0551
The Role of Quantitative Imaging for Early Detection of Prostate Cancer Progression in Patients on Active Surveillance1Radiation Oncology, University of Miami, Miami, FL, United States, 2Pathology, University of Miami, Miami, FL, United States, 3Radiology, University of Miami, Miami, FL, United States, 4Urology, University of Miami, Miami, FL, United States
Synopsis
Keywords: Prostate, Prostate
Motivation: Patients on Active Surveillance (AS) for prostate cancer have a high risk of cancer progression to treatment. There is a need for additional tools to risk stratify AS patients.
Goal(s): To evaluate the Habitat Risk Score (HRS) method for automatic identification of lesions for early detection of AS progressors in a prospective trial.
Approach: HRS was assessed in patients that progressed in the 1st, 2nd or 3rd year of AS.
Results: In 40% of the patients, HRS identified a dominant lesion that was not targeted during biopsy. The study illustrates the quantitative power of HRS as compared to PIRADS.
Impact: Integrating Habitat Risk Score (HRS) in Active Surveillance for prostate cancer has the potential to significantly reduce the number of surveillance biopsies. HRS facilitates the detection of progression through assignment of robust biopsy targets and quantification of tumor habitat changes.
MATERIAL AND METHODS: HRS analyzes the ADC and DCE-MRI and assigns a pixel-by-pixel score from 1 to 10 in increasing fashion with tumor aggressiveness. HRS was derived in correlation with histopathological Grade Group (GG) from radical prostatectomy.1-3
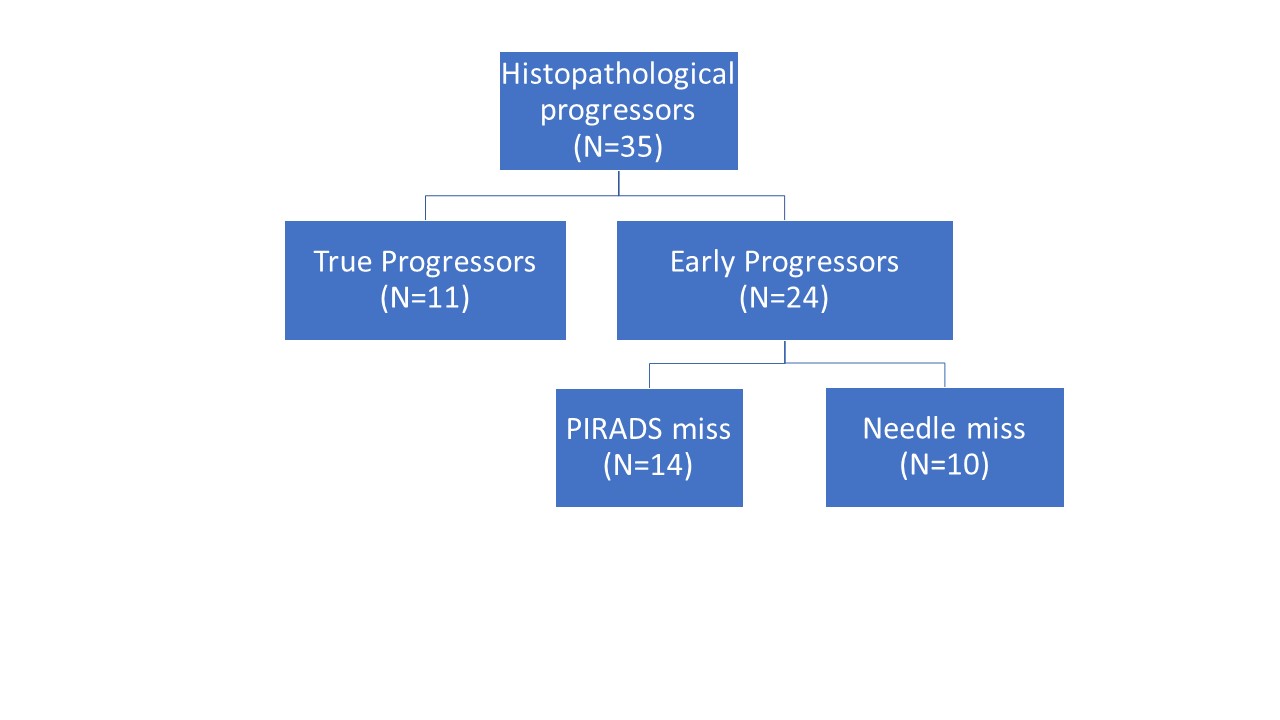
We evaluated HRS in 210 AS patients in “The Miami MAST Trial“ (ClinicalTrials.gov: NCT02242773) enrolled between 2014 and 2020. The study protocol included an mpMRI and confirmatory biopsy within 18 months of the diagnostic biopsy and every subsequent year for 36 more months, unless there was a histopathologic progression, defined as (i) more than 4 cores with any grade cancer, (ii) more than 2 cores with GG2 cancer, (iii) any single core with GG3 or higher cancer, (iv) a GG1 at diagnosis upgraded to GG2. mpMRI acquisition was consistent with the recommendations for PI-RADSv2.4 Suspicious-for-cancer regions were outlined in Dynacad (InVivo, Gainsville, FL) by a radiologist. MRI/Ultrasound (MRI-US) fusion biopsies were carried out in UroNav (InVivo, Gainsville, FL). Targeted and standard template biopsies were collected from each patient. We reviewed patients that progressed at the 1st, 2nd or 3rd year of AS. Patients were classified as “True Progressors” if: (i) the lesion(s) that resulted with a biopsy upgrade were targeted at all previous biopsy sessions; and there was evidence that (ii) the lesion(s) grew; and/or (iii) a new lesion appeared; and/or (iv) there was GG upgrade. The remaining patients were classified as “Early Progressors” when the lesion(s) that resulted in a biopsy upgrade were NOT targeted until the last session (“PIRADS miss”) or the lesion(s) were annotated for targeting in Dynacad, but it was concluded with high degree of certainty that the biopsy needle did not hit the targets (“Needle miss”).
