medicine 2020;85:2377–2390.
2. Siegel RL, Miller
KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin
2022;72(1):7-33.
3. Wang D, Li Y, Ge
H, Ghadban T, Reeh M. The Extracellular Matrix : A Key Accomplice of Cancer
Stem Cell Migration , Metastasis Formation , and Drug Resistance in PDAC.
Cancers 2022(14):3998.
4. Kolipaka A,
Schroeder S, Mo X, Shah Z, Hart PA, Conwell DL. Magnetic resonance elastography
of the pancreas: Measurement reproducibility and relationship with age.
Magnetic Resonance Imaging 2017;42:1-7.
5. Shi Y, Glaser KJ,
Venkatesh SK, Ben-Abraham EI, Ehman RL. Feasibility of using 3D MR elastography
to determine pancreatic stiffness in healthy volunteers. Journal of Magnetic
Resonance Imaging 2015;41:369-375.
6. Jugé L, Foley P,
Hatt A, Yeung J, Bilston LE. Ex vivo bovine liver nonlinear viscoelastic
properties: MR elastography and rheological measurements. Journal of the
Mechanical Behavior of Biomedical Materials 2023;138:105638.
7. Wood CD,
Vijayvergia M, Miller FH, et al. Multi-modal magnetic resonance elastography
for noninvasive assessment of ovarian tissue rigidity in vivo. Acta Biomater
2015;13:295-300.
8. Lake SP, Barocas
VH. Mechanics and kinematics of soft tissue under indentation are determined by
the degree of initial collagen fiber alignment. Journal of the Mechanical
Behavior of Biomedical Materials 2012;13:25-35.
9. Mulk Mu.
Optimization of Indentation for the Material Characterization. In: University
W, Electronic Thesis and Dissertation Repository; 2020.
10. Dittmann F,
Tzschätzsch H, Hirsch S, Barnhill E, Braun J, Sack I, Guo J. Tomoelastography
of the abdomen: Tissue mechanical properties of the liver, spleen, kidney, and
pancreas from single MR elastography scans at different hydration states.
Magnetic Resonance in Medicine 2017;78:976-983.
11. Tzschätzsch H, Guo
J, Dittmann F, et al. Tomoelastography by multifrequency wave number recovery
from time-harmonic propagating shear waves. Medical Image Analysis
2016;30:1-10.
12. Bilston LE. Soft
tissue rheology and its implications for elastography: Challenges and
opportunities. NMR in Biomedicine 2018;31:1-10.
13. Sahebjavaher RS,
Nir G, Gagnon LO, et al. MR elastography and diffusion-weighted imaging of ex
vivo prostate cancer: quantitative comparison to histopathology. NMR Biomed
2015;28(1):89-100.
14. Sinkus R, Lambert
S, Abd-Elmoniem KZ, et al. Rheological determinants for simultaneous staging of
hepatic fibrosis and inflammation in patients with chronic liver disease. NMR
Biomed 2018;31(10):e3956.
15. van Schelt AS,
Beek KJ, Wassenaar NPM, et al. Viscoelastic properties of small bowel mesentery
at MR elastography in Crohn's disease: a prospective cross-sectional
exploratory study. Eur Radiol Exp 2023;7(1):53.
16. Lam SK, Chan SC,
Leung VY, Lu WW, Cheung KM, Luk KD. The role of cryopreservation in the
biomechanical properties of the intervertebral disc. Eur Cell Mater
2011;22:393-402.
Figures