HRS was applied and compared to: (i) radiology targets; (ii) biopsy histopathology. The volumes of HRS6-8 were recorded.
RESULTS: 35 patients progressed at 1st (n = 18); 2nd (n = 13) or 3rd year (n=4), resulting in 91 mpMRI datasets. In addition, the diagnostic scans were available for 19 patients. Thus a total of 110 mpMRI studies were analyzed: 46 were acquired on 3T Discovery MR750 (GE), 48-3T Skyra, 13-3T TrioTim and 3-1.5T Symphony (Siemens). HRS was not feasible in 17 cases due to missing sequence in the mpMRI acquisition or suboptimal ADC or DCE imaging.
In Figure 1 the imaging studies from a patient, classified as a “True progressor” are presented. Representative axial slices on T2-weighted MRI, ADC and early enhancing DCE through the lesion at Diagnostic, Confirmatory and 1st Yr imaging/biopsies are shown. The lesion, indicated with yellow arrows, was targeted at all time points, but it resulted in an upgrade (GG4) in the 1st yr. HRS indicates both the lesion’s growth and increased aggressiveness scores (HRS6 to HRS9). Using similar analysis, we identified 11 (31%) “True progressors” in the dataset. In Figure 2, the median of HRS6 to HRS9 volumes in “True Progressors” are shown at Confirmatory, 1st, and 2nd year, indicating the tumor evolution both in volume and aggressiveness.
The remaining patients were classified as “Early Progressors”. In Figure 3, an example of a patient in the “PIRADS miss” group is shown. The anterior lesion was not targeted at Confirmatory biopsy and the 1st Yr biopsy resulted in GG4 cancer. Of note, HRS clearly identified the lesion as dominant on both exams. Using similar analysis, we identified 14 (40%) “PIRADS miss” in the dataset. Assuming that HRS reduces the time of surveillance for these patients at a minimum of one year, the cumulative reduction in surveillance would be 14 years. And finally, 10 (29%) patients were identified as “Early Progressors”/Needle miss. The overall classification of the patients is shown in Figure 4.
DISCUSSION: HRS as an important tool to facilitate the targeting of the dominant lesion and quantification of tumor habitat progression. The study illustrates the power of HRS as being much more quantitative and objective, as compared to PIRADS. Currently, HRS is integrated in MRI-US fusion biopsy platform for prospective evaluation.
Acknowledgements
The research was supported by the National Cancer Institute of the National Institutes of Health under Award Number P30CA240139, RO1CA189295, R01CA190105, and U01CA239141.References
1. Stoyanova R, Chinea F, Kwon D, Reis IM, Tschudi Y, Parra NA, Breto AL, Padgett KR, Dal Pra A, Abramowitz MC, Kryvenko ON, Punnen S, Pollack A. An Automated Multiparametric MRI Quantitative Imaging Prostate Habitat Risk Scoring System for Defining External Beam Radiation Therapy Boost Volumes. Int J Radiat Oncol Biol Phys. 2018;102(4):821-9. Epub 2018/06/17. doi: 10.1016/j.ijrobp.2018.06.003. PubMed PMID: 29908220; PMCID: PMC6245650.
2. Parra NA, Pollack A, Chinea FM, Abramowitz MC, Marples B, Munera F, Castillo R, Kryvenko ON, Punnen S, Stoyanova R. Automatic Detection and Quantitative DCE-MRI Scoring of Prostate Cancer Aggressiveness. Front Oncol. 2017;7:259. doi: 10.3389/fonc.2017.00259. PubMed PMID: 29177134; PMCID: PMC5686056.
3. Tschudi Y, Pollack A, Punnen S, Ford JC, Chang YC, Soodana-Prakash N, Breto AL, Kwon D, Munera F, Abramowitz MC, Kryvenko ON, Stoyanova R. Automatic Detection of Prostate Tumor Habitats using Diffusion MRI. Sci Rep. 2018;8(1):16801. Epub 2018/11/16. doi: 10.1038/s41598-018-34916-4. PubMed PMID: 30429515; PMCID: PMC6235961.
4. Barentsz JO, Weinreb JC, Verma S, Thoeny HC, Tempany CM, Shtern F, Padhani AR, Margolis D, Macura KJ, Haider MA, Cornud F, Choyke PL. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur Urol. 2016;69(1):41-9. Epub 2015/09/12. doi: 10.1016/j.eururo.2015.08.038. PubMed PMID: 26361169; PMCID: PMC6364687.
Figures
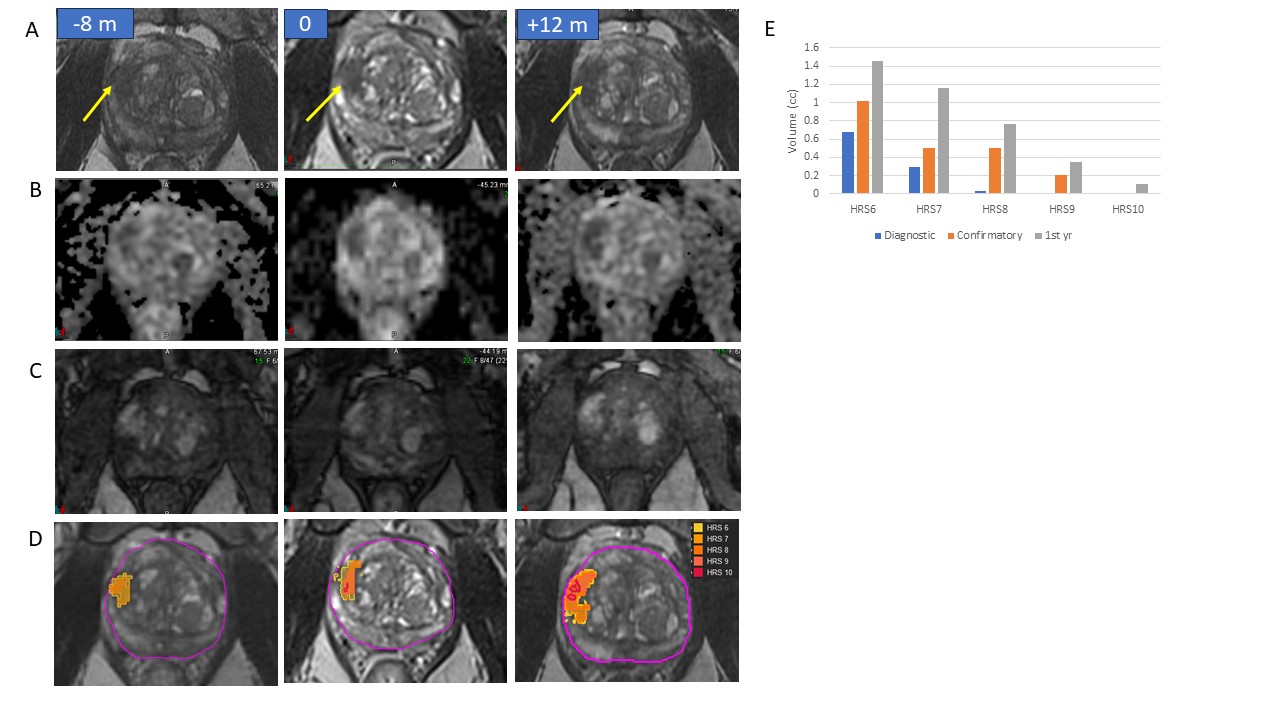
Figure 1: Imaging and HRS analysis of patient on AS, classified as “true progressor” (A, B, C) Representative axial slices on T2w, ADC and early enhancing DCE with a lesion (yellow arrow) on Diagnostic (-8 m), Confirmatory (0 m) and 1st Yr (+12 m) biopsy session. The lesion was Gleason 6 cancer @ -8 mo and 0 mo and Gleason 4+5 at 1st year (progression); (D) HRS depiction of the lesion on the same slice; (E) Quantitative HRS maps depict the lesion evolution in terms of volume and aggressiveness.
Acquired on Discovery MR750 [-8m;+12m] and TrioTim [0m]
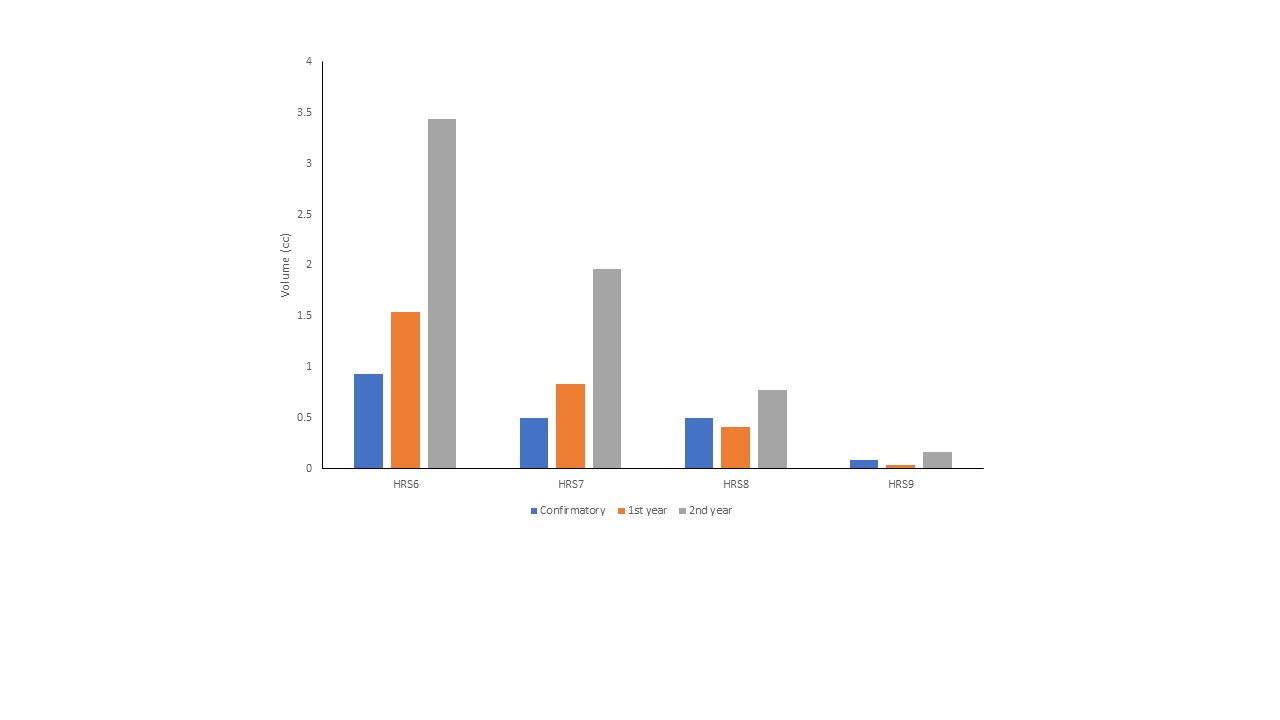
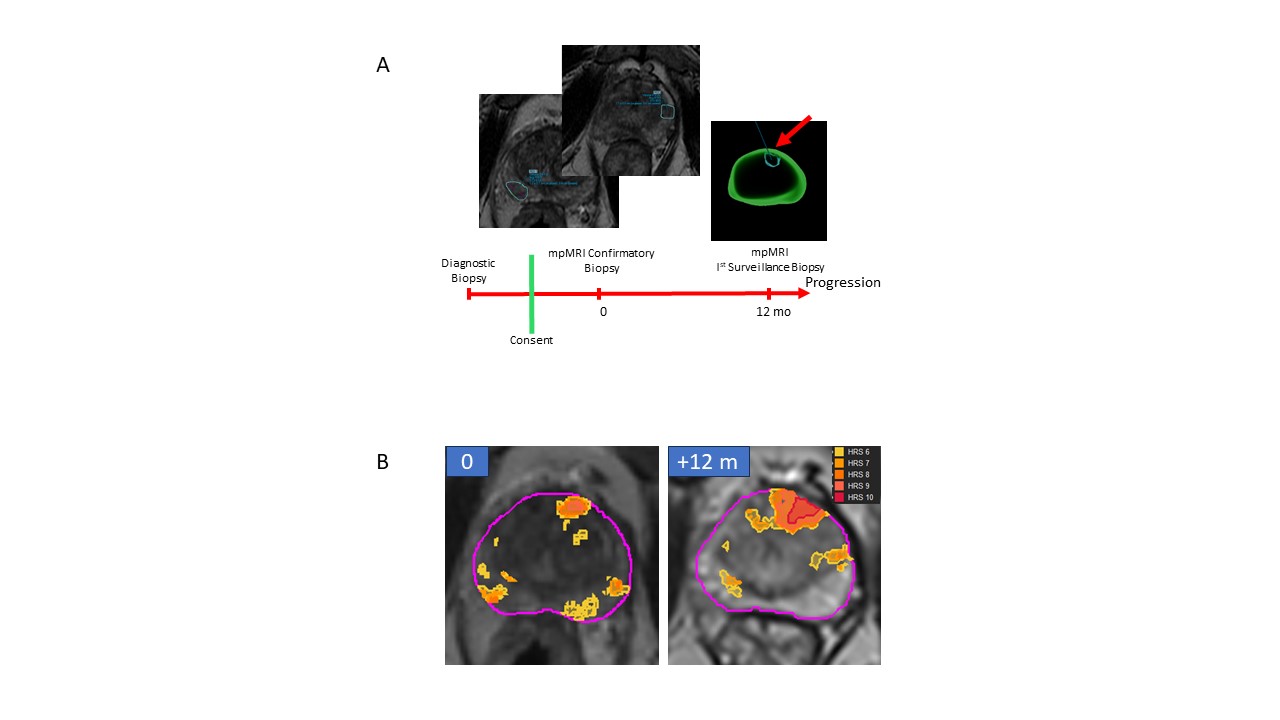
Figure 3: PIRADS lesions and HRS analysis of patient on AS, classified as “Early progressor”/PIRADS miss (A) At Confirmatory biopsy two lesions in the Peripheral Zone (PZ) were marked. All targeted and systematic biopsies from this session were negative. At 12 m biopsy, the anterior lesion was marked in that resulted in GG4; (B) HRS reveals that the anterior lesion is depicted as the dominant lesion at both 0/12m. Note that there are also HRS detections in PZ coinciding with the PIRADS lesions. HRS@12m also demonstrates increased volume.
Acquired on Discovery MR750 [0m] and TrioTim [12m]